

Abstract
Nuclear medicine (NM) services in Indonesia have rapidly developed due to the increasing number of patients, and this growth has been supported by standardized regulations in the field, including the management of solid waste generated. However, multiple reports indicate that licensing control does not regulate liquid waste disposal from patient excretions to protect personnel and the community from radiopharmaceutical exposure. One of the radiopharmaceuticals commonly used in NM and having the longest half-life among the radiopharmaceuticals used in NM is iodine 131(I-131). Thus, this study used a high-purity germanium detector to measure iodine-131 (I-131) activity in liquid waste from decay tanks, temporary collection channels, the hospital's wastewater treatment plant (WWTP) outlet, and six points around the NM service and liquid waste treatment unit. Concentration measurements in three decay tanks were carried out sequentially every 12 h for 3 d, corresponding to the therapy period. The results showed that the I-131 activity levels in the decay tanks and temporary collection channels, before being mixed with liquid waste from other units, were 95.9 × 106 ± 4.4 × 106 Bq m−3. At the point where the liquid waste from other units was mixed, the activity level decreased significantly to 472 680 ± 22 160 Bq m−3, which was below the clearance level of 107 Bq m−3. However, the recorded concentration exceeded the standard for environmental radioactivity at the hospital's WWTP outlet, namely 37 670 ± 2040 Bq m−3. The measurement results for I-131 in the air in the open space for two nuclear buildings was above the standard at 1.3 ± 0.27 Bq m−3. According to the RESRAD simulation, based on the initial dose taken from the liquid waste treatment outlet point, the accumulation of doses and the risk of cancer among workers and the community decreased within 3 months after the maximum exposure.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 4.0 license. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
1. Introduction
Cancer remains the primary or secondary cause of death before the age of 70 in 112 out of 183 countries and ranks third or fourth in 23 other countries. The incidence and mortality burden of cancer is increasing rapidly globally, due to aging and population growth [1]. According to the Globocan Report published by the World Health Organization in 2020, the prevalence of cancer worldwide was 9.2 million cases, resulting in 4.4 million deaths [2]. In Indonesia, the prevalence of cancer was 946 088 cases, with thyroid cancer being the most common type and affecting 38 650 people in the last 5 years [3]. The current standard therapy for thyroid cancer involves total or partial thyroidectomy followed by I-131 therapy [4]. The administration of I-131 therapy after total thyroidectomy through iodine-131 (I-131) aims to reduce the risk of recurrence as well as detect metastatic lesions. After the absorption of the I-131, the remaining tissue is destroyed by the radiation, which is the desired outcome [5].
Radioiodine therapy is part of the broader speciality of nuclear medicine (NM), in which radioactivity is administered to patients to diagnose or treat various diseases [6–8]. In the process, I-131 therapy in patients produces solid and liquid waste. The production of this waste is an unavoidable side effect of radioiodine therapy (as well as NM in general). Solid waste comes from the equipment used, while liquid waste is the result of excretion from patients during therapy.
As an example, the Department of NM at the University of Cologne used a closed tank-stack system to collect patient waste and measure NaI(Tl)scintillation counters to reduce I-131 activity to <1 Bq l−1 [9]. Another study in Oman used two isolation rooms and two underground concrete tanks to treat liquid waste from NM patients, with submersible pumps and an ultrasonic system. The maximum flow rate was 3.7 MBq s−1 with an average monthly concentration of 22.2 MBq m−3 [10]. Advanced technology is also being developed in the handling of radiopharmaceutical waste in a study using graphene oxide (GO) with varying concentrations before filtration with a micro-pore filter paper. The remaining radioactivity in the water under the filter paper is calculated after 15–30 min. Measurements are repeated on the fourth, eighth, twelfth, and sixteenth days, which is significant for the natural decay of I-131 radionuclides. The remaining radioactivity in the water decreases during the experiment with GO concentration. The GO:I-131 mixture (sediment formed on the filter paper) is analysed using field emission scanning electron microscopy (FESEM) and energy dispersive x-rays (EDX) for morphological and elemental analysis. FESEM images showed that the highest concentration of GO produced strong agglomerate morphology. EDX displayed I-131 as well as other elements that were attracted to the GO-coated panel. The results showed that GO has a high adsorption capacity for removing radionuclides. This ability is associated with the number of functional groups containing oxygen on the surface or edge [11]. Although this technology is still in the analysis stage, it has a positive outlook for managing liquid waste containing radioiodine. The use of delay and decay tanks in the management of liquid waste from the excretion of patients on I-131 therapy is the simplest method to decay radionuclide activity used in NM, considering that the radionuclide used has a fairly short half-life. By treating liquid waste in delay and decay tanks for a certain period of time, it is hoped that the liquid waste that will then be channelled to the hospital's waste water treatment plant (WWTP) is below the clearance level and can be processed as general waste. The main approaches to managing low-level radioactive liquid waste are 'delay and decay', 'concentrate and contain', as well as 'dilute and disperse' [12]. For radioactive wastes containing only radionuclides with half-lives measured in days or weeks, such as some medical and research isotopes, storage for weeks or months eliminates the radioactivity and converts the radioactive waste into a waste of low or negligible radioactivity. The general rule-of-thumb is that a waste stored for 10 times the half-life of the primary radionuclide is a waste of low or negligible radioactivity. Such storage reduces the radioactivity by about a factor of 1000. For other radioactive materials, a period of storage reduces the radioactivity and heat generation and, in turn, reduces transport and disposal site costs and risks [13].
In Indonesia, the development of NM technology can be seen from the utilization permits issued by Nuclear Energy Regulatory Agency (NERA) in 2021, which show a 30% increase in the last 10 years for facilities in 18 hospitals in Indonesia. The increase in cancer prevalence, particularly thyroid cancer, and NM service caused an increment in the amount of contaminated radio-pharmaceutical waste. NM waste can be solid or liquid, and the solid form is often obtained from the production of radioisotopes, syringes, patients clothing, pillows, and sheets. Meanwhile, the liquid form comes from patients bodily fluids [14]. The refuse from NM patients' excrement enters the sewerage system via decay/delay tanks, then enters the hospital's WWTP system, and is discharged into the environment via urban drainage.
One of the suboptimally supervised NM wastes in Indonesia is liquid waste, which can be in the form of vomit, urine, blood, and feces. To address this issue, NERA has emerged regulations governing radiation safety in NM through rules related to workers and environmental safety. This can be achieved by setting clearance values, namely the safe concentration of radioactive activities for domestic radioactive waste with an I-131 content of 107 Bq m−3 [15]. Furthermore, the standard values for the maximum limit of radionuclide activity concentration in the environment for I-131 is 2.7 × 10−2 Bq m−3 in air and 6.7 × 103 Bq m−3 in water bodies [16].
The reporting of license holders is not an obligation of radioiodine therapy patients waste producers to fulfil the needed requirements. This indicates that the management cannot be justified in terms of safety aspects. Control of the capacity of radioiodine therapy patients waste treatment is only carried out through document evaluation during the stage of construction permit application. The blueprint of NM facility development plan is used to calculate the maximum capacity of service load based on the equipment/unit owned at the time of application, coupled with the nuclear WWTP, which can vary at each hospital. This indicates that reporting of clearance and standard values for environmental radioactivity levels need to be included in NM service operation requirements. Therefore, this study aims to determine the effectiveness of processing radioiodine therapy patients excretory waste and the potential risks associated with radioiodine concentrations in hospital WWTP outflows.
2. Material and method
2.1. Area of study
This study was carried out in the NM unit of a referral hospital in West Java, Indonesia. The unit utilized two adjacent buildings in its service operations, with building one being old and the waste piping system blueprint was no longer available. Meanwhile, the second was a new six-story building that utilized the basement as the location for NM service. The study focus was on the management of radioiodine therapy patient's excreta in both places. In the NM installation of building one, liquid waste was not directed to the hospital's centralized WWTP, while in NM installation of building two, the waste was temporarily settled before entering the hospital's WWTP. I-131 Therapy is carried out in buildings one and two, adjusted for the availability of isolation beds in each building. In general, the workload of therapy places can be seen from the weekly patient data tabulation in each of the following buildings:
There are 14 isolation rooms in building one that are equipped with a variety of treatment options for patients in building two's liquid waste. The waste treatment in building one is terminated at the decay tank located in the parking lot, and it does not go on to the hospital's WWTP. Building two has four isolation rooms, each with its own advanced waste treatment system that connects to the hospital's WWTP, which ultimately empties into local rivers. Because of issues with water seepage on the walls of the NM room, the infiltration well serves the purpose of a well to manage the runoff of surface water that is caused by rain. This problem was caused by the NM room. In order to determine whether or not there is a leak in the decay tank located in building two, measurements of I-131 activity were taken in the infiltration well.
As depicted in figure 1, decay tank A receives waste from the isolation and post-injection rooms; decay tank B receives waste from the hot lab and four uptake rooms; and decay tank C may receive waste from patients who do not understand the recommendations for excretion procedures after and/or while waiting for patient discharge, causing radioiodine concentrations in the main sewage pit.

Figure 1. Water an air sampling point.
Download figure:
Standard image High-resolution image2.2. Environmental sampling method
Sampling was carried out on liquid and air waste around the NM unit. Furthermore, the number of sampling points was determined using a systematic method. The process was performed by considering the flow and storage of patients waste from points A to I and from points 1–6 for liquid and air samples, respectively, as shown in figure 1.
Liquid waste was collected using the WS750 Wastewater-Stormwater Sampler with a 1 l Marinelli beaker tube container based on the required capacity for contaminated sample analysis for radionuclide counters. Iodine-131 therapy with a dose above 1110 MBq requires 3 × 24 h until the patient can be discharged, resulting in two therapy terms per week. The weekly therapy schedule begins on Monday with a scheduled patient release on Wednesday. The second term begins on Wednesday afternoon with a scheduled patient release on Friday. At storage tanks A, B, and C, sampling was carried out in sequence every 12 h, starting at 12 h on the first day of therapy and ending at 48 h (day a term of therapy I-131). At locations D to I, sampling was performed only at 48 h to determine the settling or flow of waste containing I-131.
Air samples were taken using DFHV-1E High Volume Air Sampler (220–240 VAC) with a Charcoal filter and was counted on the high-purity germanium (HPGe) detector. The procedure of extraction efficiency determining CH3I-131 follows the American Standard for Testing and Materials (ASTM D 3803-79, 1979). Determination of CH3I-131 absorption efficiency of an activated charcoal filter is done at a temperature range of 30 °C–45 °C, the flow rate of 13 lpm to 26.3 lpm, and air humidity of 30%–90%. Sampling medium at locations marked 1–6, as shown in figure 1. These six points have the potential for the spread of I-131 in the air due to their proximity to the service unit and the temporary processing site of patient's liquid waste.
2.3. I-131 counting method (HPGe)
Equipment used for measuring radionuclides in wastewater was a gamma spectrometer counting system with an Ortec HPGe detector. The system consisted of an HPGe detector placed in a 10 cm thick shielding system. Furthermore, the pre-amplifier was attached to the detector body. The amplifier, HV bias supply, and multi-channel analyser were integrated into a single module called DespecPro. The gamma spectrometer system was operated with Maestro or Gamma Vision software, as schematically shown in figure 2. The device was calibrated with a standard mixed source consisting of radionuclides Co-60, Ba-133, Cs-134, Cs-137, Pb-210, and Am-241 that were traceable to the IAEA. Prepared samples were then placed in containers, such as vials or Marinelli beaker, labelled, and wrapped in plastic to prevent contamination. The radionuclide concentration in the sample was measured using a gamma spectrometer equipped with an HPGe detector calibrated using a standard source [17].

Figure 2. HPGe detector.
Download figure:
Standard image High-resolution imageCalibrating energy and efficiency used equations [18]:
Standard source decay,

With:
 :activity during counting (Bq)
:activity during counting (Bq)
 : initial activity (Bq)
: initial activity (Bq)
 : delay time (days)
: delay time (days)
T: half-life (days)
Energy calibration,

With:
Y: gamma energy (keV)
a and b: linear constant numbers
X: channel number
Efficiency calibration,

With:
 γ
: counting efficiency (%)
γ
: counting efficiency (%)
Ns : standard count
NBG: background count
ts : standard count time (seconds)
tBG: background count time (seconds)
At : standard source activity at the time of count (Bq)
pγ : gamma energy abundance (%)
To calculate the concentration of radionuclides contained in the sample (CSp), the following equation was used [19]:

With:
CSp: the concentration of radioactive substances in the sample (Bq/lt or Bq/kg)
Cavg: average concentration of radioactive substances in the sample (Bq/lt or Bq/kg)
uT : measurement uncertainty (Bq lt−1 or Bq kg−1)

With:
NSp: sample count rate (cps)
NBG: background count rate (cps)
γ
: efficiency at gamma energy (%)
pγ : yield of gamma energy (%)
WSp: sample volume or weight (lt or kg)

With:
 : sample count uncertainty (%)
: sample count uncertainty (%)
 : efficiency uncertainty at gamma energy (%)
: efficiency uncertainty at gamma energy (%)
 : yield uncertainty (%)
: yield uncertainty (%)
 : sample volume uncertainty (%)
: sample volume uncertainty (%)
k: 1
The minimum detectable concentration (MDC) for a gamma spectrometer system was influenced by counting efficiency, background count rate, and sample weight. To calculate the MDC with a 95% confidence level, the following equation [18] was used

With:
MDC: MDC (Bq/lt or Bq/kg)
NB : background count rate (cps)
tB : background count time (seconds)
γ
: count efficiency (%)
pγ : gamma energy abundance (%)
Fk : self-absorption correction factor (when sample ρ is different from the standard ρ)
w: sample volume or weight (lt or kg)
3. Result
3.1. I-131 activity on liquid waste
The analysis method used for liquid waste samples was Gamma Spectrometry based on SOP 004.003/KL, referring to IAEA Technical Report Series No. 295 and SNI ISO 10703:2009 with the lowest detectable concentration of I-131 at 2.6 × 104 Bq m−3.
As part of the I-131 therapy, three decay tanks (A, B and C) had their liquid waste concentrations read every 12 h for three days. Starting with the first 12 h the patient received I-131 therapy and continuing through the 48th hour with the annotations A1, A2, A3 and A4, as well as tanks B and C, the results are shown in table 1. The fluctuations in the readings of the concentration of I-131 in the waste samples from each sampling point are explained in figure 3(b).
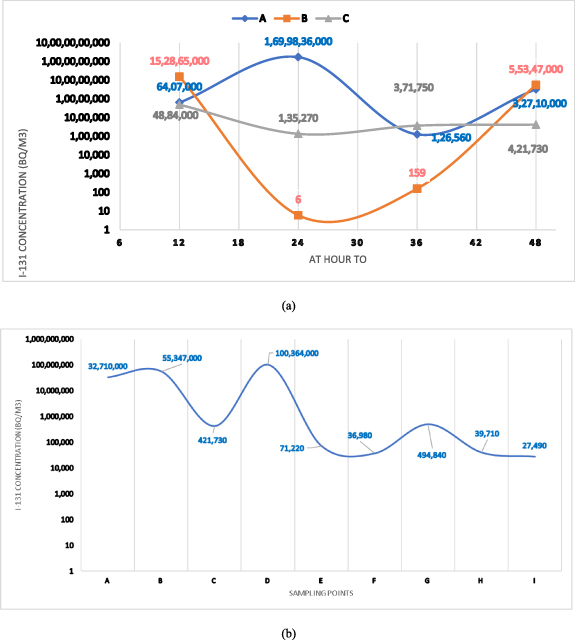
Figure 3. (a) I-131 concentration in three decay tanks of building two (b) fluctuations in the I-131 concentration from upstream to downstream of the liquid waste stream on the 3rd day.
Download figure:
Standard image High-resolution imageTable 1. NM building workload.
| Building | Number of contaminated toilets | Number of isolation bed | Number of hospitalized patients per week |
|---|---|---|---|
| 1 | 7 | 14 | 14–28 |
| 2 | 6 | 4 | 8–16 |
Point (D) was a temporary waste collector for the subsequent flow to point G and ends at H. The absence of deposition/retention of liquid waste at point D indicated that the exposure spread along the path. What is being referred to here is the high concentration of I-131 that may be found in tank D due to the fact that it receives a direct flow from tanks A, B, and C. However, the concentration at point H is higher than the amount that is considered acceptable for radioactivity in the environment. As a result, it is necessary to take action in order to lower the value of the concentration of I-31. The percentage of I-131 removal from liquid waste at point H (WWTP outlet) with the existing NM patients waste treatment system gave a high efficiency. The efficiency from decay tanks was 94% for A to D, 34% for B to D, and 99% for the D processor to the WWTP outlet.
3.2. I-131 Activity in the air
The measurement results of I-131 concentration in the air at six points around NM unit are presented in table 2. Air sampling was carried out at six points around NM buildings one and two, as indicated by numbers 1–6 in figure 1. The I-131 concentration was above the environmental radioactivity standard at points 4, 5 and 6 as shown at figure 4. Furthermore, point 4 was the Hotlab where radiopharmaceutical preparation was performed before therapy services, and 5 was patients isolation room post-therapy. Point 6 was an outdoor location used as a parking lot located between the radiopharmaceutical storage room and the final waste from radioiodine therapy patients isolation room in building one.

Figure 4. I-131 concentrations in the air.
Download figure:
Standard image High-resolution imageTable 2. The concentration of I-131 liquid waste.
| I-131 Concentration (in 103) | |
|---|---|
| Sampling points | Bq m−3 |
| A1 | 6126 ± 281 |
| A2 | 1625 285 ± 74 551 |
| A3 | 120.71 ± 5.85 |
| A4 | 31 275 ± 1435 |
| B1 | 146 153 ± 6712 |
| B2 | 5747 ± 264 |
| B3 | 152 163 ± 6980 |
| B4 | 52 918 ± 2429 |
| C1 | 4669 ± 215 |
| C2 | 128.89 ± 6.38 |
| C3 | 354.99 ± 16.76 |
| C4 | 402.95 ± 18.78 |
| D | 95 962 ± 4402 |
| E | 67.68 ± 3.54 |
| F | 35.08 ± 1.90 |
| G | 472.68 ± 22.16 |
| H | 37.67 ± 2.04 |
| I | 26.01 ± 1.48 |
Similar studies have been carried out in other countries to analyse the safety of NM waste management, particularly from patients excretions. Spain was one of the countries that have implemented reporting requirements for permission values and environmental radioactivity monitoring. Furthermore, monitoring was carried out by requiring every NM waste-generating facility to report the measurement results of radionuclide concentration values before entering the municipal WWTP system. Other controls were also carried out by taking samples in seven hospitals WWTP in the Barcelona Metropolitan Area from effluents and dried sludge.
The process was then continued with measurement of the concentration of I-131, Tc-99 m, In-111, Ga-67, and I-123 using gamma spectroscopy, which showed values of 0.2–4.4 Bq l−1 for I-131 and 5–50 Bq l−1 for Tc-99 m. Other samples were taken from municipal WWTP in the metropolitan Barcelona area, which received wastewater from several hospitals in the city. The results showed the maximum concentration found for each radionuclide in wastewater and sludge, and the activity levels were still below the specified limit [20]. Another method was carried out in Malaysia, which has also implemented reporting requirements for monitoring the results of NM waste management in waste-generating facilities. This method was carried out by measuring the exposure rate around the radio-pharmaceutical waste processor at a distance of 1.2–3 m from the collection tanks. The highest exposure rate was 177.00 µR h−1 (1552 µSv h−1) in a full ward condition for two consecutive weeks, which exceeded the community dose limit. An increase in I-131 activity from the samples used caused fluctuations of 10–25 mCi or 37 × 107–92.5 × 107 Bq [21]. A previous study showed differences in the effectiveness of using waste processing systems in reducing the activity concentration of radionuclides originating from NM. Furthermore, the number of patients affected the effectiveness of the processing system. NM building one is a three-story building built in 1970 with simple maintenance, both for the building and the WWTP which uses the overflow method in three holding tanks for patients waste treatment.
3.3. Radiation exposure risk analysis from I-131 concentration at point H using RESRAD
From the measurement results of I-131 concentration at point H, which was the WWTP outflow towards the urban drainage system and/or municipal water supply, a scenario model of exposure to the public through consumed groundwater, vegetables/fruits, and inhalation was performed. Due to its physicochemical properties, I-131 can easily enter the environment due to problems in standard operating procedure treatment or waste management. The exposure pathways can be described by the following scenario in figure 5.
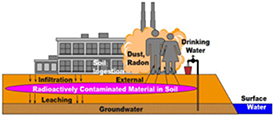
Figure 5. A scenario of exposure route I-131 through surface water [22]. Reproduced from [22]. CC BY 4.0.
Download figure:
Standard image High-resolution imageThe concentration at point H, which was the discharge point of the hospital wastewater treatment, showed a value above the environmental radioactivity standard. The scenario was based on the assumption that WWTP effluent entered the urban drainage system flowing into a river with a distance of 0.5–2 km from point H.
The river became a source for the water company and provided irrigation water for the surrounding communities. Therefore, the community, directly and indirectly, consumed materials containing I-131. The risk assessment was performed assuming a 'single' release of I-131 through the WWTP effluent of the hospital for a 24 hour period, with data gathered from measurements of I-131 concentrations in 4 decay tanks in the NM department. This highlights the significance of I-131 monitoring in hospital WWTPs prior to the discharge of fully treated effluent.
The initial activity concentration value at point H was 0.04 Bq l−1 or 37 670 Bq m−3. The graph enlargement of the cumulative dose analysis through RESRAD ONSITE is shown in figure 6.
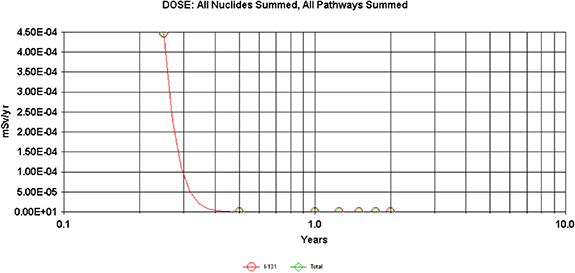
Figure 6. Dose analysis within 10 years for I-131 and its derivatives Xe-131 m.
Download figure:
Standard image High-resolution imageThe I-131 dose was at its highest value in the middle of the 2nd and 3rd months and continued to decline. The cancer risk analysis results with the assumption that the community consumed water, vegetables, and possibly ingested materials containing I-131 are shown in figure 7. Figure 7 shows a decline in cancer risk for workers and the community after the 2nd month. The risk calculation performed by RESRAD was accomplished in the low-dose-rate program and risk factor. It was assumed that there was a linear relationship between dose and risk extrapolated from high-dose and dose-rate data.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 7. Cancer risk analysis for I-131 and its derivatives Xe-131 m.
Download figure:
Standard image High-resolution image{kind=link}
Another extrapolation method into the low-dose range can produce higher or lower estimates of cancer likelihood. However, studies on humans exposed to low doses were not sufficient to show the actual level of threat. According to the Committee on Interagency Radiation Research and Policy Coordination (CIRRPC), there was a scientific uncertainty on cancer risk in the low-dose range below epidemiological knowledge and the possibility that the likelihood cannot be ruled out (CIRRPC 1992). One radiological risk assessment method used a dose conversion factor (DCF) to estimate the cost-effective dose equivalent.
3.4. Analysis of the radiation exposure risk from the I-131concentration in the air
The measurement results in figure 5 showed that point six was above the environmental radioactivity standard value for air, namely 2.7 × 10−2 Bq m−3. Considering that I-131 was classified as a radionuclide in the high radiotoxicity group due to its ability to be inhaled as a gas or ingested through food or water, and its solubility in water/alcohol, it was directly absorbed with an effective dose per unit intake by adult age at 2.0 × 10−3 Sv/Bq. Risk analysis of exposure to workers using air sample test data was carried out by calculating the dosage received by workers annually using the conversion factor for I-131, with the results shown in table 3. It was taken into consideration that the places where concentrations of iodine-131 were found that exceeded the standard level of environmental radioactivity were hot lab rooms and patient isolation rooms where medical workers work full time 8 h day−1, and parking areas where parking workers work an average of 4 h day−1 considering the fact that parking attendants move around or even work in shifts. Based on this information, scenarios were created for two distinct work periods. The dose received at the 3 far air sampling points was below the limit value determined for radiation workers and the public namely 20 mSv y−1 and 1 mSv y−1 respectively as shown at table 4.
Table 3. I-131 concentrations in the air.
| Sampling point | I-131 Concentration (Bq m−3) | Standard value of environmental radioactivity (Bq m−3) |
|---|---|---|
| 1 | 0.027 | 0.027 |
| 2 | 0.027 | |
| 3 | 0.027 | |
| 4 | 19.06 | |
| 5 | 30.28 | |
| 6 | 1.57 |
Table 4. Exposure dose rate from the inhalation route.
| I-131 concentration | Inhalation rate for worker [20] for 8 h work | Inhalation rate for worker [20] for 4 h work | I-131 DCF | Dose (8 h worker) | Dose (4 h worker) | |
|---|---|---|---|---|---|---|
| Sampling point | Bq m−3 | m3 y−1 | m3 y−1 | mSv Bq−1 | mSv y−1 | mSv y−1 |
| Hot lab | 19.06 | 11 400 | 5700 | 0.000 0076 | 1.651 3584 | 0.825 6792 |
| Isolation room | 30.28 | 11 400 | 5700 | 0.000 0076 | 2.623 4592 | 1.311 7296 |
| Parking area | 1.57 | 11 400 | 5700 | 0.000 0076 | 0.136 0248 | 0.068 0124 |
4. Conclusion
The waste treatment system for radioiodine therapy patients met the clearance level limit for I-131, but the final waste output exceeded the standard limit of environmental radioactivity in Indonesia. Furthermore, the air concentration of I-131 in the parking area adjacent to the waiting room for patients and hospital visitors was above the standard limit of environmental radioactivity levels. Based on this finding, further analysis is needed on the possibility of leaks in the I-131 therapy service room and the infiltration well that served as the final reservoir for the three decay tanks in building one. This is necessary because workers in the area are non-radiation workers, such as parking attendants, non-radiation nurses, and hospital visitors.
The radiation dose received through the air at the three points, namely the Hotlab, the isolation room in building one, and the parking area, was below the limit for workers and the public. However, this dosage was only from the inhalation pathway. The possibility of receiving exposure from other pathways, such as external and ingestion is still high depending on the range of everyone's work area. Risk analysis using RESRAD ONSITE showed the safety of the radiation exposure dose rate and cancer risk for workers and the public, with the assumption that the I-131 concentration in the WWTP effluent does not increase.
Acknowledgments
This study was funded by the University of Indonesia Postgraduate PUTI program with Contract Number NKB-342/UN2.RST/HKP.05.00/2022.
Data availability statement
All data that support the findings of this study are included within the article (and any supplementary files).