





Abstract
The aim of the present study was to compare the recolonization pattern of mutans streptococci on densely colonized teeth with and without fixed orthodontic appliances after treatment with a 40 per cent chlorhexidine (CHX) varnish (EC 40®, Explore). Healthy subjects free of carious lesions requiring fixed orthodontic appliance treatment but with high bacterial mutans streptococci saliva counts were recruited (n = 10). For baseline registration, plaque from buccal sites was sampled and cultivated on Dentocult® strips. Following professional tooth cleaning, CHX varnish was applied to all teeth for 8 minutes. Subsequently, orthodontic brackets and bands were inserted in either the upper or lower arch. Eight weeks after varnish application the degree of recolonization with mutans streptococci was reassessed on the buccal sites. Statistical analysis showed that recolonization with mutans streptococci was significantly higher (P < 0.05) on teeth with orthodontic appliances.
The results indicate that the use of fixed orthodontic appliances creates artificial environments suitable for the proliferation of mutans streptococci after CHX varnish suppression.
Introduction
Caries preventive measures, based on good oral hygiene, establishment of non-cariogenic dietary habits and the regular supplement of fluorides, are often not sufficient to prevent the development of new carious lesions in orthodontic patients with high caries activity. Beyond a certain caries activity level, neither an increase in the frequency of tooth brushing nor in the dose of administered fluoride is suitable to effectively stop the demineralization process in high-risk individuals (Øgaard et al., 1994). Patients undergoing orthodontic therapy have oral ecological changes that lead to increased numbers of mutans streptococci in saliva and plaque (Lundström and Krasse, 1987a, b).
It has also been shown that the application of fixed appliances results in enamel dermineralization and an increase in the number of carious lesions (Mitchell, 1992). It could be assumed that the insertion of orthodontic devices increases caries risk as they provide artificial niches for cariogenic micro-organisms. Therefore, preventive efforts in these ‘-at-risk’ groups should concentrate on the direct suppression of the cariogenic micro-flora by chemotherapeutics.
Chlorhexidine (CHX) is the most potent documented antimicrobial agent against mutans streptococci and dental caries. Different modes of administration have been recommended for caries prevention (Zickert et al., 1982; Fardal and Turnbull, 1986; Emilson, 1994).
It has been suggested that CHX application as a varnish results in a longer lasting suppression of mutans streptococci compared with other forms of application (Emilson, 1994; Pienihäkkinen et al., 1995; Attin et al., 2003). High and low concentrations of CHX have been reported to reduce the number of mutans streptococci in plaque and saliva (Sandham et al., 1988, 1991; Schaeken et al., 1989) for considerable periods of time (Schaeken et al., 1989; 1991; Schaeken and De Haan, 1989). Numerous studies have examined differently concentrated CHX varnishes formulated as supersaturated solutions of chlorhexidine-di-acetate in ethanol, stabilized by the natural resin sandarac. The optimal CHX varnish concentration suggested for effective suppression of mutans streptococci is in 40 per cent CHX (EC40®, Explore, Nijmegen, Netherlands). These studies reported that mutans streptococci were significantly suppressed for at least 4 weeks after a single CHX varnish application. This effect was tested in patients not undergoing orthodontic treatment. However, studies performed in high-risk orthodontic patients using highly concentrated CHX varnish treatment resulted in no influence on caries increment (Jenatschke et al., 2001).
It is uncertain whether the recolonization of mutans streptococci is enforced by orthodontic devices. The objective of the present study was, therefore, to investigate the recolonization pattern of mutans streptococci on sites adjacent to orthodontic appliances in comparison with teeth free of orthodontic devices after antibacterial treatment. The working hypothesis was that sites adjacent to appliances would have greater colonization than sites without appliances.
Subjects and methods
Subjects
The volunteers gave informed consent for participa-tion in the study. Twenty-seven volunteers requiring fixed orthodontic appliances, at the Department of Orthodontics, were screened and 10 were selected who fulfilled the inclusion criteria: high levels of mutans streptococci in saliva, i.e. at least a score of 2 identified with the chair-side Strip mutans method (Jensen and Bratthall, 1989). Scores of 2 and 3 correspond to approximately 105 colony-forming units (CFU)/ml saliva or more. While the majority of subjects had a full compliment of teeth, some had undergone premolar extractions due to orthodontic indication and the third molars were unerupted. None of the patients had detectable carious lesions or defective restorations. Moreover, clinical examination and radiographs did not reveal any lesions at the interproximal tooth surfaces.
Study design
Professional tooth cleaning was performed and oral hygiene instruction was given to the participants prior to the study. For the baseline examination, the subjects refrained from all oral hygiene measures for 24 hours. At baseline (time point 1) mutans streptococci levels in plaque and saliva were recorded.
The plaque mutans streptococci scores were determined with the site-specific modified Strip mutans technique as originally described by Wallman and Krasse (1993) and modified by Twetman (1995). The number of CFU with characteristic morphology was screened and scored 0–3. The evaluation was blind.
Score 0 corresponded to no CFU (mutans streptococci below detection level):The selected teeth for plaque sampling were isolated with cotton rolls and dried. A small sterile brush was carefully applied to the buccal sites (cervical area) of the two molars to be banded and the premolars to be bracketed and the corresponding teeth in the opposite arch. In subjects with extracted premolars the canines were evaluated. The sampled plaque was immediately spread on the roughened side of the plastic strip from a commercially available test kit (Strip mutans, Orion Diagnostica, Espoo, Finland). The strips were allowed to dry for 5 minutes at room temperature and were then incubated for 48 hours in a liquid medium. The composition of the medium was similar to that of mitis salivarius agar, with the sucrose concentration increased to 30 per cent. The addition of a bacitracin disc® from the kit results in a final concentration of 0.36 U bacitracin/ml medium (Jensen and Bratthall, 1989). Additionally, a saliva Strip mutans test was performed for each participant. After 48 hours' cultivation in the liquid medium the scores of mutans streptococci in plaque were recorded with the aid of a stereomicroscope with a magnification of ×10–25 (Twetman, 1995).
score 1 = 1–10 CFU; approximately less than 104–105 CFU
score 2 = 10–100 CFU; approximately 105–106 CFU
score 3 > 100 CFU; more than 106 CFU
Prior to each varnish application with EC40®, the teeth were professionally cleaned with rubber cups and pumice paste and the interdental areas with unwaxed dental floss. Each quadrant was isolated with cotton rolls and dried with compressed air. EC40® was applied to all teeth with a brush, delivered to the interproximal areas with unwaxed dental floss. The varnish was left in place for 8 minutes and then removed with a brush and dental floss. The varnish was applied only once and the mutans streptococci values in the saliva were assessed after 1 week, as described above. In subjects displaying mutans streptococci in saliva with a score of 1 or higher, the varnish was applied a second time. This was the case in 20 per cent of the subjects.
The orthodontic appliances were randomly placed in either the upper or lower arch of the subject. The respective antagonist teeth in the arch without any appliance served as the control.
Eight weeks after the final varnish treatment, mutans streptococci levels in plaque and saliva were recorded at the buccal sites of the control teeth and at the buccal sites adjacent to the brackets, as described above.
Statistical methods
All microbiological measurements were observed on a grading scale, i.e. the observations were so-called ordered categorical data and, thus, standard statistical methods such as the t-test or analysis of variance could not be applied. For the analysis of such data, ranking methods have been developed (Brunner and Langer, 2000). For this purpose, the original observations were replaced with their ranks. As only four gradings (0, 1, 2, and 3) were possible, many observations had the same values, which, in the statistical literature, are called ‘ties’ (Brunner et al., 2002). When tied, the observations were given midranks. Because ranking methods were used for the analysis of the data, it was reasonable to use the means of the ranks to summarize the outcome of the trial in tables and graphs.
The statistical design underlying the observations in the present investigation was a repeated measures design, i.e. the same patients were repeatedly observed at several time points. The main question in such a trial is whether the time profiles of the rank means for the two treatment groups are significantly different (significance level was set at 5 per cent). If the hypothesis of parallel time profiles was rejected, subsequent post hoc analyses were performed using an appropriate adjustment of the significance level. This means that statistically significant differences are assumed when the time profiles are not parallel. For a detailed description of these methods, see Brunner et al. (2002).
Results
Statistical analysis was undertaken as described using rank mean values. At baseline (time point 1) there was no statistical difference between teeth prior to active orthodontic treatment and teeth that were not going to have orthodontic intervention, which served as the controls (P = 0.643).
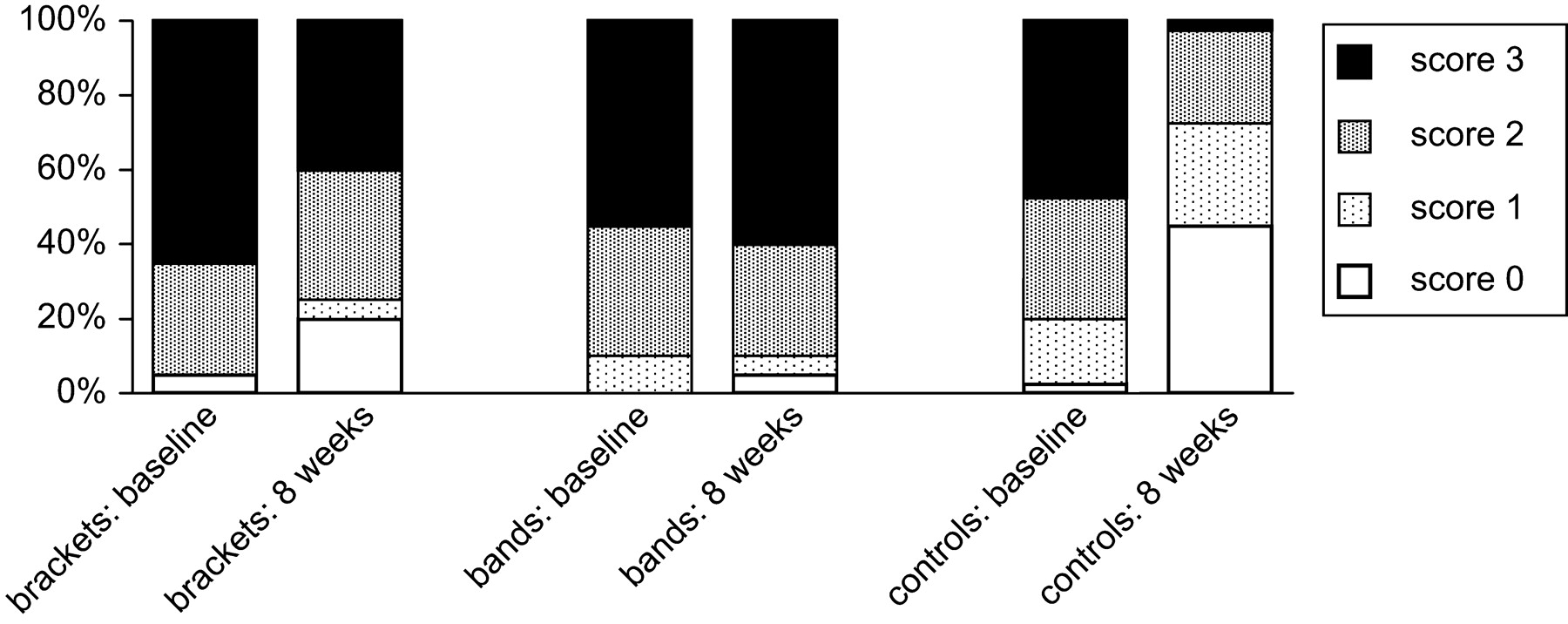
The original data for the percentage distributions of the bacterial determinations are given in Figure 1.
Percentage of plaque samples with scores (0–3) for mutans streptococci at baseline and 8 weeks after varnish treatment.
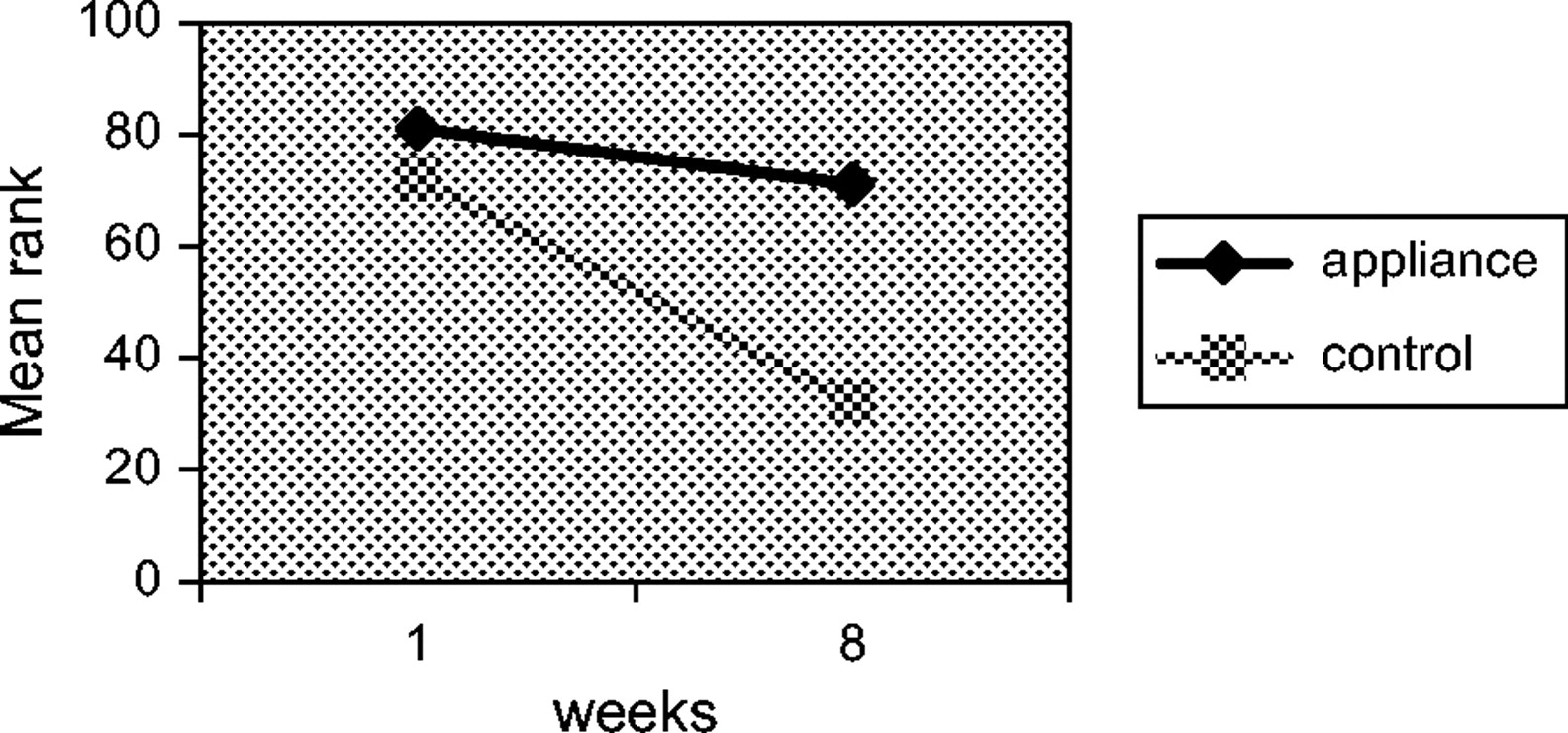
The results of site-specific plaque samples on teeth prior to orthodontic treatment and teeth that were not scheduled for orthodontic treatment at baseline (1) and 8 weeks after varnish treatment are shown in Figure 2.
Mean ranks of mutans streptococci counts in plaque at baseline and 8 weeks after treatment with EC40® in teeth with or without appliances.
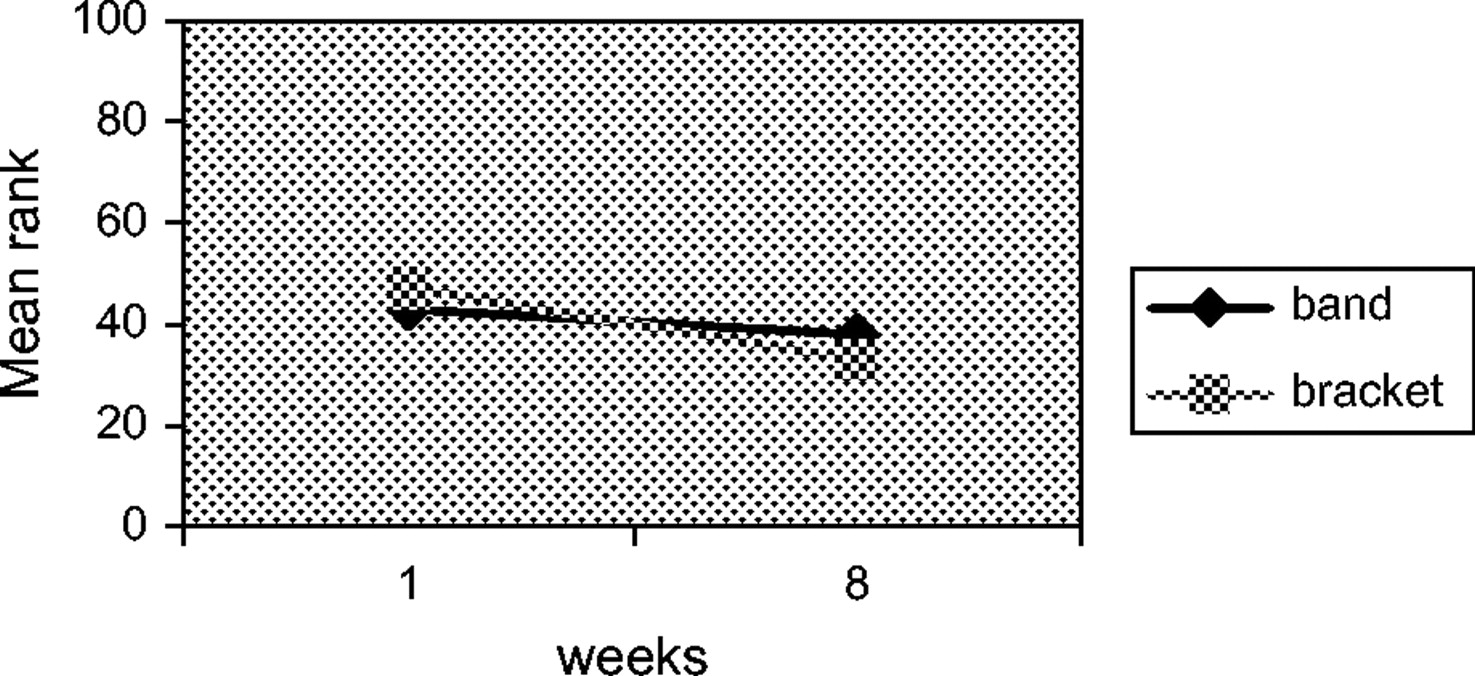
Significantly different time profiles could be observed (P = 0.023) when comparing both groups. At baseline, teeth with appliances showed a mean rank of 81, which was not significantly different from the controls (mean rank 72). However, after 8 weeks, the controls exhibited a significantly lower mean rank (32) compared with teeth with orthodon-tic devices (mean rank 71). For the teeth without orthodontic appliances (controls), varnish treatment resulted in a sig-nificant reduction in mutans streptococci when comparing the baseline values to those obtained at 8 weeks (P = 0.0013). No significant effect could be observed in teeth with orthodontic appliances (P = 0.218). For these teeth, the values gradually returned to those found at baseline and were not significantly different from time point 1. Comparing the effect of varnish treatment of teeth with bands versus teeth with brackets after 8 weeks, no significant differences could be observed (P = 0.183). Therefore, from Figure 3 it becomes obvious that the mean ranks at baseline (bands: 43; brackets: 47) were not different from the mean ranks 8 weeks after varnish treatment (bands: 38; brackets: 33).
Mean ranks of mutans streptococci counts in plaque at baseline and 8 weeks after treatment with EC40® in teeth with bands or brackets.
Discussion
It has been shown that following treatment with highly concentrated CHX varnishes, mutans streptococci can be suppressed effectively for a prolonged period of time (Schaeken et al., 1991; Ie and Schaeken, 1993; Attin et al., 2003). The optimal concentration has been suggested to be contained in 40 per cent CHX varnishes (Schaeken and De Haan, 1989; Schaeken et al., 1989).
Moreover, Ie and Schaeken (1993) observed that in some subjects two subsequent applications of highly concentrated varnish led to a longer suppression of mutans streptococci compared with a single application. This effect was also found in 20 per cent of the subjects in the present study, where the first application did not suppress saliva mutans streptococci below the detection level. In these instances, the high concentration varnish was applied for a second time, resulting in effective suppression of mutans streptococci. In patients in whom after 1 week the suppression continued to be observed, the varnish was assumed to have a long-term effect.
Because a primary aim of the present study was to evaluate the importance of bands and brackets on the recolonization pattern of mutans streptococci after antibacterial therapy, a split mouth design was used, with each subject being his/her own control. In this way, the number of participating subjects could be kept relatively low. Intergroup differences in the average of mutans streptococci values at baseline were negligible and not significant.
The present investigation revealed that mutans streptococci colonization was higher in teeth with fixed orthodontic appliances compared with the control teeth without appliances. However, this effect was only slightly sig-nificant (P = 0.023). Therefore, it may not be clinically relevant.
It should be noted that studies performed in high-risk orthodontic patients did not find significant differences in caries increment after repeated application of high or low concentrated CHX varnishes (Lundström and Krasse, 1987a; Jenatschke et al., 2001). Those authors assumed that the duration of mutans streptococci suppression partly depends on the extent to which any retention niches are coated with varnish. It was also speculated that bacterial resistance occurred during continuing varnish therapy.
In the study by Jenatschke et al. (2001), varnish application was performed on the day of bracket placement and repeated at 8 week intervals, while the fixed appliances were in place. Furthermore, no second application was performed at the beginning of mutans streptococci suppression, as opposed to the present study. The results of the present investigation show that the mutans streptococci counts on teeth with brackets and bands returned to baseline values after 8 weeks. Therefore, bearing in mind these findings, it is perceivable that no effect on caries increment could be achieved as cariogenic bacteria could not effectively be suppressed.
The effectiveness of the high concentration varnish may be explained by the toxic effect of the varnish, so that almost all mutans streptococci are killed in a single or, as described previously, a two-time application resulting in a delayed recolonization compared with treatment with low concentrated agents, such as CHX gels or varnishes. The presence of orthodontic devices is likely to hamper the application of varnish on all surfaces on which mutans streptococci exist; thus the application of varnish should be performed before banding and bracketing in order to eliminate nearly all mutans streptococci at the beginning of therapy. Furthermore, the commencement of the recolonization with mutans streptococci after antimicrobial therapy in highly colonized teeth has to be investigated. Due to the design of the study, which assessed mutans streptococci counts at baseline and at 8 weeks, the definite time point of recolonization was not discernible. Adapting the repetition of varnish applications to recolonization time could presumably avoid a return of mutans streptococci to baseline values and achieve long-term suppression.
In contrast to the results of the present study, Øgaard et al. (1997) achieved mutans streptococci suppression in patients with fixed orthodontic appliances 20 weeks after application of a low concentration varnish. In their investigation, varnishing was performed before the placement of orthodontic bands and brackets. They found significantly reduced mutans streptococci counts in comparison with the untreated controls. However, those authors ignored the initial mutans streptococci colonization of the subjects, in contrast to the present investigation. Emilson and Lindquist (1988) evaluated the coherence of the infection level of mutans streptococci and recolonization of teeth after CHX treatment and reported that tooth surfaces with a high level of infection are more rapidly colonized by mutans streptococci, even if these micro-organisms have been suppressed to undetectable levels after antimicrobial treatment. This shows that a slow recolonization pattern and higher efficacy can be achieved after antimicrobial treatment in low colonized teeth.
Because in orthodontic patients with high caries activity standard caries prevention measures based on oral hygiene, non-cariogenic dietary habits and regular supplementation of fluorides are often insufficient to prevent the development of new carious lesions, the use of antimicrobials or, alternatively, the early removal of bands and brackets is necessary. On the other hand, the present study showed, in agreement with the findings of Jenatschke et al. (2001), that the efficacy of the most potent CHX treatment as shown in high-risk non-orthodontic subjects (Emilson, 1994; Pienihakkinen et al., 1995; Attin et al., 2003) failed in highly mutans streptococci colonized teeth in orthodontic patients.
Conclusions
The negative influence of orthodontic bands and brackets on the effectiveness of antimicrobial therapy could be proven in the present study. Nevertheless, the use of antimicrobials is currently the only promising alternative to improved oral hygiene, fluoridation measures and dietary counselling for caries prevention. Consideration has to be given to the mode of application of antimicrobial varnishes to achieve a long-term suppression in at-risk orthodontic patients. Developing more effective therapy modes and identifying existing sources of error in application should be investigated in further studies.
References
Attin R, Tuna A, Attin T, Brunner E, Noack M J
Brunner E, Langer F
Brunner E, Domhof S, Langer F
Emilson C G
Emilson C G, Lindquist B
Fardal O, Turnbull R S
Ie Y L, Schaeken M J M
Jenatschke F, Elsenberger E, Welte H D, Schlagenhauf U
Jensen B, Bratthall D
Lundström F, Krasse B
Lundström F, Krasse B
Mitchell L
Øgaard B, Seppä L, Rölla G
Øgaard B, Larsson E, Glans R, Henriksson T, Birkhed D
Pienihäkkinen K, Söderling E, Ostela I, Leskelä I, Tenovuo J
Sandham H J, Brown J, Chan K H
Sandham H J, Nadenau L, Philips H I
Schaeken M J M, De Haan P
Schaeken M J M, Van der Hoeven J S, Hendriks J C M
Schaeken M J M, Schouten M J, Van Den Kieboom C W A, Van Der Hoeven J S
Twetman S
Wallman C, Krasse B
Author notes
*Department of Operative Dentistry and Preventive Dentistry and Periodontology, University of Göttingen, **Private Practice, Köln, ***Department of Operative Dentistry and Periodontology, University of Würzburg, ****Medical Statistics, University of Göttingen, Germany


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}