
Abstract
OBJECTIVE: To understand the role of written advance directives (ADs) in medical decision making through examination of qualitative and quantitative data sources. We specifically wanted to address whether physicians unilaterally disregard advance directives.
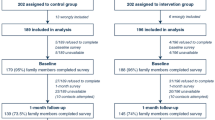
DESIGN: Block randomized controlled trial to improve decision making and outcomes of seriously ill patients.
SETTING: Five academic medical centers.
PATIENTS: Fourteen hospitalized, seriously ill adults were randomized to receive an intervention of patient-specific information on prognoses and specially trained nurse to facilitate decision making. To be included in this analysis, patients reported having an AD and also met one of these criteria of severity; were comatose, had objective estimate of prognosis for surviving 2 months of 40% or less, or died during this hospital admission.
MEASUREMENTS AND MAIN RESULTS: Quantitative data sources consisted of medical record review and interviews with the patient (when possible), surrogate, and responsible physician about prognosis, symptoms, preferences, and decision making. Qualitative data consisted of narratives by the nurse responsible for counseling and facilitating decision making. Each element of the quantitative database was reviewed, and a timeline of communication and decision making was constructed. Qualitative data were analyzed using grounded theory and narrative summary analysis. We compared and contrasted qualitative and quantitative data to better understand the role of ADs in decision making. In each case, the patient had a period of diminished capacity in which ADs should have been invoked. Advance directives played an important role in decision making of 5 of 14 cases, but even in those cases, life-sustaining treatment was stopped only when the patient was “absolutely, hopelessly ill.” In two of these cases, the family member wrongly reported that the patient had an AD, and in the remaining seven cases, ADs had a limited role. The limited role could not be traced to a single explanation. Rather, a complex interaction of several factors was identified: patients were not considered hopelessly ill, so the directive was never seen as applicable and a transition in the goals of care did not occur; family members or the designated surrogate were not available, were ineffectual, or were overwhelmed; or the content of the AD was vague, or not applicable to the clinical situation, and the intent in completing the AD was never clarified. A physician did not unilaterally disregard a patient’s preference in any of the cases. Two factors that enhanced the role of the AD were an available surrogate who was able to advocate for the patient and open communication between the physician and the surrogate in which the patient’s prognosis was reconsidered.
CONCLUSIONS: Our findings indicate that physicians are not unilaterally disregarding patients’ ADs. Despite the patients’ serious illnesses, family members and physicians did not see them as “absolutely, hopelessly ill.” Hence, ADs were not considered applicable to the majority of these cases. Cases in which Ads had an impact evidenced open negotiation with a surrogate that yielded a transition in the goals of care.
Article PDF
Similar content being viewed by others


References
Weeks WB, Kofoed LL, Wallace AE, Welch HG. Advance directives and the cost of terminal hospitalization. Arch Intern Med. 1994;154:2077–83.
Chambers CV, Diamond JJ, Perkel RL, Lasch LA. Relationship of advance directives to hospital charges in a Medicare population. Arch Intern Med. 1994;154:541–7.
Thomasma DC. Functional status care categories and national health policy. J Am Geriatr Soc. 1993;41:437–43.
Schneiderman LJ, Kronick R, Kaplan RM, et al. Effects of offering advance directives on medical treatments and costs. Ann Intern Med. 1992;117:599–606.
Teno J, Lynn J, Wenger N, et al. Advance directives in end of life decision making: lessons from the Patient Self Determination Act and the SUPPORT Project. J Am Geriatr Soc. 1997;45:500–7.
Murphy DJ, Knaus WA, Lynn J. Study population in SUPPORT: Patients (as defined by disease categories and mortality projections), surrogates, and physicians. J Clin Epidemiol. 1990;43:11S-28S.
The SUPPORT Investigators. A controlled trial to improve outcomes for seriously ill hospitalized patients: the study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment (SUPPORT). JAMA. 1995;274:1591–8.
Knaus WA, Wagner DP, Draper EA, et al. The APACHE III prognostic system: risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100:1619–36.
Teasdale G, Jennett B. Assessment of coma and impaired consciousness: a practical scale. Lancet. 1974;2:81–3.
Cullen DJ, Civetta JM, Briggs BA, Ferrara LC. Therapeutic intervention scoring system: a method for quantitative comparison of patient care. Crit Care Med. 1974;2:57–60.
Glaser BG, Strauss AL. The Discovery of Grounded Theory: Strategies for Qualitative Research. New York, NY: Aldine DeGruyther; 1967.
Gilligan C. In a Different Voice: Psychological Theory and Women’s Development. Cambridge, Mass: Harvard University Press; 1982.
Mischer E. Research Interviewing: Content and Narrative. Cambridge, Mass: Harvard University Press; 1986.
Maxwell JA. Qualitative Research Design: An Interactive Approach. London, UK: Oxford University Press; 1996.
Inui TS, Frankel RM. Evaluating the quality of qualitative research: a proposal pro tem. J Gen Intern Med. 1991;6:485–6.
Teno JM, Lynn J, Connors AF, et al. The illusion of end-of-life resource savings with advance directives. J Am Geriatr Soc. 1997;45:513–8.
Teno JM, Licks S, Lynn J, et al. Do advance directives provide instructions which direct care? J Am Geriatr Soc. 1997;45:508–12.
Morrison RS, Olson E, Mertz KR, et al. The inaccessibility of advance directives on transfer from ambulatory to acute care settings. JAMA. 1995;274(6):478–82.
Teno JM, Lynn J. Putting advance care planning into action. J Clin Ethics. Fall 1996:100–8.
Teno JM, Nelson HL, Lynn J. Advance care planning: priorities for ethical and empirical research. Hastings Cent Rep. 1994;24(suppl):S32-S36.
Emanuel L. Structure advance planning: is it finally time for physician action and reimbursement? JAMA. 1995;274(6):501–3.
Author information
Authors and Affiliations
Additional information
The opinions and findings in this manuscript are those of the authors and do not necessarily represent the views of its sponsors.
This research was made possible by funding from the Robert Wood Johnson Foundation’s Program on the Care of Critically-III Hospitalized Adults: The Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatment (SUPPORT) and from grant 1 RO1 HS07075 from the Agency for Health Care Policy and Research.
This effort would not be possible without the dedication and fortitude of the intervention nurses of the SUPPORT project.
Rights and permissions
About this article
Cite this article
Teno, J.M., Stevens, M., Spernak, S. et al. Role of written advance directives in decision making. J GEN INTERN MED 13, 439–446 (1998). https://doi.org/10.1046/j.1525-1497.1998.00132.x
Issue Date:
DOI: https://doi.org/10.1046/j.1525-1497.1998.00132.x