





Sir,
On many occasions dialysis is initiated with a temporary jugular venous catheter which is later exchanged for a permanent tunnelled venous catheter, pending creation of an arteriovenous fistula. The exchange of catheter over a guide wire is usually a low-risk procedure and in uncomplicated cases, a chest radiograph is not warranted [ 1 , 2 ]. Cardiac tamponade is a rare complication following initial insertion of a central vein catheter via the Seldinger technique. We report a case of cardiac tamponade, following routine exchange of a temporary jugular catheter to a permanent tunnelled catheter.
A 56-year-old man with advanced renal failure secondary to diabetic nephropathy presented with pulmonary oedema. On the 10th day of admission, his temporary right internal jugular catheter was changed for a permanent tunnelled catheter. The procedure was performed by an experienced practitioner. The procedure was uneventful, although a straight guide wire was used after initial difficulty passing a J-tipped guide wire. Two hours after the procedure the patient became hypotensive, blood pressure fell to 60 mmHg systolic. The jugular venous pressure was not elevated, and heart sounds were normal. There was no evidence of pneumothorax and portable chest radiograph did not demonstrate an obvious cause for his clinical condition ( Figure 1 ). Emergency CT scan was requested as an occult vascular injury was suspected. This identified a large pericardial effusion ( Figure 2 ). Pericardiocentesis was performed, with 400 ml of blood stained fluid drained. The patient's blood pressure improved immediately following this procedure. The tunnelled haemodialysis catheter remained functional. The patient continues on maintenance dialysis and has not required further hospitalization.
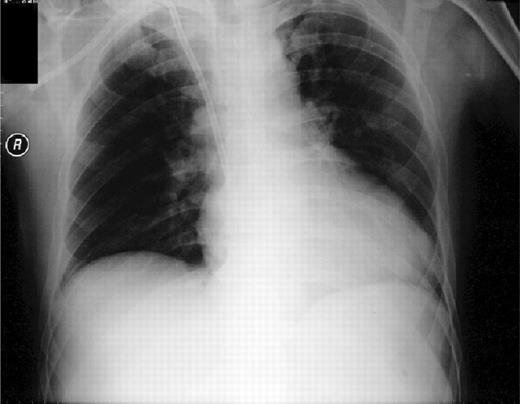
Portable chest radiograph.
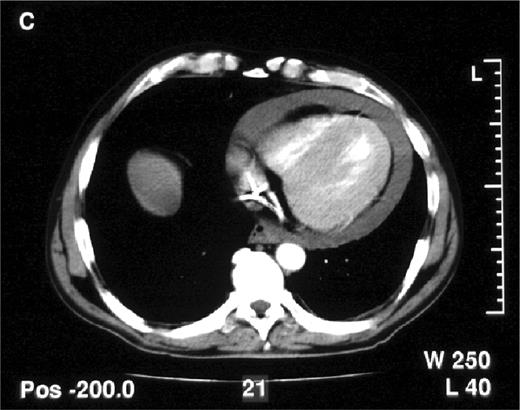
CT demonstrating pericardial effusion and catheter artefact.
Pericardial tamponade is thought to arise when dilator, cannula or guidewire punctures the myocardial wall [ 3 , 4 ]. This case illustrates that this complication can also arise when catheters are exchanged over a guide wire. In this patient, the initial difficulty experienced trying to pass a J-tipped guide wire led to the use of a straight wire. For practical reasons, the majority of central venous catheters are placed without real-time radiological screening. The position of the guide wire is estimated by the operator. Guide wires with distance markers may improve the operator's awareness of the distance advanced in a central vein and reduce the risk of accidental myocardial injury. Chest radiography is often unhelpful, as in this case, in confirming or refuting a diagnosis of pericardial tamponade. Echocardiography is the primary imaging modality for suspected cardiac tamponade. CT scan or MRI may be more useful if major vessel injury is suspected.
More widespread use of graduated guide wires could reduce the risk of cardiac tamponade by improving operator's awareness of how far the guide wire tip has been advanced.
Conflict of interest statement . None declared.
References
Frassinelli P, Pasquale MD, Cipolle MD, Rhodes M. Utility of chest radiographs after guidewire exchanges of central venous catheters.
Amshell CE, Pulesty JA, Dudrick SJ. Are chest X-rays mandatory following central venous recatheterisation over a wire?.
Yilmazlar A, Bilgin M, Korfuli G, Grem A, Ozkan U. Complications of 1303 central venous cannulations.


{kind=link}
{kind=link}
Comments