





Abstract
Aims To examine the heritability of atrial fibrillation (AF) in Icelanders, utilizing a nationwide genealogy database and population-based data on AF. AF is a disorder with a high prevalence, which has been known to cluster in families, but the heritability of the common form has not been well defined.
Methods and results The study population included 5269 patients diagnosed since 1987 and age-sex-matched controls randomly selected from the genealogy database. Kinship coefficients (KC), expressed as genealogical index of familiality (GIF=average KC×100 000), were calculated before and after exclusion of relatives separated by one to five meiotic events. Risk ratios (RR) were calculated for first- to fifth-degree relatives. The average pairwise GIF among patients with AF was 15.9 (mean GIF for controls 13.9, 95%CI=13.3, 14.4); this declined to 15.4 (mean GIF for controls 13.6, 95%CI=13.1, 14.2) after exclusion of relatives separated by one meiosis and to 13.7 (mean GIF for controls 12.6, 95%CI=12.1, 13.2), 12.7 (mean GIF for controls 11.9, 95%CI=11.4, 12.4), and 11.3 (mean GIF for controls 10.6, 95%CI=10.1, 11.1) after exclusion of relatives within two, three, and four meioses, respectively (all P<0.00001). RRs among relative pairs also declined incrementally, from 1.77 in first-degree relatives to 1.36, 1.18, 1.10, and 1.05 in second- through fifth-degree relatives (all P<0.001), consistent with the declining proportion of alleles shared identically by descent. When the analysis was limited to subjects diagnosed with AF before the age of 60, first-degree relatives of the AF cases were nearly five times more likely to have AF than the general population.
Conclusion AF shows strong evidence of heritability among unselected patients in Iceland, suggesting that there may be undiscovered genetic variants underlying the risk of the common form of AF.
Introduction
Atrial fibrillation (AF) is a common arrhythmia associated with increased mortality and significant morbidity.1,2 As AF is primarily a disease of the elderly, its prevalence is expected to increase with the advancing age of Western populations.3 Multiple risk factors have been implicated, including hypertension, coronary artery disease, and elevated CRP.4,5 However, AF is known to occur in the absence of these conditions6 and there is some evidence of familial clustering,7 suggesting a genetic component to the risk of the disease, especially in patients with lone AF.
Although a few studies have identified Mendelian variants in selected families, which increase susceptibility to AF,8–11 none has yet uncovered variants that underlie the common form of the disease. A recent report from the Framingham Study described increased risk in offspring of patients with AF, but only parent/offspring risk was assessed and the number of offspring cases was small.12 Demonstration of familial clustering in unselected families is an important first step towards the study of genetic contribution to the risk of the common form of AF.
Icelanders are relatively homogeneous with respect to both genetic and environmental factors, they have an accessible health-care system and extensive genealogical records covering the entire nation,13 all features that render population-wide heritability studies of conditions such as AF feasible. In this study, these resources were leveraged to address the following objectives: (i) to compare the degree of relatedness of AF patients to a random population sample by assessing the kinship coefficient (KC); (ii) to assess the risk ratio (RR) of AF among relatives at varying degrees of genetic distance; and (iii) to determine the strength and consistency of these risk relationships in AF patients above and below the age of 60 at the time of diagnosis.
Methods
Patients
All patients diagnosed with AF at the Landspitali University Hospital from 1987 to 2003, the only tertiary referral centre in Iceland and the only hospital in Reykjavik (where two-thirds of the population resides), were included in this study. Diagnoses were confirmed by a 12-lead electrocardiogram demonstrating no P waves and irregularly irregular R–R intervals. All electrocardiograms were manually read by a cardiologist. All AF cases diagnosed during the time period were included regardless of whether the patients had clinical symptoms or not. Although detailed phenotypic information was not available for the cohort, we stratified patients on the basis of age <60 or ≥60 years at the time of diagnosis of AF. This was done because some include in their definition of lone AF an age limit <60 years,6 whereas others do not include an age limit in their definition.14 It has been demonstrated that the prevalence of heart disease in Iceland increases substantially after the age of 60.15,16 Given this, individuals under the age of 60 at the time of diagnosis are more likely to have lone AF than those over the age of 60. Thus, dividing the group in this way might give an idea of the potential heritability of lone AF vs. AF associated with organic heart disease, although this clearly relies on some assumptions. The data currently do not allow further subclassification of the arrhythmia as paroxysmal, persistent, or permanent.
The study protocol was approved by the National Bioethics Committee of Iceland and the Icelandic Data Protection Authority.
Genealogical database
The Icelandic genealogy database contains records on 716 000 individuals, more than half the adult population of Iceland since the settlement of the island more than 11 centuries ago.17 It includes all living Icelanders, more than 284 000 individuals, and a large proportion of their ancestors back to 930 AD.13 This allows investigation of various levels of relatedness among patients as well as recruitment of population-based control groups.17
According to studies based on Y-chromosome and mitochondrial polymorphisms, 75% of males who settled in Iceland were Norwegian and 66% of females were Celtic.18–20 Although the island has been relatively isolated since its settlement, autosomal recessive disorders, which are frequently seen in inbred populations, have not been prevalent in Iceland.
Assessment of inheritance
The average pairwise KC was calculated for AF patients and compared to the distribution of the average KC for a set of controls matched one to one for sex, year of birth (5-year strata), and numbers of ancestors in the genealogy database five generations back. KC is the probability that two randomly selected alleles at an autosomal locus, one from each individual, are inherited from a common ancestor.21 KCs were refined by excluding the contribution by close relatives, as these are more likely to share the environment and may dominate the results22 and the resulting values were compared to the distribution of values of 100 000 matched control groups. In this study, a control group refers to a sample selected randomly from our genealogy database of individuals matching the patients in sex, year of birth (rounded to 5 years), and connectivity in the genealogy database (same number of ancestors five generations back). These control groups are not ascertained for any phenotype, and we use between 10 000 and 100 000 randomly chosen such control groups. They serve the purpose of estimating confidence intervals for the RR and KC estimates, respectively, not in obtaining the estimates for RR and KC themselves. KCs were expressed as genealogical index of familiality (GIF=average KC×100 000).23
The RR for relatives of affected patients was defined as the risk of the disease in the relatives divided by the risk in the general population. This ratio is directly related to the power to map susceptibility genes.24 Obtaining valid estimates of the RR are not straightforward because many sampling schemes and inappropriate estimators can lead to biased or inflated estimates.25,26 The use of population-based groups of patients eliminates much of the potential sampling bias, and a near-complete genealogy database facilitates identification of patients related to other patients. From the distribution of RR calculated for 10 000 matched controls sets,22 95%CIs were estimated. Heritability was also assessed separately for AF patients aged <60 and ≥60 at the time of the diagnosis of arrhythmia. For both KCs and RRs, a P-value of <0.05 was considered significant.
The software used for familiality calculations was developed at deCODE.26
Results
A total of 5269 patients were diagnosed with AF during the study period, and of those, 914 (17.3%) were under 60 years at the time of diagnosis of AF. The mean age of patients was 71.6 years (SD=13.6). There were 3110 (59%) males and 2159 (41%) females. Eighty per cent of patients (n=4195) were related within four meioses to another patient, with the four largest family clusters including 728, 130, 114, and 107 patients. Figure 1 shows a representative cluster of AF patients in one of the affected families.
GIF values were higher among AF patients than among controls, including when relatives within six or less meioses were excluded (Table 1); all P<0.00001 except when excluding relatives within six meioses (P=0.00003). GIFs for AF patients diagnosed at age <60 were also higher than for controls, with P<0.00001 for GIFs with none or first-level relatives removed and maintained significance until fifth or higher level relations were excluded. Results for AF patients aged ≥60 were similar to those for the full cohort.
First-degree relatives of AF patients were 1.77-fold more likely to have AF than the general population (Table 2). RRs declined incrementally by degree of relationship (but remained significantly above 1.0) in second- through fifth-degree relatives, consistent with the proportion of alleles shared identically by descent.
First-degree relatives of patients <60 years of age were more than four-fold (RR=4.67) more likely to have AF at age <60 than the general population. Second-degree relatives of those patients were also more likely to have AF at age <60 than the general population. More distant relatives demonstrated the same pattern but there is not sufficient power in the study to claim significance. For those diagnosed at the age ≥60, the RR was greater than 1.0 for all relatives, although this did not reach statistical significance for fourth- and fifth-degree relatives and again declined incrementally, with excess risk falling by about a factor of 2 with each diminishing degree of relatedness.
Discussion
This population-based cohort of over 5000 patients with AF shows significant familial clustering by two robust analytic methods, KC and RR, strongly suggesting a familial basis for the condition. This observation extends well beyond second-degree relatives (grandparents/grandchildren, aunts/uncles, nephews/nieces, half-siblings), suggesting that the impact of the common home environment is likely to be small.27
To our knowledge, only one other population-based cohort of AF cases has been used to estimate heritability of the condition and that focused exclusively on parent–offspring RRs.12 Ascertainment of parent–offspring risk of AF is complicated in most contemporary studies by the difficulties of ascertaining late-onset disease in previous generations. The Framingham Heart Study solved this problem by having essentially complete, prospective ascertainment of AF among both parents and offspring.2 The current study solved this by using recent diagnoses among contemporaries and using a genealogy database to link them through familial relationships to a number of previous generations.13
We observed an exponential decline in RR by degree of relatedness, consistent with diminishing proportion of alleles shared identically by descent. Evidence of a graded association such as this is considered to be among the strongest of the epidemiological criteria for causal inferences.28 The Icelandic data are unique in permitting reliable assessment of RRs at such distant levels of relatedness.
Although patients diagnosed at an age of <60 comprised only 17% of the sample, evidence of heritability was stronger in the younger group, at least among more closely related persons. This might imply that (i) the genetics of AF in patients aged ≥60 is more complex and different from those under 60; (ii) lone AF is not representative of common AF in its familial clustering; or (iii) the sample size of the cohort <60 years of age is insufficient to demonstrate all but the strongest risks. This supports the value of examining heritability on a population basis, with a broad definition of phenotype.
The present study has several limitations, most notably a lack of detailed information on other risk factors for AF and the lack of categorization of the subtype of AF. The results, nevertheless, strongly suggest that genetic factors contribute to the risk of all AF. The heritability of hypertension and coronary artery disease, both known risk factors for AF, has also been well documented, and the possibility that these risk factors underlie, at least in part, the familial clustering observed for AF obviously has to be considered. The aetiology of AF is likely multi-factorial, with a number of cardiovascular comorbidities known to increase the risk of AF. It is also well known that AF can occur in those with no demonstrable heart disease. The limitations to the data presented here need to be addressed in future studies with detailed phenotyping of the cohort.
Although other investigators have mainly focused on lone AF in familial studies,7–11 our previous work in myocardial infarction29 and stroke30 lends additional support to the value of initial studies using broadly defined phenotypes in the context of our genealogy database. In both diseases, an initial approach with a broad phenotype has led to discoveries of genes that confer risk of myocardial infarction and stroke.29,30 Thus, we anticipate that our AF studies may also offer a novel insight into the pathogenesis of AF and point towards new therapeutic possibilities.
The substantial population burden of undifferentiated AF, which is expected to increase significantly in the coming years,3 underscores the need for exploration of a broadly defined phenotype. Indeed, the results presented in this study using a broad phenotype indicate a familial component to the common form of AF. As the results of the pharmacological therapy for AF are somewhat unsatisfactory and access to ablative therapy limited, exploring new therapeutic options for this common disorder is important. Further understanding of the molecular mechanisms of AF is crucial in developing new strategies in dealing with the significant public health burden caused by the disease. Detailed phenotyping of the cohort and linkage analysis in search of AF susceptibility genes are necessary steps to further understand the genetic contribution to the common form of AF.
In conclusion, we have demonstrated substantial familial aggregation of AF in Iceland and strong likelihood of heritability among unselected AF patients, suggesting that there may be undiscovered genetic variants underlying the risk of the common form of AF. The observation that these results relate to both younger patients and those over 60 years of age indicates that these results might be generalizeable to all AF populations.
Acknowledgement
The authors would like to thank Dr Augustine Kong for his important contribution to the manuscript.
Conflict of interest: D.O.A. and T.A.M. have declared that no competing interests exist. G.T., S.T., K.K., H.H., and K.S. have stock in deCODE genetics.
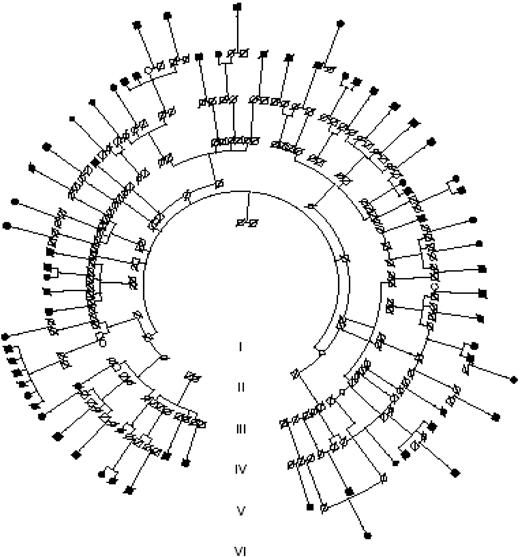
Figure 1 A large representative pedigree showing 69 patients with AF. Filled circles represent affected females and filled squares affected males. Slash marks denote family members listed in the local death registry. The AF patients presented could be traced to common ancestors less than or equal to six previous generations.
GIF in AF patients and matched controls, before and after exclusion of relatives separated less than or equal to one to six meiotic events
| Relations removed | Mean GIF, patients | Mean GIF (95%CI), controls | P-value |
|---|---|---|---|
| All AF | |||
| None | 15.9 | 13.9 (13.3, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.1, 14.2) | <0.00001 |
| ≤2 meioses | 13.7 | 12.6 (12.1, 13.2) | <0.00001 |
| ≤3 meioses | 12.7 | 11.9 (11.4, 12.4) | <0.00001 |
| ≤4 meioses | 11.3 | 10.6 (10.1, 11.1) | <0.00001 |
| ≤5 meioses | 10.2 | 9.6 (9.1, 10.1) | <0.00001 |
| ≤6 meioses | 8.7 | 8.2 (7.7, 8.6) | 0.00003 |
| AF at age <60 | |||
| None | 13.6 | 9.6 (8.2, 11.0) | <0.00001 |
| ≤1 meiosis | 12.7 | 9.5 (8.1, 10.8) | <0.00001 |
| ≤2 meioses | 10.0 | 8.8 (7.6, 9.9) | 0.00004 |
| ≤3 meioses | 9.0 | 8.3 (7.3, 9.3) | 0.0057 |
| ≤4 meioses | 7.6 | 7.2 (6.3, 8.0) | 0.027 |
| ≤5 meioses | 6.4 | 6.3 (5.5, 7.0) | 0.17 |
| ≤6 meioses | 5.2 | 5.0 (4.3, 5.6) | 0.089 |
| AF at age ≥60 | |||
| None | 15.7 | 13.8 (13.1, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.0, 14.2) | <0.00001 |
| ≤2 meioses | 13.4 | 12.3 (11.8, 12.9) | <0.00001 |
| ≤3 meioses | 12.6 | 11.4 (11.2, 12.3) | <0.00001 |
| ≤4 meioses | 10.9 | 10.3 (9.8, 10.8) | <0.00001 |
| ≤5 meioses | 9.9 | 9.4 (8.9, 9.9) | 0.00007 |
| ≤6 meioses | 8.2 | 7.8 (7.3, 8.3) | 0.00037 |
| Relations removed | Mean GIF, patients | Mean GIF (95%CI), controls | P-value |
|---|---|---|---|
| All AF | |||
| None | 15.9 | 13.9 (13.3, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.1, 14.2) | <0.00001 |
| ≤2 meioses | 13.7 | 12.6 (12.1, 13.2) | <0.00001 |
| ≤3 meioses | 12.7 | 11.9 (11.4, 12.4) | <0.00001 |
| ≤4 meioses | 11.3 | 10.6 (10.1, 11.1) | <0.00001 |
| ≤5 meioses | 10.2 | 9.6 (9.1, 10.1) | <0.00001 |
| ≤6 meioses | 8.7 | 8.2 (7.7, 8.6) | 0.00003 |
| AF at age <60 | |||
| None | 13.6 | 9.6 (8.2, 11.0) | <0.00001 |
| ≤1 meiosis | 12.7 | 9.5 (8.1, 10.8) | <0.00001 |
| ≤2 meioses | 10.0 | 8.8 (7.6, 9.9) | 0.00004 |
| ≤3 meioses | 9.0 | 8.3 (7.3, 9.3) | 0.0057 |
| ≤4 meioses | 7.6 | 7.2 (6.3, 8.0) | 0.027 |
| ≤5 meioses | 6.4 | 6.3 (5.5, 7.0) | 0.17 |
| ≤6 meioses | 5.2 | 5.0 (4.3, 5.6) | 0.089 |
| AF at age ≥60 | |||
| None | 15.7 | 13.8 (13.1, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.0, 14.2) | <0.00001 |
| ≤2 meioses | 13.4 | 12.3 (11.8, 12.9) | <0.00001 |
| ≤3 meioses | 12.6 | 11.4 (11.2, 12.3) | <0.00001 |
| ≤4 meioses | 10.9 | 10.3 (9.8, 10.8) | <0.00001 |
| ≤5 meioses | 9.9 | 9.4 (8.9, 9.9) | 0.00007 |
| ≤6 meioses | 8.2 | 7.8 (7.3, 8.3) | 0.00037 |
GIF in AF patients and matched controls, before and after exclusion of relatives separated less than or equal to one to six meiotic events
| Relations removed | Mean GIF, patients | Mean GIF (95%CI), controls | P-value |
|---|---|---|---|
| All AF | |||
| None | 15.9 | 13.9 (13.3, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.1, 14.2) | <0.00001 |
| ≤2 meioses | 13.7 | 12.6 (12.1, 13.2) | <0.00001 |
| ≤3 meioses | 12.7 | 11.9 (11.4, 12.4) | <0.00001 |
| ≤4 meioses | 11.3 | 10.6 (10.1, 11.1) | <0.00001 |
| ≤5 meioses | 10.2 | 9.6 (9.1, 10.1) | <0.00001 |
| ≤6 meioses | 8.7 | 8.2 (7.7, 8.6) | 0.00003 |
| AF at age <60 | |||
| None | 13.6 | 9.6 (8.2, 11.0) | <0.00001 |
| ≤1 meiosis | 12.7 | 9.5 (8.1, 10.8) | <0.00001 |
| ≤2 meioses | 10.0 | 8.8 (7.6, 9.9) | 0.00004 |
| ≤3 meioses | 9.0 | 8.3 (7.3, 9.3) | 0.0057 |
| ≤4 meioses | 7.6 | 7.2 (6.3, 8.0) | 0.027 |
| ≤5 meioses | 6.4 | 6.3 (5.5, 7.0) | 0.17 |
| ≤6 meioses | 5.2 | 5.0 (4.3, 5.6) | 0.089 |
| AF at age ≥60 | |||
| None | 15.7 | 13.8 (13.1, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.0, 14.2) | <0.00001 |
| ≤2 meioses | 13.4 | 12.3 (11.8, 12.9) | <0.00001 |
| ≤3 meioses | 12.6 | 11.4 (11.2, 12.3) | <0.00001 |
| ≤4 meioses | 10.9 | 10.3 (9.8, 10.8) | <0.00001 |
| ≤5 meioses | 9.9 | 9.4 (8.9, 9.9) | 0.00007 |
| ≤6 meioses | 8.2 | 7.8 (7.3, 8.3) | 0.00037 |
| Relations removed | Mean GIF, patients | Mean GIF (95%CI), controls | P-value |
|---|---|---|---|
| All AF | |||
| None | 15.9 | 13.9 (13.3, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.1, 14.2) | <0.00001 |
| ≤2 meioses | 13.7 | 12.6 (12.1, 13.2) | <0.00001 |
| ≤3 meioses | 12.7 | 11.9 (11.4, 12.4) | <0.00001 |
| ≤4 meioses | 11.3 | 10.6 (10.1, 11.1) | <0.00001 |
| ≤5 meioses | 10.2 | 9.6 (9.1, 10.1) | <0.00001 |
| ≤6 meioses | 8.7 | 8.2 (7.7, 8.6) | 0.00003 |
| AF at age <60 | |||
| None | 13.6 | 9.6 (8.2, 11.0) | <0.00001 |
| ≤1 meiosis | 12.7 | 9.5 (8.1, 10.8) | <0.00001 |
| ≤2 meioses | 10.0 | 8.8 (7.6, 9.9) | 0.00004 |
| ≤3 meioses | 9.0 | 8.3 (7.3, 9.3) | 0.0057 |
| ≤4 meioses | 7.6 | 7.2 (6.3, 8.0) | 0.027 |
| ≤5 meioses | 6.4 | 6.3 (5.5, 7.0) | 0.17 |
| ≤6 meioses | 5.2 | 5.0 (4.3, 5.6) | 0.089 |
| AF at age ≥60 | |||
| None | 15.7 | 13.8 (13.1, 14.4) | <0.00001 |
| ≤1 meiosis | 15.4 | 13.6 (13.0, 14.2) | <0.00001 |
| ≤2 meioses | 13.4 | 12.3 (11.8, 12.9) | <0.00001 |
| ≤3 meioses | 12.6 | 11.4 (11.2, 12.3) | <0.00001 |
| ≤4 meioses | 10.9 | 10.3 (9.8, 10.8) | <0.00001 |
| ≤5 meioses | 9.9 | 9.4 (8.9, 9.9) | 0.00007 |
| ≤6 meioses | 8.2 | 7.8 (7.3, 8.3) | 0.00037 |
RR in relatives of AF patients, by degree of relationship, for all AF and stratified by age <60 or ≥60
| Degree of relatives | Risk ratio (95%CI) | P-value |
|---|---|---|
| All AF | ||
| 1 | 1.77 (1.67, 1.88) | <0.001 |
| 2 | 1.36 (1.27, 1.44) | <0.001 |
| 3 | 1.18 (1.14, 1.23) | <0.001 |
| 4 | 1.10 (1.06, 1.13) | <0.001 |
| 5 | 1.05 (1.02, 1.07) | <0.001 |
| AF at age <60 | ||
| 1 | 4.67 (3.57, 6.08) | <0.001 |
| 2 | 2.13 (1.47, 2.87) | <0.001 |
| 3 | 1.34 (1.06, 1.61) | 0.06 |
| 4 | 1.35 (1.12, 1.54) | <0.001 |
| 5 | 1.02 (0.89, 1.12) | 0.53 |
| AF at age ≥60 | ||
| 1 | 1.94 (1.68, 2.22) | <0.001 |
| 2 | 1.36 (1.21, 1.47) | <0.001 |
| 3 | 1.26 (1.13, 1.36) | <0.001 |
| 4 | 1.07 (0.99, 1.11) | 0.060 |
| 5 | 1.07 (0.99, 1.10) | 0.076 |
| Degree of relatives | Risk ratio (95%CI) | P-value |
|---|---|---|
| All AF | ||
| 1 | 1.77 (1.67, 1.88) | <0.001 |
| 2 | 1.36 (1.27, 1.44) | <0.001 |
| 3 | 1.18 (1.14, 1.23) | <0.001 |
| 4 | 1.10 (1.06, 1.13) | <0.001 |
| 5 | 1.05 (1.02, 1.07) | <0.001 |
| AF at age <60 | ||
| 1 | 4.67 (3.57, 6.08) | <0.001 |
| 2 | 2.13 (1.47, 2.87) | <0.001 |
| 3 | 1.34 (1.06, 1.61) | 0.06 |
| 4 | 1.35 (1.12, 1.54) | <0.001 |
| 5 | 1.02 (0.89, 1.12) | 0.53 |
| AF at age ≥60 | ||
| 1 | 1.94 (1.68, 2.22) | <0.001 |
| 2 | 1.36 (1.21, 1.47) | <0.001 |
| 3 | 1.26 (1.13, 1.36) | <0.001 |
| 4 | 1.07 (0.99, 1.11) | 0.060 |
| 5 | 1.07 (0.99, 1.10) | 0.076 |
RR in relatives of AF patients, by degree of relationship, for all AF and stratified by age <60 or ≥60
| Degree of relatives | Risk ratio (95%CI) | P-value |
|---|---|---|
| All AF | ||
| 1 | 1.77 (1.67, 1.88) | <0.001 |
| 2 | 1.36 (1.27, 1.44) | <0.001 |
| 3 | 1.18 (1.14, 1.23) | <0.001 |
| 4 | 1.10 (1.06, 1.13) | <0.001 |
| 5 | 1.05 (1.02, 1.07) | <0.001 |
| AF at age <60 | ||
| 1 | 4.67 (3.57, 6.08) | <0.001 |
| 2 | 2.13 (1.47, 2.87) | <0.001 |
| 3 | 1.34 (1.06, 1.61) | 0.06 |
| 4 | 1.35 (1.12, 1.54) | <0.001 |
| 5 | 1.02 (0.89, 1.12) | 0.53 |
| AF at age ≥60 | ||
| 1 | 1.94 (1.68, 2.22) | <0.001 |
| 2 | 1.36 (1.21, 1.47) | <0.001 |
| 3 | 1.26 (1.13, 1.36) | <0.001 |
| 4 | 1.07 (0.99, 1.11) | 0.060 |
| 5 | 1.07 (0.99, 1.10) | 0.076 |
| Degree of relatives | Risk ratio (95%CI) | P-value |
|---|---|---|
| All AF | ||
| 1 | 1.77 (1.67, 1.88) | <0.001 |
| 2 | 1.36 (1.27, 1.44) | <0.001 |
| 3 | 1.18 (1.14, 1.23) | <0.001 |
| 4 | 1.10 (1.06, 1.13) | <0.001 |
| 5 | 1.05 (1.02, 1.07) | <0.001 |
| AF at age <60 | ||
| 1 | 4.67 (3.57, 6.08) | <0.001 |
| 2 | 2.13 (1.47, 2.87) | <0.001 |
| 3 | 1.34 (1.06, 1.61) | 0.06 |
| 4 | 1.35 (1.12, 1.54) | <0.001 |
| 5 | 1.02 (0.89, 1.12) | 0.53 |
| AF at age ≥60 | ||
| 1 | 1.94 (1.68, 2.22) | <0.001 |
| 2 | 1.36 (1.21, 1.47) | <0.001 |
| 3 | 1.26 (1.13, 1.36) | <0.001 |
| 4 | 1.07 (0.99, 1.11) | 0.060 |
| 5 | 1.07 (0.99, 1.10) | 0.076 |
References
Chugh SS, Blackshear JL, Shen WK, Hamill SC, Gersh B. Epidemiology and natural history of atrial fibrillation: clinical implications.
Benjamin EJ, Wolf PA, D'Agostino RB, Silberhatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham study.
Go AS, Hylek EM, Phillips KA, Chang Y, Henault LE, Selby JV, Singer DE. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: anticoagulation and risk factors in atrial fibrillation (ATRIA) study.
Benjamin EJ, Levy D, Vaziri SM, D'Agostino RB, Belanger AJ, Wolf PA. Independent risk factors for atrial fibrillation in a population-based cohort: the Framingham Heart Study.
Aviles RJ, Martin DO, Apperson-Hansen C, Houghtaling PL, Rautaharju P, Kronamal RA, Tracy RP, Van Wagoner DR, Psaty BM, Lauer MS, Chung MK. Inflammation as a risk factor for atrial fibrillation.
Kopecky S, Gersh B, McGoon M, Whisnant JP, Holmes DR Jr, Ilstrup DM, Frye RL. The natural history of lone atrial fibrillation. A population based study over three decades.
Darbar D, Herron BA, Ballew JD, Jahangir AS, Gersh BJ, Shen WK, Hammill SC, Packer Dl, Olson TM. Familial atrial fibrillation is a genetically heterogenous disorder.
Brugada R, Tapscott T, Czernuszewics GZ, Marian AJ, Iglesias A, Mont L, Brugada J, Girona J, Domingo A, Bachinski LL, Roberts R. Identification of a genetic locus for familial atrial fibrillation.
Chen YH, Xu SJ, Bendahhou S, Wang XL, Wang Y, Xu WY, Jin HW, Sun H, Su XY, Zhuang QN, Yang YQ, Li YB, Liu Y, Xu HJ, Li XF, Ma N, Mou CP, Chen Z, Barhanin J, Huang W. KCNQ1 gain of function mutation in familial atrial fibrillation.
Ellinor P, Shin JT, Moore RK, Yoerger DM, MacRae CA. Locus for atrial fibrillation maps to chromosome 6q14–16.
Olson TM, Michaels VV, Ballew JD, Reyna SP, Karst ML, Herron KJ, Horton SC, Rodeheffer RJ, Anderson JL. Sodium channel mutations and susceptibilty to heart failure and atrial fibrillation.
Fox CS, Parise H, D'Agostino RB, Lloyd-Jones DM, Vasan RS, Wang TJ, Levy D, Wolf PA, Benjamin EJ. Parental atrial fibrillation as a risk factor for atrial fibrillation in an offspring.
Gulcher J, Kong A, Stefansson K. The genealogic approach to human genetics of disease.
Brand FN, Abbott RD, Kannel WB, Wolf PA. Characteristics and prognosis of lone atrial fibrillation. 30-year follow-up in the Framingham Study.
Sigurdsson E, Thorgeirsson G, Sigvaldason H, Sigfusson N. Prevalence of coronary heart disease in Icelandic men 1968–1986.
Jonsdottir LS, Sigfusson N, Sigvaldason N, Thorgeirsson G. Incidence and prevalence of recognised and unrecognised myocardial infarction in women. The Reykjavik Study.
Sigurdardottir S, Helgason A, Gulcher JR, Stefansson K, Donelly P. The mutation rate in the human mtDNA control region.
Helgason A, Hickey E, Goodacre S, Bosnes V, Stefanson K, Ward R, Sykes B. mtDNA and the islands of the North Atlantic. Estimating the proportions of Norse and Gaelic ancestry.
Helgason A, Sigurdardottir S, Gulcher JR, Ward R, Stefansson K. mtDNA and the origin of Icelanders. Deciphering signals of recent population history.
Helgason A, Sigurdardottir S, Nicholson J, Sykes B, Hill EW, Bradley DG, Bosnes V, Gulcher JR, Ward R, Stefansson K. Estimating Scandinavian and Gaelic ancestry in the male settlers of Iceland.
Haines JL, Pericak-Vance MA.
Sveinbjornsdottir S, Hicks AA, Jonsson T, Petursson H, Gudmundsson G, Frigge ML, Kong A, Gulcher JR, Stefansson K. Familial aggregation of Parkinson's disease in Iceland.
Cannon-Albright LA, Thomas A, Goldgar DE, Gholami K, Rowe K, Jacobsen M, McWhorter WP, Skolnick MH. Familiality of cancer in Utah.
Risch N. Linkage strategies for genetically complex traits: I. Multilocus models.
Guo SW. Inflation of sibling recurrence-risk ratio, due to ascertainment bias and/or overreporting.
Amundadottir LT, Thorvaldsson S, Gudbjartsson DF, Sulem P, Kristjansson K, Arnason S, Gulcher JR, Bjornsson J, Kong A, Thorsteinsdottir U, Stefansson K. Cancer as a complex phenotype: pattern of cancer distribution within and beyond the nuclear family.
Gudmundsson H, Gudbjartsson DF, Frigge M, Gulcher JR, Stefansson K. Inheritance of human longevity in Iceland.
Hill AB. The environment and disease: association or causation?
Helgadottir A, Manolescu A, Thorleifsson G, Gretarsdottir S, Jonsdottir H, Thorsteinsdottir U, Samani NJ, Gudmundsson G, Grant SF, Thorgeirsson G, Sveinbjornsdottir S, Valdimarsson EM, Matthiasson SE, Johannson H, Gudmundsdottir O, Gurney ME, Sainz J, Thorhallsdottir M, Andresdottir M, Frigge ML, Topol EJ, Kong A, Gudnason V, Hakonarson H, Gulcher JR, Stefansson K. The gene encoding 5-lipoxygenase activating protein confers risk of myocardial infract and stroke.
Gretarsdottir S, Thorleifsson G, Reynisdottir ST, Manolescu A, Jonsdottir S, Jonsdottir T, Gudmundsdottir T, Bjarnadottir SM, Einarsson OB, Gudjonsdottir HM, Hawkins M, Gudmundsson G, Gudmundsdottir H, Andrason H, Gudmundsdottir AS, Sigurdardottir M, Chou TT, Nahimas J, Goss S, Sveinbjornsdottir S, Valdimarsson EM, Jakobsson F, Agnarsson U, Gudnason V, Thorgeirsson G, Fingerle J, Gurney M, Gudbjartsson D, Frigge ML, Kong A, Stefansson K, Gulcher JR. The gene encoding phosphodiesterase 4D confers risk of ischemic stroke.


{kind=link}