




Abstract
Recent anatomic findings suggest aging-related changes of the complex fat distribution in the hand.
To rejuvenate the aging hand, we developed a targeted fat grafting technique based on the physiologic fat distribution of the hand.
The dorsum of both hands was examined in 30 healthy volunteers of different age utilizing B-mode ultrasound to determine physiological changes of the aging hand. Additional anatomic dissection was performed in 10 hands of five fresh cadavers to establish the anatomic basis for the targeted restoration technique. A total of 17 patients were treated for hand rejuvenation utilizing this technique and followed up for at least 6 months. The posttreatment outcome was assessed through B-mode ultrasound, 3-dimensional (3D) topography scanning, and a patient satisfaction survey.
According to the fat distribution of the dorsum, hand aging was divided into three grades: (1) mild atrophy with rhytides; (2) moderate atrophy with exposed veins; and (3) serious atrophy with exposed tendons. Anatomic findings showed the existence of distinct superficial and deep fat compartments. The average fat grafting volume was 25.5 ml per hand dorsum administered in one or two procedures. Patients were monitored for 8.3 ± 2.6 months. After 6 months, a volume gain was found in all patients. The degree of aging was significantly reduced. The majority of patients (94.1%) were satisfied with their results.
This study provides the anatomic and clinical basis for targeted restoration of the physiological fat volume in the hand dorsum with high satisfaction rates.

The hand represents one of the most important functional parts of the human body. Aging-related volume loss results in wrinkles, bulging veins, and distinctly visible tendons in the dorsum of the hand. Owing to an increasingly holistic aesthetic approach, the demand for hand rejuvenation has significantly risen in recent years.1,2 Therapeutic options for hand rejuvenation include artificial filler injection, laser therapy, sclerotherapy, and autologous fat grafting,3-7 among which autologous fat grafting achieves the most aesthetically pleasing and stable results in the long term.8-10
Recent anatomic findings suggest aging-related changes of the complex fat distribution in the hand, but a systematic analysis of the dorsal hand regarding the aging and rejuvenation process is lacking. We hypothesized that anatomically correct restoration of the respective atrophic fat layers allows for improved, natural-looking outcomes. Utilizing B-mode ultrasound and anatomic dissection, we first identified the physiological fat volume and distribution of the dorsal hand in different age groups and, based on these findings, developed a targeted restoration technique to obtain a youthful and natural-looking hand. Moreover, we share our clinical experience and long-term results of patients treated with this hand rejuvenation approach.
MethodS
B-Mode Ultrasound Examination of the Dorsal Hand
In January 2014, a total of 30 hands from 30 healthy volunteers of different age groups, range 4 to 67 years of age, were examined utilizing B-mode ultrasound to assess physiological changes of fat distribution during aging. Inclusion criteria were as follows: (1) healthy volunteers of any age recruited from the outpatient clinic, (2) BMI range 15 to 25 kg/m2, and (3) no obvious change in weight for 1 month. Exclusion criteria included the presence of risk factors including smoking, diabetes, and vascular diseases involving the hand, and infectious diseases. All volunteers were divided into three age groups each with a male-to-female ratio of 1:1: under 18 years of age, 19 to 45 years of age, and above 45 years of age. Each group consisted of 10 volunteers with average ages of 10.3, 35.2, and 59.3 years of age, respectively. We investigated the soft tissue layers and distribution of the dorsal hand and determined differences between the different age groups.11
Anatomic Study
Between September 2013 and January 2014, we dissected 10 hands from five fresh cadavers, two men and three women, with a mean age of 62.7 years of age (range, 58-83 years of age), to identify fat compartments and neurovascular structures in the dorsum of the hand with special regard to soft tissue layers and their extent. Cadavers were obtained from the Willed Body Program at Shanghai Jiao Tong University School of Medicine. The study was conducted after approval by the Independent Ethics Committee of Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine. In detail, we injected methylene blue dye into the superficial lamina of six dorsal hands. Four hours later, we analyzed the distribution of the dye and determined the extent of the superficial fat compartments of the dorsal hands.12 In addition, possible approaches for fat grafting to the dorsal hand were evaluated. Because of unpredictable postmortem changes in tissue volume, soft tissue thickness of the dorsal hand was only measured in healthy volunteers and patients for correlation with age.
Clinical Application of Targeted Fat Grafting for Hand Rejuvenation
Patients
Between January 2014 and June 2014, 17 healthy female patients underwent fat grafting to the dorsal hand in our outpatient clinic. The average patient age was 51.5 years (range, 45-60 years) (Table 1). All patients presented with distinct rhytides and considerably exposed veins and tendons in the dorsal hand. The study was approved by the Independent Ethics Committee of Shanghai Ninth People’s Hospital affiliated to Shanghai Jiao Tong University School of Medicine in Shanghai, China. Each patient was fully informed regarding the aim of the study, treatment, risks, and possible complications. All surgical procedures were performed by the same plastic surgeon (L.Q.F.) after informed written consent was given by the patients. Exclusion criteria included the chronic use of steroids, connective tissue diseases, chronic blood abnormalities, and other systemic metabolic disorders, including diabetes, a history of obesity or body dysmorphic disorder, anticoagulant treatment, and previous chemotherapy and radiotherapy.
Demographic Data and Follow-Up Time for Patients Who Underwent Hand Rejuvenation by Targeted Fat Grafting to the Dorsum of the Hands
| Characteristics | Mean ± SD | Range |
|---|---|---|
| Age, yr | 51.5 ± 5.4 | 40-60 |
| Body weight, kg | 51.9 ± 6.7 | 42-65 |
| Height, cm | 158.5 ± 5.1 | 151-167 |
| BMI, kg/m2 | 20.7 ± 2.5 | 15.8-24.7 |
| Total follow-up time, months | 8.3 ± 2.6 | 6-12 |
| Characteristics | Mean ± SD | Range |
|---|---|---|
| Age, yr | 51.5 ± 5.4 | 40-60 |
| Body weight, kg | 51.9 ± 6.7 | 42-65 |
| Height, cm | 158.5 ± 5.1 | 151-167 |
| BMI, kg/m2 | 20.7 ± 2.5 | 15.8-24.7 |
| Total follow-up time, months | 8.3 ± 2.6 | 6-12 |
BMI, body mass index
Demographic Data and Follow-Up Time for Patients Who Underwent Hand Rejuvenation by Targeted Fat Grafting to the Dorsum of the Hands
| Characteristics | Mean ± SD | Range |
|---|---|---|
| Age, yr | 51.5 ± 5.4 | 40-60 |
| Body weight, kg | 51.9 ± 6.7 | 42-65 |
| Height, cm | 158.5 ± 5.1 | 151-167 |
| BMI, kg/m2 | 20.7 ± 2.5 | 15.8-24.7 |
| Total follow-up time, months | 8.3 ± 2.6 | 6-12 |
| Characteristics | Mean ± SD | Range |
|---|---|---|
| Age, yr | 51.5 ± 5.4 | 40-60 |
| Body weight, kg | 51.9 ± 6.7 | 42-65 |
| Height, cm | 158.5 ± 5.1 | 151-167 |
| BMI, kg/m2 | 20.7 ± 2.5 | 15.8-24.7 |
| Total follow-up time, months | 8.3 ± 2.6 | 6-12 |
BMI, body mass index
Autologous Fat Grafting Technique
The previously described 3L3M (ie, low pressure, low speed, low volume, multi-tunnels, multi-planes, and multi-points) fat injection technique was applied.13 Briefly, fat was collected by liposuction from the abdomen or thigh regions utilizing the superwet technique. The area to be suctioned was first infiltrated by means of a 3-mm Klein cannula with anesthetic tumescence solution consisting of normal saline with 0.25% lidocaine and 1:500,000 epinephrine. A 20 ml syringe with a 20g cannula was utilized to suction fat under manual regulation of negative pressure, not exceeding 10 cc. The harvested fat was washed three times with normal saline to remove the drugs from the tumescence liquid. Tissue fibers were cut and removed. After centrifugation with 64g force for 2 minutes, the upper oil and lower liquid phases were discarded and the pure fat was ready to use. Multi-layered fat injections to the dorsal hand were performed according to the targeted fat restoration technique to improve age-related changes of the fat compartment architecture of the dorsal hand based on our findings from anatomic and clinical ultrasound studies. The fat injection was conducted in both superficial and deep layers. Deep-layer injections were performed to correct the concave between the metacarpal bones. A gentle injection technique is important to avoid dislocation of the cannula into the tendon sheaths. The superficial layer was grafted according to the anatomy of fat compartments by evenly distributing the fat in the dorsum of the hand. Importantly, fat injection to the middle layer containing the vascular supply was strictly avoided.
Outcome Evaluation
All patients who underwent hand rejuvenation by the target restoration technique had follow-up for at least 6 months. Outcomes were evaluated utilizing photography, B-mode ultrasound, 3D topography scanning, and a patient satisfaction survey.
Standard pictures of both hands were taken in the anteroposterior and oblique positions before and after surgery. For the oblique views, patients were asked to rotate their relaxed hands from anteroposterior to a 45-degree supinated position. B-mode ultrasound was utilized to determine the soft tissue thickness in the dorsal hand and to localize the grafted fat.
The 3D laser surface scanning images were collected utilizing a Konica Minolta Vivid 910 (without the rotating stage set) and Polygen Editing Tools version 2.21 (Konica Minolta, Tokyo, Japan). The patients placed their hands flat on the plate vertical to the ground with their fingers spread to the greatest extent. The images were captured frontally and 80 degrees bilaterally. All digital data were processed utilizing HPxw6200 (Hewlett Packard, Shanghai, China).
Aesthetic outcomes were evaluated for their degree of improvement by plastic surgeons not involved in patient treatment, as well as independent investigators from a nonmedical field based on pretreatment and posttreatment patient pictures. Hand lipoatrophy severity was evaluated according to the following criteria: Grade 0 = a natural and smooth hand contour; Grade 1, mild fat atrophy characterized by rhytides; Grade 2, moderate atrophy exhibiting exposed veins; and Grade 3, serious fat atrophy characterized by exposed tendons.
In addition, a patient satisfactory survey was conducted. At 6 months posttreatment, patients were asked to anonymously complete the patient satisfaction survey in the waiting room of the outpatient clinic. The degree of improvement was classified as very satisfactory for significantly improved hand dorsum, satisfactory for noticeable beneficial effects, and unsatisfactory for no improvement. A blank copy of the survey is available as Supplementary Material at www.aestheticsurgeryjournal.com.
Statistical Analysis
The data were analyzed utilizing the paired sample t test to evaluate the grade of hand lipoatrophy before and after treatment using SPSS 12.0 (SPSS, Inc., Chicago, IL). P values P < 0.05 were considered statistically significant.
RESULTS
Aging Process of the Hand Assessed by Ultrasound
B-mode ultrasound examination showed that the dorsal hand exhibited three fascia layers—superficial, intermediate, and deep fascia layers—that along with the skin form three laminae. The dorsal superficial lamina contains no relevant structures, whereas veins and nerves run in the intermediate lamina. The dorsal deep lamina was found to be separated by tendons into four compartments. The fascia layers of the dorsal hand fused proximally at the level of the extensor retinaculum of the hand. The distribution of fat in the superficial lamina was uneven. The superficial lamina at the dorsal metacarpophalangeal joints contains almost no fat.
The soft tissue thickness of the dorsal hands steadily decreased with age (Figure 1). The average soft tissue thickness between the second and third metacarpal bones, including skin, fat, and fascia, was 3.12 ± 0.78 mm under the age of 19 years, 2.33 ± 1.07 mm in 19- to 45-year-old volunteers, and 1.6 ± 0.54 mm in the group above 45 years of age as assessed by B-mode ultrasound.
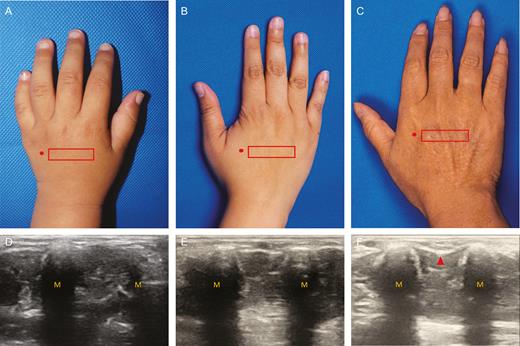
Photographs showing the hand dorsum of (A) a 4-year-old-child, (B) a 25-year-old woman, and (C) a 56-year-old woman. The location of the ultrasound probe is marked in the photographs. Corresponding ultrasound images of the hand dorsum of the (D) child, (E) young woman, and (F) older woman. (M, metacarpal bone. The red arrow in Figure 1F indicates atrophy of the interosseous muscles.).
Veins and tendons in the dorsal hand became more distinct due to aging-related fat atrophy. In more serious cases, the soft tissue between the metacarpal bones was sunken, indicating atrophy of the interosseous muscle. This phenomenon was seen in the group above 45 years of age. According to the fat distribution of the dorsum, the aging hand was divided into three grades: Grade 1, mild fat atrophy characterized by rhytides as a result of photographic aging; Grade 2, moderate atrophy exhibiting exposed veins due to superficial fat loss; and Grade 3, serious fat atrophy characterized by exposed tendons following fat loss of all layers, usually accompanied by interosseous atrophy (Figure 1F).
Architecture of Fat Compartments of the Dorsal Hand Based on Anatomic Dissection Studies
Anatomic dissection studies confirmed the layers in the dorsum of the hand as seen in ultrasound examination including the superficial, intermediate, and deep laminae. The dorsal hand and palm were connected by tight ligaments inserting into the skin. The distribution of dye injected to the dorsal superficial lamina was limited to the area between the carpometacarpal and metacarpophalangeal joints. The methylene blue dye injection results demonstrated the existence of septate in the superficial lamina. In the superficial lamina, the dye spread transversely and separated the dorsal fat lamina into several compartments (Figure 2). The superficial lamina was divided into proximal and distal fat chambers that extend to a line at the distal third of the metacarpals. The four fat compartments between the metacarpophalangeal joints form the distal part, whereas the proximal part consists of three fat compartments (ie, radial, middle, and ulnar compartments). The region of the dorsal metacarpophalangeal joints was scarce in adipose tissue.
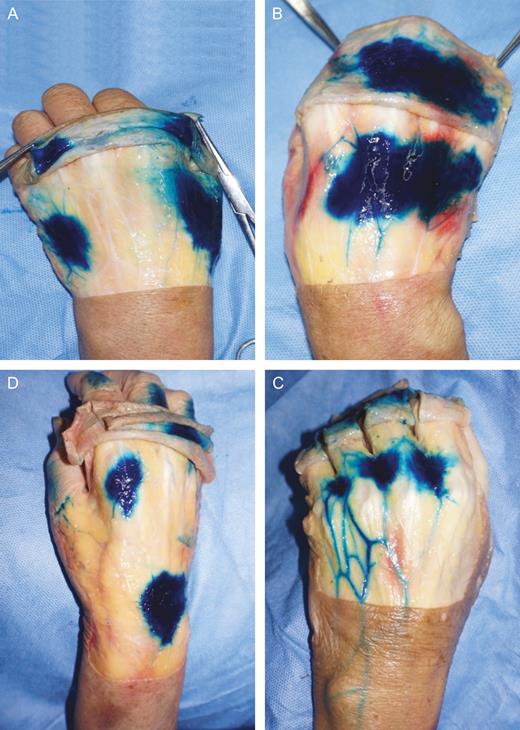
The superficial lamina is divided into proximal and distal fat chambers. The proximal part of the superficial lamina consists of (A) radial, ulnar (left hand, male, 58 years of age), and (B) middle compartment (right hand, male, 58 years of age). (C, D) The fat compartments of the distal part were divided into (C) first (right hand, female, 61 years of age) and (D) second to fourth compartments (left hand, male, 67 years of age).
The Targeted Fat Restoration Technique for Hand Rejuvenation
The targeted restoration technique for the dorsum of the hand was established based on ultrasound and anatomic results. Nonsurgical treatment is recommended for the treatment of grade 1 aged hands. In grade 2 aged hands, fat should be grafted to the superficial lamina, whereas in grade 3 aged hands, both superficial and deep laminae should receive targeted fat restoration (Figure 3).
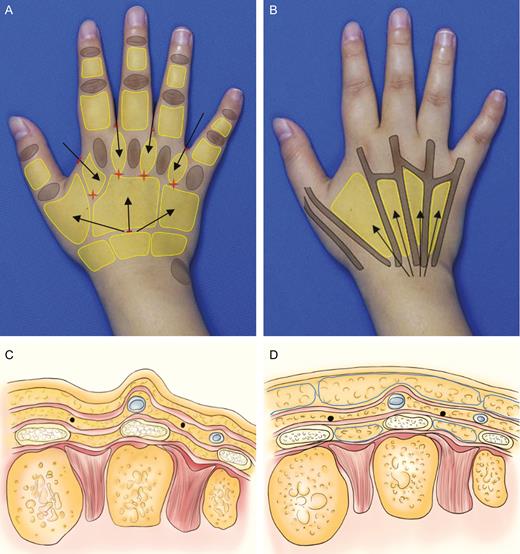
Cannula paths (black arrows) and incisions (red short lines) within (A) the superficial and (B) deep lamina are shown in the right hand of a 35-year-old woman. (A) Red flags mark the location of the dorsal metacarpal perforator arteries. (B) The black lines illustrate the course of the tendons. (C) The illustrations show soft tissue structure and fat compartments in the cross-section of an aged hand. (D) Based on the resetting technique, autologous fat was injected into the superficial and deep fat compartments marked by blue lines.
A total of five incisions were utilized for cannula insertion: one is at wrist and the other four are at the web spaces (Figure 3). At the wrist, the incision was made distally to and in the middle of the extensor retinaculum. Before injection, the patient was asked to stretch the fingers to expose the tendons. Extensor tendons converged at the distal edge of the extensor retinaculum. The incision was made proximal to this point, and dissection was performed onto the extensor retinaculum. The cannula was inserted into the deep lamina distally to the retinaculum, and the injection was performed radially following the direction of the tendons. The distal parts of the superficial fat compartments were targeted through the web spaces. Importantly, fat grafts were injected at the concave into the deep fat compartments between the tendons, whereas the superficial fat compartments located superficial to the tendons were restored by fat grafting to cover the exposed tendons.
Clinical Outcome of Rejuvenated Hands
A total of 17 patients were treated with targeted fat restoration injections to the dorsum of both hands for rejuvenation purposes. All patients were treated in one or two sessions with a mean grafted volume of 25.5 ml (range, 13-39 ml) per hand and were followed up for at least 6 months, 8.3 ± 2.6 months (range, 6-12 months) on average. Considering the higher absorption rate in the hands because of increased mobility, we aimed at a 10% to 15% overcorrection in the fat grafting procedure. There was no case of fat removal. In seven patients, additional fat injection was performed.
At 6 months after surgery, a volume gain in the desired areas was seen in all patients. The hand dorsum became smooth, and the veins and tendons were less exposed as shown in 2-dimensional (2D) topographic analysis, indicating improved hand dorsum contour after autologous fat grafting. Posttreatment B-mode ultrasound showed that the location of the injected fat was consistent with the targeted compartments in the superficial and deep laminae. The exact thickness of the grafted fat was calculated as the difference between pretreatment and posttreatment hand dorsum soft tissue thickness. The soft tissue thickness of the dorsal hands was 1.52 ± 0.53 mm before surgery and 4.04 ± 0.70 mm after surgery. The thickness of the grafted fat was 2.52 ± 0.26 mm.
Standard photography of rejuvenated hands was performed at the 6-month follow-up (Figures 4 and 5). Among 17 patients, the degree of hand lipoatrophy decreased from grade 3 to grade 1 in nine patients, from grade 3 to grade 2 in two patients, from grade 2 to grade 1 in three patients, and from grade 2 to grade 0 in three patients. The t value was 14.990, P < 0.001(t0.001(16) = 4.015). The degree of aging was significantly reduced.

(A) A 58-year-old female patient, 5 years postmenopausal, presented with distinctly visible veins and tendons on the dorsum of both hands, classified as grade 2 lipoatrophy of the hand. (B) A total volume of 15 ml of fat was injected into the superficial lamina of her dorsal hands. Posttreatment photographs. (C) B-mode ultrasound before surgery showed a reduced soft tissue thickness of 1.6 mm without signs of interosseous atrophy and (D) B-mode ultrasound image are shown at 6 months after fat grafting. The yellow arrow marks the superficial lamina. (M, metacarpal bone.).
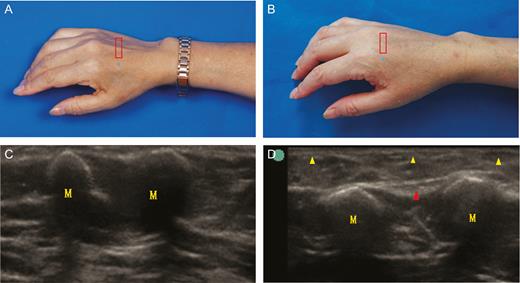
(A) A 54-year-old female patient, 2 years postmenopausal, sought treatment for her grade 3 aging hands. Veins and tendons on her dorsal hands were prominent with a concave contour of the interosseous spaces. (B) A total fat volume of 27 ml was injected into superficial and deep laminae of both dorsal hands. 3D laser scanning demonstrated a significant increase in soft tissue volume posttreatment. (C) The B-mode ultrasound examination before surgery measured a soft tissue thickness of 1.5 mm in the dorsal hand along with mild interosseous atrophy. (D) Standard and B-mode ultrasound photographs at 6 months posttreatment are shown. Arrows mark the superficial (yellow) and deep lamina (red). (M, metacarpal bone.).
3D scanning demonstrated a significant volume increase of 8 to 27.5 ml (average, 10.3 ml).
The patient satisfaction rate was 94.1% in this series; 58.8% of the patients were very satisfied with the posttreatment results, whereas only 5.88% of the patients evaluated their outcome as unsatisfactory (Table 2).
Results of the Patient Satisfaction Survey
| # | Preoperative grade of aging hand | Postoperative grade of aging hand | Patient satisfaction |
|---|---|---|---|
| 1 | 3 | 1 | Satisfactory |
| 2 | 3 | 1 | Very satisfactory |
| 3 | 2 | 0 | Very satisfactory |
| 4 | 2 | 1 | Satisfactory |
| 5 | 3 | 2 | Satisfactory |
| 6 | 2 | 0 | Very satisfactory |
| 7 | 3 | 2 | Satisfactory |
| 8 | 2 | 1 | Satisfactory |
| 9 | 3 | 1 | Very satisfactory |
| 10 | 3 | 1 | Very satisfactory |
| 11 | 2 | 1 | Satisfactory |
| 12 | 3 | 1 | Very satisfactory |
| 13 | 3 | 1 | Unsatisfactory |
| 14 | 3 | 1 | Very satisfactory |
| 15 | 2 | 0 | Very satisfactory |
| 16 | 3 | 1 | Very satisfactory |
| 17 | 3 | 1 | Very satisfactory |
| # | Preoperative grade of aging hand | Postoperative grade of aging hand | Patient satisfaction |
|---|---|---|---|
| 1 | 3 | 1 | Satisfactory |
| 2 | 3 | 1 | Very satisfactory |
| 3 | 2 | 0 | Very satisfactory |
| 4 | 2 | 1 | Satisfactory |
| 5 | 3 | 2 | Satisfactory |
| 6 | 2 | 0 | Very satisfactory |
| 7 | 3 | 2 | Satisfactory |
| 8 | 2 | 1 | Satisfactory |
| 9 | 3 | 1 | Very satisfactory |
| 10 | 3 | 1 | Very satisfactory |
| 11 | 2 | 1 | Satisfactory |
| 12 | 3 | 1 | Very satisfactory |
| 13 | 3 | 1 | Unsatisfactory |
| 14 | 3 | 1 | Very satisfactory |
| 15 | 2 | 0 | Very satisfactory |
| 16 | 3 | 1 | Very satisfactory |
| 17 | 3 | 1 | Very satisfactory |
Results of the Patient Satisfaction Survey
| # | Preoperative grade of aging hand | Postoperative grade of aging hand | Patient satisfaction |
|---|---|---|---|
| 1 | 3 | 1 | Satisfactory |
| 2 | 3 | 1 | Very satisfactory |
| 3 | 2 | 0 | Very satisfactory |
| 4 | 2 | 1 | Satisfactory |
| 5 | 3 | 2 | Satisfactory |
| 6 | 2 | 0 | Very satisfactory |
| 7 | 3 | 2 | Satisfactory |
| 8 | 2 | 1 | Satisfactory |
| 9 | 3 | 1 | Very satisfactory |
| 10 | 3 | 1 | Very satisfactory |
| 11 | 2 | 1 | Satisfactory |
| 12 | 3 | 1 | Very satisfactory |
| 13 | 3 | 1 | Unsatisfactory |
| 14 | 3 | 1 | Very satisfactory |
| 15 | 2 | 0 | Very satisfactory |
| 16 | 3 | 1 | Very satisfactory |
| 17 | 3 | 1 | Very satisfactory |
| # | Preoperative grade of aging hand | Postoperative grade of aging hand | Patient satisfaction |
|---|---|---|---|
| 1 | 3 | 1 | Satisfactory |
| 2 | 3 | 1 | Very satisfactory |
| 3 | 2 | 0 | Very satisfactory |
| 4 | 2 | 1 | Satisfactory |
| 5 | 3 | 2 | Satisfactory |
| 6 | 2 | 0 | Very satisfactory |
| 7 | 3 | 2 | Satisfactory |
| 8 | 2 | 1 | Satisfactory |
| 9 | 3 | 1 | Very satisfactory |
| 10 | 3 | 1 | Very satisfactory |
| 11 | 2 | 1 | Satisfactory |
| 12 | 3 | 1 | Very satisfactory |
| 13 | 3 | 1 | Unsatisfactory |
| 14 | 3 | 1 | Very satisfactory |
| 15 | 2 | 0 | Very satisfactory |
| 16 | 3 | 1 | Very satisfactory |
| 17 | 3 | 1 | Very satisfactory |
Minor complications included edema and ecchymosis. Posttreatment local edema was present in all patients that resolved spontaneously within 3 weeks posttreatment. Ecchymosis of the dorsal hand was observed in 3 patients on the first posttreatment day and subsided without further treatment within 10 days. The presence of bumps was recorded in one early case in which injection cannulae of larger diameter were utilized. Subsequently, neither lumps nor bumps were found during follow-up examinations. The presence of edema, prolonged recovery time, immobilization of the hand for 14 days posttreatment, and peeling of the skin after bandage removal were complaints of the patients. No severe intraoperative and posttreatment complications occurred.
DISCUSSION
Aging in the hands is characterized by increased soft tissue atrophy of the dorsum, including the dermal, fascia, fat tissue, and interosseous muscles layers. Veins and tendons become more visible.14,15 Because of interosseous atrophy, the concave between the metacarpal bones becomes more distinct. Among all kinds of fillers that may be injected to the dorsal hand for rejuvenation purposes, the effect of autologous fat injection has been shown to provide the best results with a low complication rate.9,16
Restitution of fat to the superficial lamina is essential to improve the exposition of veins and nerves that are located in the intermediate lamina, and the tendons run in the deep lamina. Thus, targeted restoration of fat into the superficial lamina allows for the optimal coverage of veins and tendons. Importantly, there is no important structure running in the superficial layer,11,17 making it a safe layer for injection. Secondly, the B-mode ultrasound results showed that interosseous atrophy is a major cause of serious volume loss in the dorsum of the hand. Therefore, fat grafting into the compartments of the deep lamina between the metacarpal bones allows for targeted structural restoration. In our hands, targeted fat injections into these two layers led to highly satisfactory results.
Based on our findings from the dye injection studies and B-mode ultrasound, we identified the metacarpophalangeal joints and extensor retinaculum as distal and proximal borders of the superficial compartment, and the deep layer was separated by the extensor tendons into four fat compartments. We established the resetting technique accordingly, targeting superficial and deep fat compartments with stable results and a natural and youthful hand contour.
The cannula was inserted to the proximal and distal fat compartments through the wrist and finger web incisions, respectively. The arteries of the dorsal hand are located at the distal third of the metacarpals, thus the approach will also preserve vasculature. Notably, veins are running superficial to the retinaculum, whereas tendons are located beneath the retinaculum. The cannula was inserted subcutaneously superficial to the veins into the superficial fat compartments. The cannula may also follow the interosseous muscles between tendons distally and then be inserted into the deep fat compartments. Cannula insertion should be performed from proximal to distal, because the veins become thinner distally, thus the injection should be in the same direction as the course of the veins to protect the vessels. We have applied similar injection incisions as those of Agostini and Perello,17 which are advantageous for the even distribution of fat in the lamina. Furthermore, we found that based on our findings regarding the distribution of fat compartments in superficial lamina, fat graft injection was more accurate. In addition, injection to the interosseous space helps to improve tendon exposure. To prevent lumps and bumps, we recommend careful harvest and purification of the fat graft. Moreover, adequate cannula size such as 17g should be utilized for injection. Cannulae of larger diameter are likely to cause bumps, whereas cannulae with narrow diameter may create oil cysts.
A potential limitation of this study was the lack of a larger number of patients with a longer follow-up period. Further studies will be required to ultimately evaluate our approach. Until then, we believe that these preliminary results may serve as a guideline for plastic surgeons engaged in hand rejuvenation.
CONCLUSIONS
There are independent compartments at the dorsal hand. Targeted fat restoration of the dorsal hands according to the compartment structure is an effective and safe method for hand rejuvenation. Further studies will be necessary to determine the outcome and potential risks of this procedure in the long term.
Supplementary Material
This article contains supplementary material located online at www.aestheticsurgeryjournal.com.
Disclosures
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
This work was supported by the National Natural Science Foundation of China (program #81620108019), which provided equipment and assisted with laboratory costs.
References


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}