
Abstract
Data sources Sources were the Cochrane Oral Health Group Trials Register, the Cochrane Central Register of Controlled Trials, MEDLINE and EMbase. Relevant journals and bibliographies of papers and review articles were hand-searched and experts and companies conducting clinical research on ceramic restorations were also contacted.
Study selection Randomised controlled trials (RCT) were included where longevity of ceramic inlays was compared with that of other posterior restorations.
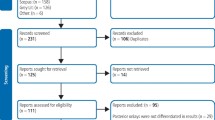
Data extraction and synthesis Screening of possible studies and data extraction were independently conducted by two reviewers (MH and AY) using a specially designed chart. Authors of studies were contacted for additional information. The methodological quality of studies was assessed in duplicate using individual components. The Cochrane Oral Health Group statistical guidelines were followed and the results expressed as odds ratios and 95% confidence intervals for dichotomous outcomes.
Results Only one study was eventually included, which evaluated the clinical performance of 60 ceramic inlays and 20 gold inlays for 5 years. Seven of the 60 ceramic inlays and two of the 20 gold inlays failed at 5-year review. No ceramic inlays resulted in postoperative pain/discomfort after the treatment, but one gold inlay did. The power of the included study was not great enough to detect any important difference in longevity and postoperative pain or discomfort between ceramic and gold inlays.
Conclusions There is no strong evidence available to support any differences in the clinical performance of ceramic inlays and other posterior restorations. There are a limited number of well-designed clinical trials within this research area. Greater attention to the design and reporting of studies should be given to improve the study quality of ceramic restoration trials.
Similar content being viewed by others

Commentary
Systematic reviews developed according to the methodological rigour of the Cochrane Collaboration format leave little room for criticism of the procedural steps leading up to the authors' conclusions. Nevertheless, the authors choose to include only RCT, which severely limited the scope of possible trials. Only one such trial was included, which does not allow any general statements to the made about clinical performance. The authors described the lack of studies as disappointing and recommend that more well-designed trials should be carried out. The question is whether this is realistic, given the indications and contraindications for using ceramics intraorally.
Restoring posterior teeth with ceramic inlays is relatively limited, in spite of ceramics being among the oldest restorative materials we have. This relates to restoration, following caries destruction, to salvage remaining tooth tissue and not to, improving the smile (posteriorly). The positive side of ceramic restoration is that ceramics are highly biocompatible and can be made to match tooth colour perfectly. Unfortunately, they are also brittle. The consequence of this is that extensive tooth preparation is required, contrasting with modern restorative thinking where minimal-intervention dentistry is favoured. Moreover, the techniques for producing and for placing well-fitting intracoronal ceramic inlays are time-consuming and highly technique-sensitive. The novelty of modern ceramics is the wider spectrum of production possibilities, that is, there is traditional sintering, cast- and/or pressed- as well as infiltrated-ceramics. Innovative concepts for machining prefabricated ceramic blocks are constantly being developed and some new, interesting, high-strength ceramics have emerged. These have the potential to reduce the need for removal of tooth substance to reach a necessary minimum thickness of the inlay.
There is a disturbing trend emerging in dentistry reflected by a recent paper stating, “Our patients have a higher dental IQ than those of the past, more disposable income, and are demanding conservative, aesthetically pleasing, non-metallic restorations.” I am not so sure if this would be the case if the dentist were to describe the option, “Yes, we can restore the tooth with something that looks very nice, but I will have to remove more sound tooth structure than would otherwise be necessary, it will probably last a fraction of the time of the alternatives and it is rather expensive because it is technically complicated to create.”
Ethically, one cannot carry out clinical trials unless there is equipoise about a working hypothesis. Based on our current knowledge about material properties and the data from a limited number of mostly short-term cohort studies, is there any reason to assume that a ceramic inlay will perform better than another restorative material with respect to longevity? I think not. It is also very probable that publication bias exists regarding the clinical performance of ceramics. Moreover, it should always be the informed patient who should decide on the choice of treatment. Given that patients are provided with adequate and correct information, although perhaps not described as pointedly as above, is it likely that they will consent to being randomised into a group where an alternative non-ceramic, or even a metallic, restorative material is to be used? Again, I think not. Because of this I do not believe there will be numerous RCT published on the topic in the future, the exception perhaps being comparisons between conventional and, hopefully, new higher-strength ceramics.
Practice point
-
Little evidence is available that supports any difference in clinical performance of ceramic inlays and other posterior restorations.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Emma Tavender, Review Group Co-ordinator, Cochrane Oral Health Group, University Dental Hospital of Manchester, Higher Cambridge Street, Manchester M15 6FH, UK. E-mail: emma.tavender@man.ac.uk
Hayashi M, Yeung CA. Ceramic inlays for restoring posterior teeth (Cochrane Review). The Cochrane Library 2003; Issue 1. Oxford: Update Software
Rights and permissions
About this article
Cite this article
Jokstad, A. No evidence supports differences in clinical performance of ceramic inlays and other posterior restorations. Evid Based Dent 4, 31 (2003). https://doi.org/10.1038/sj.ebd.6400174
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400174
