
Abstract
The digital healthcare (DH) system has recently emerged as an advanced rehabilitation approach that promotes rehabilitation training based on virtual reality (VR) and augmented reality (AR). The purpose of this meta-analysis study is to review and assess the impact of DH systems on pain and physical function among patients diagnosed with knee joint pain. Between January 2003 and September 2023, studies that met the listed inclusion criteria were gathered from Scopus, PubMed, Web of Science, and EBSCO databases. The analysis of standardized mean difference (SMD) was carried out with 95% confidence interval (95% CI) (PROSPERO registration number: CRD42023462538). Nine research papers were selected, which collectively involved 194 males and 279 females. The meta-analysis outcomes revealed that DH intervention significantly improved balance (SMD, 0.41 [0.12, 0.69], p < 0.05) and pain level (SMD, − 1.10 [− 2.02, − 0.18], p < 0.05). The subgroup analysis of the pain level showed varied outcomes for the TKA (SMD, − 0.22 [− 0.49, 0.04], p = 0.10) or OA patients (SMD, − 2.80 [− 3.83, − 1.78], p < 0.05) Next, this study found no significant effect of DH intervention on knee joint range of motion (ROM) (SMD, 0.00 [− 0.76, 0.76], p = 1.00) and walking velocity (SMD, 0.04 [− 0.22, 0.29], p = 0.77) in patients with knee joint pain. The meta-analysis review conducted in this study revealed that DH intervention may potentially improve balance among the patients with knee joint pain. It may also alleviate the pain level particularly among OA patients.
Similar content being viewed by others

Introduction
Total knee arthroplasty (TKA) and knee osteoarthritis (OA) are the main causes of knee joint pain. Besides limiting knee movement, these knee-related issues cause atrophy of muscles around the knee joint and severely affect the function of knee joint1. Knee injuries can potentially trigger serious fibrous exudate and fibrin in the interstitial space deposited in the knee joint cavity, which can further lead to fibrous adhesion2. Long-term immobilization due to knee pain induces osteoporosis, causes muscle atrophy, articular cartilage nutritional disorder, and fibrosis3,4,5. In addition, joint cavity stenosis may occur as the synovial sacs dry up stemming from prolonged immobilization of the knee joints6.
The digital healthcare (DH) system has recently emerged as an advanced rehabilitation approach that promotes rehabilitation training based on virtual reality (VR) and augmented reality (AR). In VR games, real-like worlds are simulated by using interactive computer settings to improve the daily activities of patients or their functional movements7. This is achievable by deploying AR technology that superimpose computer-generated virtual objects on real images to yield real-world simulations8. The patients are given a unique avatar that represents their body movements7 to interact with the virtual environment by using specific devices or with body movements. Apart from offering a sense of reality, telerehabilitation integrated with AR enhances postural perception by enabling simultaneous real-time interaction with virtual objects (in the virtual world) and physical settings (in the real world)9.
Prior studies10,11 revealed that DH systems effectively improved pain and body function recovery in patients suffering from knee joint pain when compared to standard rehabilitation (SR) techniques. For example, Nambi et al.11 compared the pain level and physical function of the knee among OA patients subjected to 4 weeks of VR games training and SR training, with 20-min five sessions per week. The study disclosed significant improvement in knee joint movements and pain levels after implementing VR training when compared to the outcomes derived from SR training. On the contrary, other studies12,13 reported that DH systems had no impact on TKA patients. Therefore, the efficacy of DH systems to rehabilitate knee joint pain remains debatable.
A meta-analysis study7 showed that VR games could alleviate pain levels in chronic neck pain and shoulder impingement syndrome, but its effect on knee joint pain was not disclosed. Therefore, this present meta-analysis study systematically reviewed and assessed the impact of DH systems on pain and physical function among patients diagnosed with knee joint pain.
Methods
Study selection and data collection
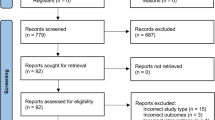
The protocol for this meta-analysis review was registered in the PROSPERO database (CRD42023462538) on September 21, 2023. As depicted in Appendix A, two researchers were responsible for the search strategy and manuscript preparation by adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. The search strategy was executed by identifying articles published between January 1, 2003, and September 20, 2023, from four electronic databases, namely EBSCO, PubMed, Scopus, and Web of Science. We chose to search for studies from the past 20 years14 because the number of published studies on digital healthcare systems has been continuously increasing from 2003 (Pubmed: 199 studies) to 2023 (Pubmed: 4321 studies). The following keywords were used to search through the databases: “Knee”, “Training”, “Exercise”, “Virtual reality”, and “Augmented reality”. Subsequently, the screening process (title and abstract) was performed by two independent investigators. The selected full articles were re-screened based on the inclusion and exclusion criteria set for this study. The two independent investigators conducted a quality assessment and a data extraction process for articles that met the inclusion criteria. All data were retrieved from the published literature. In the event of any dispute regarding the status of an article, another independent investigator was invited to weigh in on the decision until a consensus was achieved. The respective reference was acquired manually once a study inclusion was confirmed. Figure 1 illustrates the article selection protocol deployed in this study.

Flow diagram of the search results using the preferred reporting items for systematic reviews and meta-analysis (PRISMA).
Inclusion and exclusion criteria
The article selection was performed by adhering closely to the following inclusion criteria: (1) patients with knee joint pain, (2) studies that conducted the randomized controlled trial (RCT) approach, (3) either VR or AR training was assigned to the DH group, while SR training was assigned to the SR group (examples of SR interventions: knee joint stretching, strength, and balance training), (4) pre- and post-training analyses that included pain level, balance, walking velocity (WV), and range of motion (ROM) of knee joint, (5) findings expressed in median (interquartile range) or mean ± standard deviation, (6) articles published between January 2003 and September 2023, and (7) articles written in English. The only exclusion criterion for article selection in this review refers to articles derived from grey literature.
Quality assessment
The quality of the selected articles was determined by using the Cochrane risk of bias assessment tool15. The assessed quality aspects comprised of blinding of outcome assessment, participants and personnel blinding, allocation concealment, incomplete data, random sequence generation, and selective reporting16. Each article was given a score of “yes”, “no” or “unclear”. Two co-authors independently (L.G. and S.L.) assessed the quality of each study, whereas another author (S.X.) facilitated the decision-making upon any disagreement.
Data extraction
Based on the previous research paradigm17, the content to be extracted was formulated, and the extracted content was optimized through the studies included in the initial search10,13. Details from each included study were extracted and tabulated, such as age, gender, disease type, DH device, training duration, index, traditional training (TR) and DH protocol (see Table 1). Data extraction was performed independently by two co-authors (L.G. and S.L.) Any disagreement was resolved by another researcher (S.X.)
Data analysis
The meta-analysis was performed by using the Review Manager (RevMan) software (version 5.4.1, Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2020) to assess the impact of the interventions. The standardized mean difference (SMD) was selected as the most suitable effect scale index after considering that the reviewed articles recorded continuous variable outputs with varying test methods. Next, median (range) data were standardized by converting them into mean ± standard deviation18. In cases where data were not disclosed, the authors of the respective articles were contacted by email to gather clarifications.
When more than five studies displayed a similar indicator, the sensitivity analysis was carried out by excluding each study in sequence to assess the stability of the meta-analysis outcomes. Study heterogeneity was applied to examine I2 statistics. A small I2 indicates low heterogeneity between studies, whereas an I2 below 50% implies homogeneous studies. In the current review, a fixed effect model was applied for data analysis. On the contrary, I2 ≥ 50% suggests heterogeneous studies, thus the random effect model will be applied for data analysis19. The publication bias was evaluated by using funnel plot, while the SMD was evaluated by using the Forest plot. Finally, the uncertainty level was calculated at 95% CI.
Results
Eligibility of studies
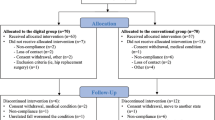
The systematic review was conducted based on nine RCT articles that met the inclusion criteria. Each included study indicated ethical approval of the study protocol from the respective institutions. Two independent co-authors reported a high consistency level with each other (Cohen kappa coefficient = 0.89) during the screening process. Out of the 473 patients from the included articles, 194 were males and 279 were females. As for group division, 246 and 227 patients were assigned to DH and SR groups, respectively. Six studies used VR tools for DH training, while three studies used AR technology. The shortest intervention time was 10 days and the longest was 12 weeks.
Quality assessment
The overall quality of the nine articles was relatively high, with most of the articles displaying a low risk of bias (69.9%) (Fig. 2). Meanwhile, a small percentage of the articles were highly biased (9.5%) and the remaining articles appeared to be unclear (20.6%).

Analysis of risk of bias according to Cochrane Collaboration guideline.
Quantitative synthesis
The effects of DH and SR groups on balance were compared in four10,13,20,21 included articles (see Fig. 3a) while the pain level (see Fig. 3b) were compared in seven10,11,12,13,21,22,23 included articles. Apparently, the meta-analysis for balance (SMD, 0.41 [0.12, 0.69], p < 0.05, I2 = 0%, p for heterogeneity = 0.64) and pain level (SMD, − 1.10 [− 2.02, − 0.18], p < 0.05, I2 = 95.6%, p for heterogeneity < 0.05) showed that enhanced balance was more prevalent in the DH group than in the SR group. The subgroup analysis of the pain level showed varied outcomes for the TKA (SMD, − 0.22 [− 0.49, 0.04], p = 0.10, I2 = 0%, p for heterogeneity = 0.72) and OA (SMD, − 2.80 [− 3.83, − 1.78], p < 0.05, I2 = 68%, p for heterogeneity = 0.08) patients.

Forest plot illustrates the effects of TR versus DH intervention on balance (a) and pain level (b).
The effects of DH and SR groups on ROM were compared in three13,21,22 included articles (see Fig. 4a), while the WV (see Fig. 4b) were compared in four10,12,13,24 included articles. Interestingly, the meta-analysis detected an insignificant variance in the ROM (SMD, 0.00 [− 0.76, 0.76], p = 1.00, I2 = 81%, p for heterogeneity < 0.05) and WV (SMD, 0.04 [− 0.22, 0.29], p = 0.77, I2 = 21%, p for heterogeneity = 0.29) between the DH and SR groups.

Forest plot illustrates the effects of TR versus DH intervention on ROM (a) and WV (b).
Publication bias analysis
This review includes 9 studies, which is close to the minimum requirement for using funnel plots. Publication bias can be reflected to some extent, and the presence of small sample publication bias has also been noted in previous studies14,16,25. As illustrated in Figs. 5 and 6, the publication bias analysis showed that the analysis yielded a left–right symmetrical distribution that indicated a low probability of publication bias.

Funnel plot of publication bias for balance (a) and pain level (b) in the TR versus DH intervention.

Funnel plot of publication bias for ROM (a) and WV (b) in the TR versus DH intervention.
Sensitivity analysis
The meta-analysis revealed no significant changes in each group after the analysis type was modified, the impact size was changed, and the individual studies were excluded. Thus, the sensitivity analysis showed that the research results were reliable.
Discussion
This study assessed the impact of DH systems on balance, pain, ROM, and WV in patients suffering from knee joint pain. Notably, the DH systems were more effective in enhancing balance and lowering pain levels in patients diagnosed with knee joint pain than ROM and WV. Despite the insignificant impact of DH systems on TKA patients in the subgroup analysis, patients with knee OA may benefit significantly from such approach. A previous study also reported that the DH systems effectively improved pain in patients with from burn injuries26. These findings denote the varying impacts of the DH systems on different populations. The reasons for the varied DH system performance, however, remain unclear.
The two main objectives of post-knee joint surgery rehabilitation are to relieve pain and facilitate knee function recovery, such as body weight support, balance, ROM, and WV. The deterioration of muscles, ligaments, tendons, and meniscal tissues surrounding the knee joint can adversely affect the postural balance of the patients27. As evidenced in the literature, the declining balance ability may lead to an increased risk of falling22. Therefore, the long-term functional outcomes depend on one’s ability to maintain balance. Based on the meta-analysis findings, DH systems may improve the balance ability of patients with knee joint pain more effectively than SR techniques.
For example, Ozlu et al.10 performed a VR game intervention on patients with knee OA five times a week for three weeks. The study showed that the balance ability of the participants in the DH group improved significantly when compared to those in the SR group. In addition, the study highlighted that DH systems may improve patients’ balance through visual and auditory stimuli10. Increased muscle strength and decreased pain level were also associated with improved balance, especially when DH systems were integrated21.
Several studies pointed out that rehabilitative training in either VR or AR offers immersive and multi-sensory effects that enable patients to experience sufficient distraction that minimizes pain sensation28 and enhances physical performance29. The concept of cognitive distraction refers to the primary working mechanism of the DH systems that regulates pain management and improves physical ability30. During DH systems training, patients actively participate in an immersive experience and hardly perceive stimulation beyond their field of attention, including pain. Pain sensation is generated in the thalamus region of the human brain, which is one of the most important anatomical structures that receive projections from multiple ascending pain pathways. Pain perception is also processed in the thalamus region before the information is transmitted to the corresponding cerebral cortex region. Next, the thalamus manages the pain-related factors, such as sensory discrimination (lateral pain pathway) and emotional motivation (internal pain pathway) components31. Another study showed that training in a virtual environment regulates the pain input intensity from the outside at the thalamus level before the cerebral cortex detects the sensory input32. Apart from the pain reduction mechanism via VR training, the DH systems may minimize significantly the bio-physiological parameters related to distress, particularly in declining the heart rate33. This exemplifies the positive impact of DH systems on pain reduction, which serves as an analgesic effect on the relevant psychological variables.
This review is limited by several apparent drawbacks. First, the nine selected articles were considered a small sample size and may not represent the entire population. Second, non-intervention as a control group is not possible in RCT for clinical population, thus we are only able to compare the impacts between DH and SR groups. Moreover, the intervention plans of both the DH and SR groups in each study were inconsistent due to the purpose of each respective study, thus hampering this present review to perform horizontal comparisons of individual included studies. Therefore, future work should include more well-designed articles to strengthen the meta-analysis findings. Finally, as it has not been found that DH intervention has a positive impact on ROM and WV, caution should be exercised when choosing DH intervention for patients who want to improve ROM and WV.
Conclusion
The meta-analysis showed that the DH system may provide a significant impact on both pain and body function in patients with knee joint pain, in comparison to the standard rehabilitation. The DH system may improve the balance ability of patients with knee pain. Also, interventions that integrated the DH system may alleviate the pain level, particularly among OA patients. However, more RCTs with bigger sample size are required to ensure that these results are homogenous and applicable in health policies.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Change history
27 February 2024
A Correction to this paper has been published: https://doi.org/10.1038/s41598-024-55342-9
References
Reddy, S. S., Vaish, A. & Vaishya, R. Fracture in an arthrodesed Charcot’s knee joint. BMJ Case Rep. 14, e246529 (2021).
Usher, K. M. et al. Pathological mechanisms and therapeutic outlooks for arthrofibrosis. Bone Res. 7, 9 (2019).
Gailey, R. Review of secondary physical conditions associated with lower-limb amputation and long-term prosthesis use. J. Rehabil. Res. Dev. 45, 15–30 (2008).
Bamman, M. M. et al. Muscle inflammation susceptibility: A prognostic index of recovery potential after hip arthroplasty?. Am. J. Physiol. Metab. 308, E670–E679 (2015).
Wang, M. et al. Knee fibrosis is associated with the development of osteoarthritis in a murine model of tibial compression. J. Orthop. Res. 39, 1030–1040 (2021).
Kim, J., Kim, Y., Cho, K.-J. & Kim, K. Development and preclinical trials of a novel steerable cannula for 360° arthroscopic capsular release in minimally invasive surgery. In 2020 42nd Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC) 4890–4890 (IEEE, 2020). https://doi.org/10.1109/EMBC44109.2020.9175681.
Gumaa, M. & Rehan Youssef, A. Is virtual reality effective in orthopedic rehabilitation? A systematic review and meta-analysis. Phys. Ther. 99, 1304–1325 (2019).
Milgram, P., Takemura, H., Utsumi, A. & Kishino, F. Augmented reality: A class of displays on the reality-virtuality continuum. In Telemanipulator and Telepresence Technologies (Das, H., ed.) 282–292 (1995). https://doi.org/10.1117/12.197321.
Portalés, C., Lerma, J. L. & Navarro, S. Augmented reality and photogrammetry: A synergy to visualize physical and virtual city environments. ISPRS J. Photogramm. Remote Sens. 65, 134–142 (2010).
Ozlu, A., Unver, G., Tuna, H. İ & Menekseoglu, A. K. The effect of a virtual reality-mediated gamified rehabilitation program on pain, disability, function, and balance in knee osteoarthritis: A prospective randomized controlled study. Games Health J. 12, 118–124 (2023).
Nambi, G. et al. Comparative effects of virtual reality training and sensory motor training on bone morphogenic proteins and inflammatory biomarkers in post-traumatic osteoarthritis. Sci. Rep. 10, 15864 (2020).
Pournajaf, S. et al. Effect of balance training using virtual reality-based serious games in individuals with total knee replacement: A randomized controlled trial. Ann. Phys. Rehabil. Med. 65, 101609 (2022).
Shim, G. Y. et al. Postoperative rehabilitation using a digital healthcare system in patients with total knee arthroplasty: A randomized controlled trial. Arch. Orthop. Trauma Surg. 143, 6361–6370 (2023).
Xie, S., Li, S. & Shaharudin, S. The effects of combined exercise with citrulline supplementation on body composition and lower limb function of overweight older adults: A systematic review and meta-analysis. J. Sports Sci. Med. 22, 541–548 (2023).
Higgins, J. P. T. et al. Cochrane Handbook for Systematic Reviews of Interventions (Wiley, 2019). https://doi.org/10.1002/9781119536604.
Li, S. et al. Effects of high-intensity interval exercise on cardiac troponin elevation when comparing with moderate-intensity continuous exercise: A systematic review and meta-analysis. PeerJ 11, e14508 (2023).
Li, S., Ng, W. H., Abujaber, S. & Shaharudin, S. Effects of resistance training on gait velocity and knee adduction moment in knee osteoarthritis patients: A systematic review and meta-analysis. Sci. Rep. 11, 16104 (2021).
Hozo, S. P., Djulbegovic, B. & Hozo, I. Estimating the mean and variance from the median, range, and the size of a sample. BMC Med. Res. Methodol. 5, 13 (2005).
Li, Y. et al. Efficacy and safety of tripterygium glycoside in the treatment of diabetic nephropathy: A systematic review and meta-analysis based on the duration of medication. Front. Endocrinol. (Lausanne) 12, 25 (2021).
Hadamus, A. et al. Assessment of the effectiveness of rehabilitation after total knee replacement surgery using sample entropy and classical measures of body balance. Entropy 23, 164 (2021).
Yu, J.-H., Nekar, D. M., Kang, H.-Y., Lee, J.-W. & Oh, S.-Y. Comparison of physical activity training using augmented reality and conventional therapy on physical performance following a total knee replacement: A randomized controlled trial. Appl. Sci. 13, 894 (2023).
Gianola, S. et al. Effects of early virtual reality-based rehabilitation in patients with total knee arthroplasty. Medicine (Baltimore) 99, e19136 (2020).
Li, L. Effect of remote control augmented reality multimedia technology for postoperative rehabilitation of knee joint injury. Comput. Math. Methods Med. 2022, 1–8 (2022).
Hadamus, A. et al. Effectiveness of Early rehabilitation with exergaming in virtual reality on gait in patients after total knee replacement. J. Clin. Med. 11, 4950 (2022).
Lu, Y., Wang, W., Ding, X. & Shi, X. Association between the promoter region of serotonin transporter polymorphisms and recurrent aphthous stomatitis: A meta-analysis. Arch. Oral Biol. 109, 104555 (2020).
Carrougher, G. J. et al. The effect of virtual reality on pain and range of motion in adults with burn injuries. J. Burn Care Res. 30, 785–791 (2009).
Anwer, S., Alghadir, A., Zafar, H. & Al-Eisa, E. Effect of whole body vibration training on quadriceps muscle strength in individuals with knee osteoarthritis: A systematic review and meta-analysis. Physiotherapy 102, 145–151 (2016).
Spiegel, B. et al. Virtual reality for management of pain in hospitalized patients: A randomized comparative effectiveness trial. PLoS One 14, e0219115 (2019).
Nekar, D. M., Kang, H. Y. & Yu, J. H. Improvements of physical activity performance and motivation in adult men through augmented reality approach: A randomized controlled trial. J. Environ. Public Health 2022, 3050424 (2022).
Wang, Y., Guo, L. & Xiong, X. Effects of virtual reality-based distraction of pain, fear, and anxiety during needle-related procedures in children and adolescents. Front. Psychol. 13, 842847 (2022).
Ab Aziz, C. B. & Ahmad, A. H. The role of the thalamus in modulating pain. Malays. J. Med. Sci. 13, 11–18 (2006).
Lier, E. J., Oosterman, J. M., Assmann, R., de Vries, M. & van Goor, H. The effect of virtual reality on evoked potentials following painful electrical stimuli and subjective pain. Sci. Rep. 10, 9067 (2020).
Chirico, A. et al. virtual reality in health system: beyond entertainment. A mini-review on the efficacy of VR during cancer treatment. J. Cell. Physiol. 231, 275–287 (2016).
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this Article was revised: The original version of this Article contained an error in the Abstract. “Eight research papers were selected, which collectively involved 194 males and 279 females.” now reads: “Nine research papers were selected, which collectively involved 194 males and 279 females.”
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Guo, L., Li, S., Xie, S. et al. The impact of digital healthcare systems on pain and body function in patients with knee joint pain: a systematic review and meta-analysis. Sci Rep 14, 3310 (2024). https://doi.org/10.1038/s41598-024-53853-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-53853-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
