
Abstract
To investigate the incidence rate and risk factors of postoperative delirium in middle-aged and elderly patients with fracture. A total of 648 middle-aged and elderly fracture patients who underwent surgical treatment in our hospital from January 2018 to December 2020 were included in the study, aged 50–103 years, mean 70.10 ± 11.37 years. The incidence of postoperative delirium was analyzed. Univariate analysis was used to screen the risk factors of gender, age, interval between injury and operation, preoperative complications, fracture site, anesthesia method, operation time, intraoperative blood loss, hidden blood loss and hormone use. For the factors with P < 0.05, multivariate logistic regression analysis was used to determine the main independent risk factors. 115 cases (17.74%) of 648 patients had postoperative delirium. Univariate analysis showed that patients with delirium and patients without delirium had significant correlation in age, medical disease comorbidity, fracture type, anesthesia method, operation time and perioperative blood loss (P < 0.05). Multivariate logistic regression analysis showed that age (OR = 1.061), preoperative complications (OR = 1.667), perioperative blood loss (OR = 1.002) were positively correlated with postoperative delirium. It shows that older age, more preoperative complications, longer operation time and more perioperative bleeding are more likely to lead to postoperative delirium; patients with general anesthesia were more likely to develop postoperative delirium than patients with local anesthesia (OR = 1.628); and patients with hip and pelvic fractures are more likely to develop a postoperative delirious state (OR = 1.316). Advanced age, complex orthopedic surgery, more medical comorbidities, general anesthesia and greater perioperative blood loss may be independent risk factors for the development of delirium after internal fixation of fractures in middle-aged and elderly patients.
Similar content being viewed by others
Introduction
With the aging of the world population, the number of middle-aged and elderly orthopedic patients is increasing year by year, and postoperative delirium (POD) is becoming more and more common as a postoperative complication in middle-aged and elderly fracture patients. POD usually occurs 2–3 days after operation, and the incidence of POD in patients over 65 years old is 5–50%. It will not only lead to prolonged hospital stay, increased nursing costs, but also lead to permanent dementia, even life-threatening 1,2,3, and become an important focus of orthopedic physicians. Currently, there are still difficulties in the diagnosis and treatment of POD, especially the lack of effective therapeutic drugs. Therefore, it is urgent to prevent the incidence of POD and shorten the duration of delirium by targeting high-risk patients at an early stage.
Given that the pathophysiological mechanism of POD is still unclear, and there are multiple subtypes in clinical practice, the risk factors leading to its occurrence have not been clarified so far. Therefore, it is important to clarify the mechanism and risk factors of POD and to formulate reasonable prevention and treatment measures to reduce the incidence of POD in middle-aged and elderly fracture patients. In this paper, we retrospectively analyzed the clinical data of 648 middle-aged and elderly (≥ 50 years old) fracture patients who underwent surgical treatment in our hospital between January 2018 and December 2020, counted the incidence of POD, discussed and analyzed the risk factors related to POD in middle-aged and elderly patients with fractures, and provided a basis for the prevention and treatment of POD.
Materials and methods
Inclusion and exclusion criteria
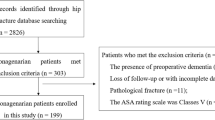
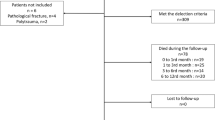
Inclusion criteria: ① age ≥ 50 years old; ② no previous family history of mental illness, no history of mental disorder, no cognitive impairment; ③ clinical symptoms and imaging data were diagnosed as fracture; ④ surgical treatment was performed without contraindication of anesthesia operation; ⑤ no use of drugs that can significantly affect mental activity in the last 1 month; ⑥ no history of heart, brain or lung surgery, no history of paralysis or convulsions.
Exclusion criteria: ① preoperative patients with a clear history of neurological and psychiatric disorders and taking corresponding medications; ② preoperative patients with dementia with cognitive impairment; ③ patients with severe visual or hearing diseases cannot cooperate with the completion of cognitive function tests; ④ patients with conservative treatment of fractures.
General information
A total of 648 patients were included in this study, male 256 cases and female 392 cases; age ranged from 50 to 103 years, mean 70.10 ± 11.37 years; cases of extremity fractures 239, cases of spine fractures 212, and 197 cases of hip and pelvis fractures. 330 cases were combined with medical diseases. The time from injury to surgery ranged from 4 to 72 h, mean 37.35 ± 19.81 h.
Diagnostic criteria for postoperative delirium4
The main diagnosis of POD is based on the American Psychiatric Association's Mental Disorders and Statistics Manual (5th Edition) (DSM-5) and the Ambiguous Consciousness Assessment Method (CAM). The main diagnostic features include acute or subacute attacks, repeated or fluctuating conditions, clinical manifestations of inattention, change of consciousness and decrease of cognitive function (orientation disorder, memory disorder, language disorder). Other features that support the diagnosis of POD include sleep–wake cycle disorders, perceived disorders (hallucinations or misunderstandings, etc.), delusions, improper behavior, emotional instability, etc.
Observation index
Refer to relevant literature research and clinical experience to determine the relevant factors that may affect the occurrence of delirium after orthopedic surgery in middle-aged and elderly patients. Record the patient’s gender, age, interval between injury and operation, preoperative complications, fracture site, anesthesia method, operation time, intraoperative blood loss, hidden blood loss and hormone use, etc.
Statistical methods
SPSS 23.0 statistical software was used for statistical analysis of the data. Measurement data were expressed as mean ± standard deviation, t-test was used for comparison between two groups, and chi-square test was used for count data comparison between two groups. P < 0.05 was considered statistically significant. Finally, all the observed indicators were taken as univariate covariates, and postoperative delirium was taken as the dependent variable, which was taken into the Logistic regression model for multivariate analysis. The 95% confidence interval (CI) was used, and P < 0.05 was considered statistically significant.
Ethical approval and consent to participate
The study was approved by the Institutional Review Board (IRB) of Second Affiliated Hospital of Zhejiang Chinese Medical University (authorization number 2020-KL-040-01), all methods were carried out in accordance with relevant guidelines and regulations. This study was carried out in compliance with the Declaration of Helsinki. Due to the retrospective nature of the study, Second Affiliated Hospital of Zhejiang Chinese Medical University’s IRB waived the need of obtaining informed consent.
Results
Incidence of postoperative delirium
A total 648 of patients met the inclusion and exclusion criteria for inclusion in this study. Postoperative 115 cases of middle-aged and elderly fracture patients developed POD with an overall incidence of 17.74%, including cases of extremity fractures 38, spine fractures 28, and hip and pelvis fractures 49.
Univariate analysis
Univariate analysis showed that the incidence of postoperative delirium in middle-aged and elderly patients with fracture was correlated with age, preoperative complications, fracture type, anesthesia method, operation time and perioperative blood loss, and the difference was statistically significant (P < 0.05). There was no significant correlation with the patient's gender, the interval from injury to surgery, and hormone use, and the difference was not statistically significant (P > 0.05). The specific analysis results are shown in Table 1.
Logistic regression analysis of related factors
The indicators that showed statistical differences in the univariate analysis results were included in the logistic regression model to test the reality. Among them, age, preoperative complications, operation time, perioperative blood loss were positively correlated with the occurrence of POD. This means that the older the age, the more preoperative complications, the longer the operation time, the more perioperative blood loss, the more likely to cause POD. Patients with general anesthesia are also more prone to POD than patients with local anesthesia. The specific analysis results are shown in Table 2.
Discussion
POD is a common surgical complication, especially in middle-aged and elderly surgical patients5, which is harmful to patients and families and affects their prognosis and recovery. The clinical symptoms of postoperative delirium are often difficult to recognize and easy to ignore, requiring keen clinical observation skills. The pathogenesis of postoperative delirium in middle-aged and elderly patients with fractures is still unclear, although some scholars have proposed some theoretical hypotheses, including the inflammatory theory, the neurotransmitter theory, and the theory of altered brain function, which may contribute to the occurrence of postoperative delirium6. However, there is a lack of clinical studies to support them.
Relationship between postoperative delirium and age
At present, most scholars at home and abroad generally believe that advanced age is an independent risk factor for postoperative delirium in middle-aged and elderly patients, especially in patients with hip surgery7,8. Some scholars believe that this may be related to the decline of cholinergic nerves in the brain, the gradual decline of acetylcholine and central cholinergic neurons with age, systemic stress and neurotransmitter disorders, as well as the decline of cortical function, resulting in abnormal brain function9. At the same time, as the body functions deteriorate, the ability of middle-aged and elderly patients to adapt to external stress decreases, especially for fracture trauma and surgical stimulation, which leads to a decrease in their ability to adapt to the surrounding environment, and they are more likely to be affected by psychological factors before surgery, which leads to nervousness, apprehension and fear, and makes them overly nervous, which, together with trauma or surgical stress, increases the risk of delirium. This study shows that the risk of postoperative delirium in patients aged ≥ 70 years old is much higher than that in patients aged < 70 years old.
Relationship between postoperative delirium and complications
Middle-aged and elderly patients are often complicated with a variety of medical diseases, such as "three highs"(high blood pressure, high blood sugar, high blood lipid), heart disease, lung disease, etc. This can easily lead to decreased stress ability and immunity of the body, water and electrolyte disorders, acid–base imbalance, and postoperative hypoxemia, leading to brain cell edema and brain dysfunction, which leads to POD. Previous studies have found that some preoperative underlying diseases such as hypertension and coronary heart disease are related to postoperative delirium, and the acute onset of chronic diseases is the most common precipitating factor. The more complications there are, the more precipitating factors there are, especially for patients with preoperative Alzheimer's disease and pulmonary diseases, the incidence of POD is higher10. Also, patients with more complicated internal diseases are more likely to suffer from electrolyte disorder and POD after surgery11. Related studies have confirmed that higher American Society of Anesthesiologists (ASA) scores is a high risk factor for postoperative delirium12, which explains why POD often occurs in elderly and weak adults, but rarely in young people.
Association of postoperative delirium with type of surgery and length of bed rest
Current studies have found that the incidence of POD in middle-aged and elderly patients after hip and spine surgery is significantly higher than that in other patients with simple extremity fractures13,14. A recent meta-analysis showed that hip surgery was significantly associated with the occurrence of POD in elderly patients after orthopedic surgery15. This may be related to the fact that patients still need to rest in bed for a long time after the operation of these parts. Meanwhile, a prospective study also confirmed that the occurrence of POD is closely related to the decrease of postoperative activity16. Zhu et al.17 also confirmed through a meta-analysis that POD after spinal surgery is associated with a significant reduction in early postoperative activities. Therefore, the above results can confirm that the incidence of POD in patients is significantly increased after major surgeries such as spine and hip surgery, and at the same time, a long time of bed rest after surgery is also easy to lead to the occurrence of POD in patients. This is similar to the results of our study.
Relationship between postoperative delirium and anesthetic methods
The pathophysiological mechanism of POD induced by anesthesia remains unclear. Previous studies have confirmed that it may be related to the dose of anesthetic drugs used during the operation, hemodynamic impairment and inflammatory response. At present, many scholars have explored the correlation between anesthesia methods and POD. Weber et al.18 showed that the cognitive function of patients after general anesthesia decreased more significantly than that after local anesthesia. Vasilevskis et al.19 showed that POD was highly likely to occur in middle-aged and elderly patients after general anesthesia. Some scholars have proved that local anesthesia can significantly reduce the occurrence of POD in the early postoperative period20. This may explain why POD is less common in patients with osteoporotic vertebral compression fractures after percutaneous vertebral augmentation. In this way, the occurrence of POD in early postoperative period also has a certain relationship with anesthesia methods. This study showed that the incidence of POD in patients with general anesthesia was significantly higher than that in patients with local anesthesia. Therefore, for middle-aged and elderly patients with fracture, we should mainly pay attention to the management of surgery and anesthesia. For the middle-aged and elderly patients, surgical methods with less trauma and short time should be selected as much as possible, and the normal physiological functions of the human body should not be disturbed as much as possible. At the same time, the anesthesia method should be as simple as possible, if necessary, electroencephalogram monitoring can be used in the operation to avoid too deep anesthesia. However, a recent multicenter randomized controlled study confirmed that there was no significant difference in the incidence, type and severity of postoperative delirium between local and general anesthesia in elderly patients with hip fracture21. Neuman m.d. et al.22 found through clinical research that the incidence of postoperative delirium in elderly patients with hip fractures under spinal anesthesia and general anesthesia was similar. These studies changed the traditional concept that "general anesthesia can cause brain dysfunction in elderly patients" and provided important guidance for clinical practice.
Relationship between postoperative delirium and hormone use
Glucocorticoids have anti-allergic, anti-inflammatory and other effects. Perioperative use of glucocorticoids in spinal surgery can reduce the stress response of patients and play a certain neuroprotective role. Therefore, after spinal surgery with neurological dysfunction, most doctors prefer to give patients a certain amount of glucocorticoids in the short term. A meta-analysis found that reducing the use of methylprednisolone in middle-aged and elderly patients after spinal surgery can reduce the incidence of POD23. Clemmesen et al.24 conducted a randomized controlled study on 117 elderly patients with hip fracture, found that preoperative intravenous injection of 125 mg methylprednisolone could significantly reduce the incidence of postoperative delirium, but did not reduce the severity of postoperative delirium. However, Royse et al.25 found that methylprednisolone could not reduce the incidence of POD through a randomized double-blind trial. At the same time, Sauër et al.26 found that the use of dexamethasone similarly failed to reduce the occurrence of POD. In the present study, we found that in some patients with burst spine fractures and hip fractures, the short-term use of methylprednisolone in small amounts (≤ 48 h) during the perioperative period had no significant effect on the occurrence of POD. Therefore, it is controversial whether there is an effect of hormonal use on POD occurrence.
Relationship between postoperative delirium and perioperative bleeding
At present, most studies have confirmed that intraoperative bleeding and postoperative hidden blood loss can significantly increase the incidence of POD. A recent meta-analysis showed that more blood loss during spinal surgery can be used to predict the occurrence of POD17. Nazemi et al.22 also confirmed that more blood loss during spinal surgery is more likely to lead to the occurrence of POD. Li et al.11 confirmed that high hidden blood loss during the perioperative period was an independent risk factor for the development of POD after internal fixation in middle-aged and elderly patients with intertrochanteric femoral fractures. This study showed that the incidence of POD in the operation with high perioperative blood loss such as spine and hip surgery was significantly higher than that in the operation with simple extremity fractures which could use tourniquet. This may be due to the increase of perioperative blood loss, leading to postoperative hypotension, interfering with the stability of blood circulation, affecting blood pressure and tissue perfusion and oxygen supply, contributing to tissue ischemia and hypoxia, and inducing POD.
Limitations
This study was a retrospective analysis, and the inclusion and exclusion criteria for patients with POD may be biased. In addition, this study was reported from a single medical clinical center, and the mechanisms and influencing factors regarding the occurrence of delirium after internal fixation of fractures in the middle-aged and elderly still need to be further explored in a multicenter, large sample size study.
Conclusions
In summary, advanced age, complex orthopedic surgery, more medical comorbidities, general anesthesia, greater perioperative blood loss may be independent risk factors for the development of POD after internal fixation of fractures in middle-aged and elderly patients. In middle-aged and elderly patients with fractures, less surgical trauma and more comprehensive perioperative management with guaranteed efficacy may significantly reduce the incidence of postoperative delirium.
Data availability
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- POD:
-
Postoperative delirium
- DSM-5:
-
American Psychiatric association's mental disorders and statistics manual
- CAM:
-
Ambiguous consciousness assessment method
- CI:
-
Confidence interval
- ASA:
-
American society of anesthesiologists
References
Inouye, S. K., Westendorp, R. G. & Saczynski, J. S. Delirium in elderly people reply. Lancet 383(9920), 2045 (2014).
Schenning, K. J. & Deiner, S. G. Postoperative delirium in the geriatric patient. Anesthesiol. Clin. 33(3), 505–516 (2015).
Liu, J. C. et al. Management of postoperative delirium in elderly patients. Chin. J. Geriatr. 39(10), 1130–1131 (2020).
Cai, L. et al. Research progress of postoperative delirium. Int. J. Anesthesiol. Resusc. 41(4), 411–416 (2020).
Dong, B. R. & Yu, P. L. Pay attention to the recognition and management of senile delirium. Chin. J. Geriatr. 39(10), 1113–1115 (2020).
Wen, X. P. et al. Research progress of postoperative delirium after hip fracture in the elderly. Chin. J. Geriatr. 39(10), 1219–1222 (2020).
Xiong, C. J. et al. Analysis of risk factors for postoperative delirium in elderly hip fracture patients. Chin. J. Bone Joint Injury 35(2), 162–164 (2020).
Li, T. et al. Design considerations of a randomized controlled trial of sedation level during hip fracture repair surgery: A strategy to reduce the incidence of postoperative delirium in elderly patients. Clin. Trials 14(3), 299–307 (2017).
Watne, L. O. The effect of a pre-and postoperative orthogeriatric service on cognitive function in patients with hip fracture: Randomized controlled trial (Oslo Orthogeriatric Trial). BMC Med. 12, 63 (2014).
Marcantonio, E. R. Delirium in hospitalized older adults. N. Engl. J. Med. 377(15), 1456–1466 (2017).
Li, K. P. et al. Analysis of risk factors of delirium after internal fixation in elderly with intertrochanteric femoral fractures after internal fixation. Chin. J. Trauma. Orthop. 22(3), 255–258 (2020).
Mosk, C. A. et al. Dementia and delirium, the outcomes in elderly hip fracture patients. Clin. Interv. Aging 12, 421–430 (2017).
Yang, L. & Li, Y. H. Research progress of postoperative delirium and cognitive dysfunction in the elderly. Chin. J. Gerontol. 39(6), 1508–1513 (2019).
Zhang, C. Q. & Jin, Q. K. Analysis of risk factors and nursing strategies of postoperative delirium in elderly hip fracture patients. Chin. General Med. 17(08), 1427–1429 (2019).
Yang, Y. et al. Incidence and associated factors of delirium after orthopedic surgery in elderly patients: A systematic review and meta-analysis. Aging Clin. Exp. Res. 33(6), 1493–1506 (2021).
Shi, Z. et al. Postoperative delirium is associated with long-term decline in activities of daily living. Anesthesiology 131(3), 492–500 (2019).
Zhu, C. et al. Risk factors for postoperative delirium after spinal surgery: A systematic review and meta-analysis. Aging Clin. Exp. Res. 32(8), 1417–1434 (2020).
Weber, C. F. et al. Impact of general versus local anesthesia on early postoperative cognitive dysfunction following carotid endarterectomy: Gala study subgroup analysis. World. J. Surg. 33(7), 1526–1532 (2009).
Vasilevskis, E. E. et al. Epidemiology and risk factors for delirium across hospital settings. Best. Pract. Res. Clin. Anaesthesiol. 26(3), 277–287 (2012).
Aldecoa, C. et al. European society of anaesthesiology evidence-based and consensus-based guideline on postoperative delirium. Eur. J. Anaesthesiol. 34(4), 192–214 (2017).
Li, T. et al. Effect of regional vs general anesthesia on incidence of postoperative delirium in older patients undergoing hip fracture surgery: The raga randomized trial. JAMA 327(1), 50–58 (2022).
Neuman, M. D. et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N. Engl. J. Med. 385(22), 2025–2035 (2021).
Nazemi, A. K. et al. Prevention and management of postoperative delirium in elderly patients following elective spinal surgery. Clin. Spine Surg. 30(3), 112–119 (2017).
Clemmesen, C. G. et al. Effect of a single pre-operative 125 mg dose of methylprednisolone on postoperative delirium in hip fracture patients; a randomised, double-blind, placebo-controlled trial. Anaesthesia 73(11), 1353–1360 (2018).
Royse, C. F. et al. Impact of methylprednisolone on postoperative quality of recovery and delirium in the steroids in cardiac surgery trial: A randomized, double-blind, placebo-controlled substudy. Anesthesiology 126(2), 223–233 (2017).
Sauer, A. M. et al. Intraoperative dexamethasone and delirium after cardiac surgery: A randomized clinical trial. Anesth. Analg. 119(5), 1046–1052 (2014).
Funding
National TCM Clinical Research Base Support Discipline Construction Plan (2020-JDXK-ZC01); Zhejiang Province "Thirteenth Five-Year Plan" Key Specialty Construction Project of Traditional Chinese Medicine (2019-01).
Author information
Authors and Affiliations
Contributions
L.Q.D. and X.P.Z. conceived and designed the study. Z.C.A., H.W. and L.G.W. collected the data. C.C. and Z.C.A. analyzed and interpreted the data. Z.C.A., L.G.X., and L.Q.D. wrote and translate the paper. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
An, Z., Xiao, L., Chen, C. et al. Analysis of risk factors for postoperative delirium in middle-aged and elderly fracture patients in the perioperative period. Sci Rep 13, 13019 (2023). https://doi.org/10.1038/s41598-023-40090-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-40090-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
