
Abstract
HIV continues to be a serious global public health concern, having 40.4 million lives up to now and continuing to spread throughout all countries. The objective of this study was to identify predictors for viral load suppression among HIV positive adults under ART treatment in University of Gondar Comprehensive Specialized Hospital, Ethiopia. An institution based retrospective cohort study design was carry out from 30th March 2017–30th March 2022.Accelerated failure time model were employed to get wide-ranging information about adult HIV positive patients. In this study out of 378 study participants, about 77.8% were suppressed viral load count and the rest were censored. The Weibull AFT model results revealed that predictors were older age (φ = 0.774, 95% CI 0.602–0.793), primary educators (φ = 0.931, 95% CI 0.809–0.964), patients disclosed the disease to family member (φ = 1.093, 95% CI 1.001–1.457), viral load < 10,000 copies/mL (φ = 1.153, 95% CI 1.015–1.309), hemoglobin level ≥ 11g/dL (φ = 1.145, 95% CI 1.028–1.275), CD4 cell count ≥ 200 per mm3 (φ = 1.147, 95% CI 1.019–1.290), weight ≥ 50 kg (φ = 1.151, 95% CI 1.033–1.275), BMI between 18.5 and 24.9 kg/m3 (φ = 1.143, 95% CI 1.007–1.296), fair treatment adherence (φ = 1.867, 95% CI 1.778–1.967), good treatment adherence (φ = 1.200, 95% CI 1.046–1.377), advanced WHO clinical stages (φ = 0.923, 95% CI 0.899–0.946), patients with OCC (φ = 0.821, 95% CI 0.720–0.936) and substance use (φ = 0.876, 95% CI 0.773–0.993) statistically significant predictors for viral load suppression at 5% level of significance. Then, near intensive care of adult patients’ whose ages between 25 and 34 years, primary educational level, advanced WHO clinical stage, patients with OCC, and substance users can help them improve their health and live longer. Lastly, further studies should be done on HIV positive adult patients by considering other important independent variables that were not included in this study.
Similar content being viewed by others

Introduction
HIV continues to be a serious global public health concern, having 40.4 million lives up to now and continuing to spread throughout all countries. By the end of 2022, there were an estimated 39.0 million HIV-positive individuals worldwide, with 25.6 million of them individuals living in Africa. An estimated 660,000 people acquired by HIV in 2022 and 380,000 deaths with HIV-related causes1. Ethiopia has also one of the largest HIV infected population among sub-Saharan Africa countries with an estimated 691,362 people were living in 20192.
Antiretroviral therapy (ART) aims to improve the prognosis and quality of life for patients living with HIV3 by reducing the rate of disease occurrence, progression, mortality4, and morbidity5. This successful ART leads to high chance of HIV viral load suppression 6 and undetectable levels of virus in both improving individual health and halting onward. Initial viral load testing in people with HIV should be measured after 6 months of initiating ART and every one year thereafter routinely. Patients viral load count less than or equal to 1000 copies per mL, which implies that HIV is controlled by the current ART regiment and also commonly referred to as having a suppressed viral load count7.
The 90–90–90 targets were introduced in 2014 by the Joint United Nations and they set a goal of 90% of all HIV-positive individuals being diagnosed, 90% of those being diagnosed receiving ART, and 90% of those receiving treatment achieving viral load suppression by 20208. However, world health organization recommends viral load monitoring to ensure viral load suppression is achieved and maintained, but large gaps in global access remain, particularly in low- and middle-income countries9.
Ethiopia adopted the global 90–90–90 target which is part of the strategies designed to eliminate HIV/AIDS epidemics by 2030 and has been working with many collaborators and stakeholders in improving disease detection, viral load testing and adherence on antiretroviral therapy2. However, in different studies of Ethiopia viral load suppression is very far from achieving the UNAIDS 90–90–90 target. For instance, the suppression rate of viral loads is 80.9% in Arba Minch and 72% in the eastern Shewa zone, respectively10,11.
Numerous studies have been conducted on the clinical and sociodemographic parameters influencing HIV viral load suppression. Among them some of the studies indicated that the predictors, like marital status, baseline CD4 cell count, baseline viral load < 10,000 copies per mL, baseline Cotrimoxazole preventive therapy (CPT), baseline Isoniazid preventive therapy (IPT) and good adherence level to ART10,11, Poor treatment adherence12, alcohol drinking, non- disclosure of HIV status13, and duration of ART14 were considered as predictors that affects viral load suppression among adult HIV patients.
Additionally, the current study site is near to Bahir Dar, one of Ethiopia's HIV-positive districts, and a significant number of HIV patients visit in university of Gondar comprehensive specialized hospital. Then, there is scarcity of study have been done by Weibull accelerated failure time (AFT) model among HIV patients in these study area. Consequently, the present study conducted by Weibull AFT model to analysis survival time to viral load suppression. Therefore, the objective of this study was to identify predictors for viral load suppression among HIV positive adults under ART treatment in University of Gondar Comprehensive Specialized Hospital (UGCSH), Ethiopia.
Material and methods
Data source The source of data for this study is secondary data source because the study participant is adult HIV positive patients who registered and under follow-up from 30th March 2017 to 30th March 2022.
Study design A retrospective cohort study design was conducted on adult HIV positive patients registered at University of Gondar comprehensive specialized Hospital.
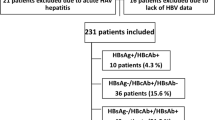
Procedure of choosing study participants Patients didn’t have full recorded information regarding viral load count and unknown patents follow up status were excluded. The survival time of these patients after treatment was determined, and patients transfer out, loss to follow-up, death, and still alive at the end of study time were considered censored. Finally, for this study there are 378 study participants were selected based on the above criteria (Fig. 1).

Sample size determination conceptual frame work among adult HIV positive patients.
Data collection procedure The data collection procedure was based on patient's chart and electronic database system. Patient charts were selected by using their medical registration number (MRN) of patients and the necessary information (socio demography, behavioral and clinical variable) was retrieved from patient charts by trained ART data clerks.
Data quality: In order to ensure the quality of collected data, two day intensive training was given for ART data extractors based on the objective of this study. All extraction processes are overseen by data extractors. During data extraction, ART data management and the principal investigator checked the checklists for completeness and consistency daily.
Response variable The response variable for this study was survival time to viral load count suppression of HIV positive patients. In this study, viral load count ≤ 1000 copies per mL can be classified suppressed and viral load count unsuppressed > 1000 copies per mL.
Independent variables Gender, age in years, residence, marital status, religion, level of education, disclosure status, and substance use, CD4 cell count per mm3, baseline viral load count in copies per mL, hemoglobin level in g/dl, weight in kg, body mass index (BMI) in kg per m3, WHO clinical stage, Adherence, Functional status, ART regiment, other comorbid condition (OCC), and Opportunistic infection(OIs) other than TB were considered as independent variables that were expected to be the predictors for the time to viral load suppression among HIV positive patients.
Kaplan–Meier estimator
The figure in Kaplan–Meier survival curves shows if the pattern of one survivorship function lying above another, which means the group defined by the upper curve had more favorable survival experience than the group defined by the lower curve. However, it is unlikely to detect a difference when survival curves cross each other.
Cox proportional hazards model
In Cox proportional hazards (PHs) regression model, the measure of effect is the hazard rate, which is the risk of failure (i.e., the risk of suffering to suppressed viral load count), given that the participant has survived up to a specific time. According to PHs assumption, the effect of a covariate is to increase or decrease the hazard by a proportionate amount which does not depend on any time (t). These indicated that the baseline hazard is a function of t but does not involve any predictor (X’s), whereas the exponential expression involves the X’s but does not involve t. Then, the Cox PHs model can be formulated as;
where \({\text{h}}\left({\text{t}},\mathrm{ X},\beta \right)\) the hazard function, \({h}_{o }\left(t\right)\) is the unspecified baseline hazard function and represents the hazards when all of the independent variables \({X}_{1} , {X}_{2 },{X}_{3 }{\cdots \cdots X}_{P}\) included in the model equal to zero. \({{\varvec{\beta}}}^{\boldsymbol{^{\prime}}}={(\beta }_{1} ,{\beta }_{2, } {\beta }_{3} \dots \dots {\beta }_{P } )\) is a vector of unknown regression coefficients and \({X=X}_{1} , {X}_{2 },{X}_{3 }{\cdots \cdots X}_{P}\) is a vector of time-fixed covariates. This hazard function is the product of two functions: The function \({h}_{o }\left(t\right)\) characterizes how the hazard function changes as a function of survival time and also the other function, \(expx{\prime}\beta \) characterizes how the hazard function changes as a function of subject covariates15.
Checking assumption of proportional hazard (PH) model
Before proceeding with other survival statistical model, it is obligatory to check PH assumptions. PHs assumption can be tested by using GLOBAL test. Small p-values indicate PH assumption holds rejected under the null hypothesis.
Accelerated failure time model
Accelerated Failure Time (AFT) model is an alternative modeling frameworks to the PH model for the analysis of survival time data when the PH assumptions don’t satisfies16. Under AFT models we measure the direct effect of the explanatory variables on the survival time instead of hazard. This characteristic allows for an easier interpretation of the results because the parameters measure the effect correspondent covariates on the mean survival time15. Suppose \({x}_{1},{x}_{2},{x}_{3}\dots \dots \dots \dots ..{x}_{p}\) explanatory variables recorded for each individual in a study. According to the general AFT model, the hazard function of the \({i}\)th individual is then,
where \({h}_{o}({\text{t}})\) is the baseline hazard function and \(\eta i\) is the acceleration factor that is a ratio of survival times corresponding to any fixed value of \({h}_{i}\left(t\right)\).
The acceleration factor is given according to the formula where \(\eta i={\beta }_{1}{x}_{1i}+{\beta }_{2}{x}_{2i}+\cdots \cdots \cdots {\beta }_{P}{x}_{pi}\) is the linear component of the model in which \({x}_{ji}\) is the value of \({j}^{th}\) explanatory variable \({X}_{j}\) for the \({i}^{th}\) individual. According to the relationship of survival function and hazard function, the survival function for an individual with p covariates is given by: \({S}_{i}(t)\)=\({S}_{o}(t/{e}^{\mathrm{\eta i}})\). The factor \({\eta }_{i}\) is telling us how a change in covariate values changes the time scale from the baseline time scale. Depends on the nature of the data different forms AFT models considered like: Weibull, log-logistic and log normal AFT model.
Model selection criteria
Model Selection criteria are crucial to compare the AIC and BIC values in order to determine which survival model are more appropriate for HIV patient’s data. Finally, the model with the lowest AIC and BIC values among these data is appropriate model.
Univariable variable selection
First selected each covariates at 25% level of significance and statistically significant covariates were selected for multivariable analysis. The data were analyzed with statistical R software version 4.1.3.
Model diagnostics checking
The plots of Cox‐Snell residuals can also be used in the graphical valuation of the adequacy of a fitted model. Thus, the plot of Cox-Snell residuals should give a straight line with unit slope, zero intercept and indicated the fitted model is good.
Ethics approval and consent to participate
A statement to confirm that all methods were performed in accordance with the ethical standards as laid down in the declaration of Helsinki. Hence, an informed consent was waived by Bahir Dar University research technical and ethical review board with Ref.no Stat-S/166/2022 G.C by reason of retrospective nature of the study. The study was approved by Bahir Dar University research technical and ethical review board.
Results
Among the 378 active participants in this study, 131 (66.1%) had a baseline CD4 cell count greater than 200 cells/mm3, and 184 (73.6%) of them had suppressed viral load during the study period. Similarly, 255 (67.5%) of the baseline viral load counts less than 10,000 copies per milliliter, of which 230 (90.2%) had suppressed viral load. On the other hand, among the 198 (52.4%) individuals whose hemoglobin level greater than 11g/dl had 146 (73.7%) suppressed viral load. Regarding weight and body mass index (BMI) of patients, 220 (58.2%) and 172(45.5%), had weight less than 50 kg and BMI greater than or equals to 25 kg/m2 respectively, of which 81.4% and 85.1% had suppressed viral load. In terms of the participants' functional status, 260 (68.8%), 86 (22.8%), and 70 (8.5%) were ambulatory, working, and bedridden respectively. 139 (36.8%) of the study subjects had clinical stage II, of which 101 (72.7%) experienced viral load suppression. Among the 145(38.4%) patients treated with 1e ART medication, 86.9% had suppressed viral load. 78.3% of patients with good treatment adherence had viral load suppressed. On the other hand, patients with-out other comorbid condition (OCC) and opportunistic infections (OIs) other than TB had 79.9% and 83.0% suppressed viral load (Table 1).
Over half of the patients in this study (65.3%) were female, and 71.1% of them suppressed viral load during the study period. In terms of patient ages in years, 188 (49.7%) patients were primarily between the age groups between 25 and 34 years; only 81.4% of these participants had a suppressed viral load. Additionally, 33.6% patients lived in rural areas and 66.4% in urban areas. Likewise, 106 (75.2%) of the 141 (45.2%) married participants had suppressed VL. In terms of religion, 275 (72.8%) had adherents to an orthodox faith, and of them, more than half (82.5%) suppressed viral load. In terms of religious status, 275 (72.8%) were followers of an orthodox religion, and of these, more than half (82.5%) had a suppressed viral load. Out of the total, 132 (34.9%) had secondary education, and 80.3% of them reduced the viral load. Similarly, 310 (82.0%) and 247 (65.3%) of the patients disclosed their status to family members and substance users, respectively. Of these, more than half (82.0%) and 65.3% suppressed the viral load (Table 2).
Survival status of adult HIV positive patients
Out of 378 adult HIV patients, 84 (22.2%) were censored and 294 (77.8%) had a suppressed viral load. The mean and median survival times, which were 34.9 and 36.0 months respectively, had standard errors of 0.8 and 1.6 (Table 3).
Kaplan Meier estimate of the survival function
According to Kaplan–Meier survival curves, the overall survivor function in this study declined monotonically as the patient's time in month increased. I.e. as the patient's time in month increased, the adult HIV positive patients' survival probability demolishes (Fig. 2).

Adult HIV positive patients Kaplan–Meier plot survival function.
Kaplan–Meier Curve for baseline hemoglobin level, CD4 cell count, adherence, and OCC
Patients with hemoglobin levels less than 11 g/dL and CD4 counts less than 200 cells/mm3 had a longer survival time than those patients with than hemoglobin level ≥ 11 g/dl and CD4 cell count ≥ 200 cells/mm3. Similarly, patients with poor adherence to treatment and OCC had longer survival time than those in the corresponding categories. i.e. The Kaplan–Meier survival curve suggested that the above curves are lower risk of suppression than their counterparts (Fig. 3).

Kaplan–Meier Survival curve for baseline hemoglobin level, CD4 cell count, adherence, and OCC.
Evaluation of proportion hazard assumption
First we want to check the proportional hazard assumption before trying to any AFT model. The goodness of fit test gives a significant global p-value is less than 5% (Table 4). Since, in this study the global null hypothesis suggested that the proportionality assumption is rejected, and leads to PH model is unsuitable. As a result, we have used the AFT model, to analyze the survival time to viral load suppression for adult HIV positive patients.
Accelerated failure time (AFT) model fitting
In the univariable AFT model analysis related to time to viral load suppression, the covariates age in years, educational status, residence, disclosure, baseline viral load, hemoglobin level, CD4 cell count, weight, body mass index, adherence, WHO clinical stage, ART regiment, OCC, and substance use are statistically significant. In contrast, gender, religion, marital status, and functional status are not significant at a 25% level of significance. A multivariable AFT mode is used to reanalyze all of the chosen univariable covariates.
Comparison of AFT models
According to the model comparison criterion, the Weibull accelerated failure time model AIC and BIC values were minimal. Thus, the Weibull accelerated failure time model is a better baseline distribution than the others model for the data set of adult HIV positive patients (Table 5).
Results of multivariable Weibull accelerated failure time model
Table 6 displays the multivariable Weibull accelerated failure time model results. The survival time to viral load suppression of HIV positive patients between the ages of 25 and 34 years was decelerated by a factor of 0.774 (φ = 0.774, 95% CI 0.602–0.793). The survival time to viral load suppression of patients with primary education was 0.931 (φ = 0.931, 95% CI 0.809–0.964) less than that of non-educators. Disclosure status of patients is a significant predictor of time to viral load suppression, and patients disclose the disease to family members are at a higher risk of viral load suppression as compared to non-disclosure with an acceleration factor of 1.093 (φ = 1.093, 95% CI 1.001–1.4570). In terms of initial viral load count, those with < 10,000 copies/mL had a higher survival time to viral load suppression for HIV positive with an acceleration factor of 1.153 (φ = 1.153, 95% CI 1.015–1.309) than those with Viral load count ≥ 10,000 copies/mL. Patients who had a hemoglobin level of ≥ 11 g/dL and a CD4 count of ≥ 200 cells/mm3 were substantially linked to poor patient survival, with a factor of 1.147 (φ = 1.147, 95% CI 1.019–1.290) and 1.145 (1.145) (φ = 1.145, 95% CI 1.028–1.275). In a similar way, patients who weight more than 11 kg and had a BMI between 18.5 and 24.9 kg/m2 were found to be substantially more likely to have poor HIV patient survival, with corresponding acceleration factors of 1.151 (φ = 1.151, 95% CI 1.033–1.275), and 1.143 (φ = 1.143, 95% CI 1.007–1.296). Considering survival time to viral load suppression of a fair treatment adherence group of patients was significantly associated with poor survival as compared to poor treatment adherence. This is revealed by a time ratio of less than one (0.867) (φ = 0.867, 95% CI 0.778–0.967) indicating a larger survival time and lower risk of viral load suppression. On the other hand, a time ratio more than one (1.2) (φ = 1.200, 95% CI 1.046–1.377) indicating a lower survival time and higher risk of viral load suppression. Individuals with OCC had a considerably longer survival time, with a roughly one-times (φ = 0.821, 95% CI 0.720–0.936) lower survival time viral load suppression. HIV patients' time to viral load suppression is significantly predicted by substance use, and those who use drugs have a somewhat lower chance of suppression than those who do not use 0.876 (φ = 0.876, 95% CI 0.773–0.993) (Table 6).
Overall goodness of fit
The blue line in the Cox–Snell residual plot displayed the model diagnosis with 95% confidence interval (CI) for the Kaplan–Meier estimate of the Cox-Snell. The blue line represents the survival function of the unit exponential distribution, while the black solid line is the Kaplan–Meier estimate of the survival function of the residuals (with the dotted lines corresponding to the 95% pointwise confidence intervals). This finding showed that the adult HIV positive patient's data suited the Weibull AFT model effectively (Fig. 4).

Cox–Snell residual plots for the Weibull AFT model of adult HIV patients.
Discussion
In this retrospective analysis, 77.8% of HIV patients suppressed their viral load while receiving antiretroviral therapy. This aligns with findings from earlier research conducted in Cambodia, which revealed 76.8%17, 89% found in Uganda18, and 93% in Vietnam19. Patients in ages between 25 and 34 years were significant predictors for survival time to viral load suppression. Previous study not supports this result11. These discrepancies could be due to differences in study areas, follow-up periods, and/or hospital facility existence.
Results of the current study revealed that educational level is a significant predictor of time to viral load suppression. This could be primary educators has better chance of understanding the treatment follow up and possible to virally suppressed as compared to non-educators. This study is inconsistent with a study done at Harare City13 and Ethiopia10 which states that primary educators were not independent risk factors for survival time.
The survival time to viral load suppression was higher for HIV patients under disclosed the disease to family member. This could be attributable to the maximizing immunity level of patients at expressed the status of the disease to family member. This study is support with former study conducted in Harare City13, in their results indicated that study participants expressed the status of the disease to family member had a nearly fourfold increased risk of suppression compared to non-disclosure patients. However, this findings were inconsistent with another study conducted in Arba Minch, Ethiopia11, which found that patients under the category of disclosed the disease to family member were not independent predictors to viral load suppression. These differences could be due to sample size, study periods, study area and methods of data analysis.
This study also illustrated that baseline viral load is a significant predictor to time to viral load suppression. Patients with low baseline viral load (< 10,000 copies/mL) experienced the higher viral load suppression than those with high baseline viral load ((≥ 10,000 copies/mL).The result of this study is supported by the findings from other studies11. These findings are not shocking due to the fact that the higher plasma viral load means the larger HIV reservoirs; therefore it takes longer survival time to achieve viral load suppression. Similarly, results of the current study revealed that the time to viral load suppression of patients whose CD4 count ≥ 200 cells/mm3 was shorter than those who have < 200 cells/mm3 CD4 count. This finding agrees the findings of the study conducted in different settings11,19,20. This result predicted that higher CD4 cell counts usually correlate with low viral load concentration and therefore patients take shorter time to viral load suppression.
Furthermore, weight of patients has also an effect on the duration of viral load suppression. The effect of weight on time to viral load suppression might be due to the fact that, weights ≥ 50 kg has a significant reduction in serious bacterial infections and mortality, this improvement correspond to a substantial success in early viral load suppression.
BMI category 18.5–24.9 kg/m2 had increased risk of viral load suppression. The result of this study is consistent with a study done by10. This study also showed that good and fair treatment adherence of patients was onefold higher to experience early viral load suppression as compared to those who have poor treatment adherence. As a matter of fact that adherence is the key, and potentially modifiable predictors associated with time to viral load suppression. The idea of these study is supported by a study done at Uganda18.
In the current investigation also shown WHO clinical stage is predictors for time to viral load suppression. Previous study had confirmed these result, in their findings shown that HIV patients with WHO clinical stage-IV have a viral load suppression than clinical stage-I10. This could be because individuals with advanced WHO clinical stages were more likely to get additional opportunistic infections like TB. However, this study is inconsistent with a study done at Southern Brazil21 and democratic republic of Congo22.
Results of the current study revealed that HIV positive individual users are slightly lower risk than non-users. On the other hand substance drug user patients had poor health status and resulting lower viral load suppression than non-users. This study is inconsistent with the literature10. Similarly, this study also showed that patient with OCC was lower to experience early viral load suppression as compared to patient’s with-out OCC.
Conclusion
In this current study Weibull AFT model was better than the other AFT models. The findings of this study showed that the predictors that were statistically associated with higher time to viral load suppression were patients disclosed the disease to others, baseline virial load count less than 10,000 copies/mL, hemoglobin level ≥ 11 g/dL, CD4 cell count ≥ 200/mm3, weight ≥ 50 kg, body mass index between 18.5 and 24.9 kg/m2, fair and good adherence. The other important predictors were age in year between 25 and 34 years, primary education level, advanced WHO clinical stage, patients with OCC, and substance users statistically associated with lower time to viral load suppression. Then, near intensive care of adult patients’ whose ages between 25 and 34 years, primary educational level, advanced WHO clinical stage, patients with OCC, and substance users can help them in order to enhance their quality of life and extend their lifespan.
Limitation of the study
This study was based on retrospective cohort study design, the data obtained from adult HIV positive patients chart. However, some important socio-demographic and clinical predictors like nutritional status, income status, homeownership, and other hematological parameters like eosinophil, neutrophil, and basophil counts, were not available in participant charts.
Data availability
The data used in the current investigation is available from the corresponding author and can be attached upon request. The data accessed in the current investigation complied with relevant data protection and privacy regulations.
Code availability
All codes organized in this study are available from the corresponding author on reasonable request.
Abbreviations
- AFT:
-
Accelerated failure time model
- AIC:
-
Akaike information criteria
- AIDS:
-
Acquired immune deficiency syndrome
- ART:
-
Antiretroviral therapy
- BIC:
-
Bayesian information criterion
- BMI:
-
Body Mass Index
- CD4:
-
Cluster differentiation 4
- G.C:
-
Gorgerin calendar
- Hgb:
-
Hemoglobin
- HIV:
-
Human immune deficiency virus
- OIs:
-
Opportunistic infections
- PHs:
-
Proportional hazards
- UGSCH:
-
University of Gondar Comprehensive Specialized Hospital
- VL:
-
Viral load
- WHO:
-
World Health Organization
References
World Health Organization. Epidemiological fact sheet HIV statistics, globally and by WHO region (2023).
Ethiopia public health Institute. Current Progress Towards 90–90–90 HIV Treatment Achievement and Exploration of Challenges Faced in Ethiopia June 2020 Addis Ababa Abstract (2020).
Brennan, A. T., Maskew, M., Sanne, I. & Fox, M. P. The interplay between CD4 cell count, viral load suppression and duration of antiretroviral therapy on mortality in a resource-limited setting. Trop. Med. Int. Health 18(5), 619–631. https://doi.org/10.1111/tmi.12079 (2013).
Wasti, S. P., van Teijlingen, E. & Simkhada, P. “Factors influencing adherence to antiretroviral treatment in Asian developing countries: a systematic review. Trop. Med. Int. Health 17, 71–81 (2012).
Volberding, P. A. & Deeks, S. G. Antiretroviral therapy and management of HIV infection. Lancet 376(9734), 49–62. https://doi.org/10.1016/S0140-6736(10)60676-9 (2010).
World Health Organization. Monitoring Response to ART and the Diagnosis of Treatment Failure: Consolidated ARV Guidelines. (2016).
World Health Organization. New WHO Guidance on HIV Viral Suppression and Scientific Updates Released at IAS 2023 (2023).
UNAIDS. 90–90–90: An ambitious treatment target to help end the AIDS epidemic|UNAIDS [Internet]. (cited 1 Sep 2016). United Nations (2014). http://www.unaids.org/en/resources/documents/2014/90-90-90.
World Health Organization. Viral suppression for HIV treatment success and prevention of sexual transmission of HIV (2018).
Ali, J. H. & Yirtaw, T. G. Time to viral load suppression and its associated factors in cohort of patients taking antiretroviral treatment in East Shewa zone, Oromiya, Ethiopia, 2018. BMC Infect. Dis. 19(1), 1–6. https://doi.org/10.1186/s12879-019-4702-z (2019).
Hussen, S. et al. Predictors of time to viral load suppression of adult PLWHIV on ART in Arba Minch General Hospital: A follow up study. Ethiop. J. Health Sci. 29(6), 751–758. https://doi.org/10.4314/ejhs.v29i6.12 (2019).
Wakooko, P., Gavamukulya, Y. & Wandabwa, J. N. Viral load suppression and associated factors among HIV patients on antiretroviral treatment in Bulambuli District, Eastern Uganda: A retrospective cohort study. Infect. Dis. https://doi.org/10.1177/1178633720970632 (2020).
Sithole, Z. et al. Virological failure among adolescents on ART, Harare City, 2017: A case-control study. BMC Infect. Dis. 18, 1–8 (2018).
Joao, E. Factors associated with viral load suppression in HIV-infected pregnant women in Rio de Janeiro, Brazil Factors associated with viral load suppression in HIV-infected pregnant women in Rio de Janeiro Brazil. Int. J. STD AIDS https://doi.org/10.1258/ijsa.2011.010545 (2012).
Collett, D. Modelling Survival Data in Medical Research (Springer, 2003).
Lelisho, M. E. et al. Modeling survival time to death among TB and HIV co-infected adult patients: An institution-based retrospective cohort study. J. Racial Ethn. Heal. Disparities https://doi.org/10.1007/s40615-022-01348-w (2022).
Chhim, K. et al. Factors associated with viral non-suppression among adolescents living with HIV in Cambodia: A cross-sectional study. AIDS Res. Ther. 15(1), 1–10. https://doi.org/10.1186/s12981-018-0205-z (2018).
Bulage, L. et al. Factors associated with virological non-suppression among HIV-positive patients on antiretroviral therapy in Uganda, August 2014-July 2015. BMC Infect. Dis. 17(1), 1–11. https://doi.org/10.1186/s12879-017-2428-3 (2017).
Rangarajan, S. et al. Factors associated with HIV viral load suppression on antiretroviral therapy in Vietnam. J. Virus Erad. 2(2), 94–101. https://doi.org/10.1016/s2055-6640(20)30466-0 (2016).
Diress, G., Dagne, S., Alemnew, B., Adane, S. & Addisu, A. Viral load suppression after enhanced adherence counseling and its predictors among high viral load HIV seropositive people in North Wollo zone public hospitals, Northeast Ethiopia 2019: Retrospective cohort study. AIDS Res. Treat. https://doi.org/10.1155/2020/8909232 (2020).
Pinto, M., Silveira, T. & Draschler, M. D. L. Predictors of undetectable plasma viral load in HIV-positive adults receiving antiretroviral therapy in Southern Brazil. Braz. J. Infect. Dis. 6, 164–171 (2002).
Shah, G. H. et al. HIV viral suppression among people living with HIV on antiretroviral therapy in Haut-Katanga and Kinshasa provinces of Democratic Republic of Congo. Healthcare 10, 1–69 (2022).
Acknowledgements
Author would like to forward their deepest gratitude to all the health staff of the university of Gondar Comprehensive and Specialized Hospital, Ethiopia and also Author would like Bahir Dar University for great contribution of permission letter before data collection.
Author information
Authors and Affiliations
Contributions
N.S.M. was involved in this study from data management, data analysis, drafting, and revising the final manuscript, contributed to the conception, design, and interpretation of data, as well as to manuscript reviews and revisions, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The author declares no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Muhie, N.S. Predictors for viral load suppression among HIV positive adults under ART treatment in University of Gondar Comprehensive Specialized Hospital: retrospective cohort study. Sci Rep 14, 3258 (2024). https://doi.org/10.1038/s41598-024-53569-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-53569-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
