
Abstract
The purpose was to predict the risk of acute kidney injury (AKI) within 100 days after hematopoietic stem cell transplantation (HSCT) in patients with hematologic disease by using a new predictive nomogram. Collect clinical data of patients with hematologic disease undergoing HSCT in our hospital from August 2012 to March 2018. Parameters with non-zero coefficients were selected by the Least Absolute Selection Operator (LASSO). Then these parameters were selected to build a new predictive nomogram model. Receiver operating characteristic (ROC) curve, calibration curve, C-index, and decision curve analysis (DCA) were used for the validation of the evaluation model. Finally, the nomogram was further evaluated by internal verification. According to 2012 Kidney Disease Improving Global Guidelines (KDIGO) diagnostic criteria, among 144 patients, the occurrence of AKI within 100 days after HSCT The rate was 29.2% (42/144). The C-index of the nomogram was 0.842. The C-value calculated by the internal verification was 0.809. The AUC was 0.842, and The DCA range of the predicted nomogram was from 0.01 to 0.71. This article established a high-precision nomogram for the first time for predicting the risk of AKI within 100 days after HSCT in patients with hematologic diseases. The nomogram had good clinical validity and reliability. For clinicians, it was very important to prevent AKI after HSCT.
Similar content being viewed by others

Introduction
HSCT is the treatment of hematological malignant and benign diseases (such as leukemia, severe Mediterranean Anemia, etc.) effective measures1. AKI is one of the common complications after HSCT. The incidence of AKI after HSCT is 20% to 73% and the median time is 31 days. About 4.8% of patients require renal replacement therapy (RRT)2,3,4. As the severity of renal failure increases, the mortality rate of AKI patients also increases, accounting for more than 80% of patients requiring RRT5. The incidence of non-recurring deaths in AKI patients is high (HR 2.77, 95% CI 1.8–4.27)6. The study found that the cumulative mortality rate of the non-malignant disease AKI group within 100 days after HSCT was significantly higher than that of the non-AKI group (44.4% vs. 0%, p = 0.003)7. Therefore, it is of great significance to pay attention to the characteristics of patients with HSCT and establish a prediction of the risk of early AKI. The etiology and risk factors of AKI are complex. It is not only affected by the underlying diseases of transplant patients (such as chronic kidney disease, diabetes, hypertension, etc.), but also related to the medications used before and after transplantation, radiation, and transplant-related complications (such as conditioning toxicity, acute graft versus host disease (aGVHD), infection, hemorrhagic cystitis (HC), conditioning toxicity, etc.8.
This study aims to construct a nomogram model to predict the occurrence of AKI within 100 days after HSCT in patients with hematologic diseases. At present, the nomogram model is used to predict the survival period of moderate-risk acute myeloid leukemia, help identify patients with poor prognosis, and guide clinical treatment9, predict the risk of severe bleeding in patients with HLA-DQB1 mismatched HSCT10. And to predict the prognosis of multiple myeloma patients with pleural effusion11. This article reports for the first time a new predictive nomogram to predict the risk of AKI within 100 days after HSCT, which is of great significance for optimizing the management of patients after HSCT and preventing AKI.
Methods
Patients
This study was approved by the Ethics Committee of the First Affiliated Hospital of Guangxi Medical University. Collect clinical data of hematologic diseases patients receiving HSCT (August 2012 to March 2018) in our hospital. The criteria for the inclusion of patient data were as follows: (1) The diagnosis was clear and the data were complete; (2) Patients without renal dysfunction before HSCT (defined as glomerular filtration rate (eGFR) ≥ 60 ml/min/1.73 m2); (3) The patient received HSCT treatment for the first time. Exclusion criteria: (1) patients with unclear diagnosis and incomplete data; (2) patients with renal impairment before HSCT; (3) The patient received HSCT multiple times.
Data collection
This study collected clinical data of hematologic diseases patients who underwent HSCT, including gender, age, weight, basic creatinine level, stem cell source, donor source, human leukocyte antigen (HLA) and blood type matching, total body irradiation (TBI), cyclosporin A(CSA), Tacrolimus (FK506), vancomycin, amphotericin B, triazole antifungals, ganciclovir, aGVHD, HC, engraftment syndrome, secondary hypertension, secondary diabetes, infection. The patients were divided into two groups, the AKI group, and the non-AKI group. The criteria for infection were that the patient must had an axillary temperature above 37.7 °C for 1 h or an axillary temperature above 38.0 °C as previously reported12. In addition, we also referred to previous literature reports for the standard of aGVHD grade (Table 1)13,14. In this study, no patients were diagnosed with TMA. We used peripheral or bone marrow hematopoietic stem cells for patient transplantation.
R software (Vienna, Austria, https://www.R-project.org) was used for data analysis. The LASSO method was used for all clinical data analysis. Parameters with non-zero coefficients were selected to establish a predictive model. The nomogram was based on a score for each parameter, and the scores for each parameter were added together to obtain a total score. Each total score corresponded to the probability of an outcome event occurring. The discriminative ability and prediction accuracy of the nomogram were evaluated by C-index. The range of the C-index was usually < 0.5, 0.5–0.7, 0.7–0.9, and > 0.9, which represent low accuracy, medium accuracy, high accuracy, and extreme accuracy, respectively15. The calibration curve was used to evaluate the actual risk and predicted risk of the AKI nomogram. The predictive ability of the nomogram was evaluated by the AUC curve. The clinical net benefit was evaluated the DCA curve. Finally, we chose an internal verification method to verify the nomogram. The C-index was calculated through the bootstrapping verification of the AKI nomogram (1000 bootstraps resamples).
Ethics approval and consent to participate
All procedures were performed following relevant guidelines. This paper has been approved by the ethics committee of The First Affiliated Hospital of Guangxi Medical University. Written informed consent of patients has been obtained for this study.
Results
Patients’ characteristics
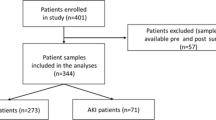
A total of 144 patients with hematological diseases who underwent HSCT were collected from August 2012 to March 2018 in our hospital, including 66 males and 78 females. Among all patients, 42 cases developed AKI and 102 cases without AKI. The data of the two groups were shown in Table 2, including the general data of the patients, transplant characteristics, drugs used, postoperative complications, and other information. In this study, a total of 42 patients with AKI were included for analysis, including 11 with stage I, 16 with stage II, and 15 with stage III renal impairment.
All data were analyzed by the LASSO regression analysis. A total of 7 parameters with non-zero coefficients were obtained. The binomial deviation (Fig. 1) and coefficient (Fig. 2) were obtained under the optimal lambda by LASSO analysis. A new nomogram was constructed to predict the risk of AKI within 100 days after HSCT (Fig. 3). The red dot for each parameter was specific information for that patient. The total score obtained for this patient was 227 points, and the predicted probability of AKI was 88.3% (Fig. 3).

The LASSO model was constructed to select the optimal parameters (lambda) and the relationship graph between binomial deviance and log (lambda) was drawn.

The features with nonzero coefficients were selected by optimal lambda.

The nomogram was constructed to predict the risk of AKI.
The C-index was measured to evaluate the predictive ability of the new nomogram, and the C-index was 0.842. The calibration curve was close to the ideal curve, indicating that the model had a good predictive ability (Fig. 4). The ROC curve was further constructed, and the AUC was calculated to be 0.842 (Fig. 5). The net benefit of the predictive nomogram ranged from 0.01 to 0.71, which was determined by DCA curve (Fig. 6).

Calibration curves for the nomogram of AKI.

Receiver operating characteristic curve of the prediction nomogram. The AUC of the nomogram scoring system for predicting AKI was 0.842.

The nomogram of the decision curve analysis and the net benefit of the model ranged from 0.01 to 0.71.
To further verify the actual predictive ability and stability of the nomogram. we chose an internal verification method. The C-index was analyzed by the bootstrap verification of the nomogram (1,000 bootstrap resampling). The C-index was 0.809, which was a very close C-index of 0.842 for the training set.
Discussion
AKI is a common complication after HSCT. The increased severity of AKI was associated with an increased risk of death7. The pathogenesis of AKI after HSCT was complicated and affected by many factors. Prerenal azotemia was a common cause of AKI in HSCT patients. Common adverse reactions to chemotherapy include nausea, vomiting, diarrhea, and mucositis, which often caused excessive fluid loss through the gastrointestinal tract or insufficient oral intake to cause circulation blood volume to be reduced, which eventually resulted in prerenal kidney injury16,17. In addition, acute tubular necrosis was also a common cause of AKI after HSCT. Hypovolemic shock, septic shock, or nephrotoxic drugs, such as amphotericin B, vancomycin and CSA could cause acute renal tubular necrosis and cause renal AKI, which could cause AKI alone or in synergy with prerenal etiology16,17,18. Urinary obstruction might be the cause of AKI in patients with HSCT. Intravenous infusion of ganciclovir and other antiviral drugs could precipitate in the urine and form crystals in the renal tubules, causing obstruction, and blood clots formed by HC could lead to urinary tract obstruction, resulting in obstructive postrenal AKI19. Although these complications might not be independent risk factors for AKI, their combination might lead to the occurrence of AKI. In addition, nephrotoxic drugs used to treat these complications could also cause AKI20.In addition, hypertension and diabetes also lead to the occurrence of AKI after HSCT3,18. Several risk factors for AKI in patients undergoing HSCT had been reported. The descriptions of transplant characteristics, such as donor, race, TBI, nephrotoxic agents, and post-transplant adverse events, such as aGVHD and infection, were inconsistently described as risk factors for the development of AKI21,22,23. Studies had shown that unrelated donors were closely associated with AKI (HR, 6.26; P = 0.042)20.It had been reported that transplantation of hematopoietic stem cells from unrelated donors was associated with a significant increase in the risk of infection, severe aGVHD, and organ toxicity24,25,26,27,28,29. Calcineurin inhibitor (CNIs) caused AKI by arteriolar vasoconstriction, reducing kidney perfusion, tubular toxicity, and endothelial injury30,31. CNIs nephrotoxicity after hematopoietic transplantation was reported in up to 31% of patients32. The infection could lead to hemodynamic changes and inflammatory damage, leading to AKI. The infection resulted in systemic arteriole constriction and endothelial damage, causing capillary leakage and renal insufficiency33. Damage to the tubules themselves led to the release of local cytokines and chemokines, resulting in local inflammation and further intrarerenal damage34. In addition, antimicrobials commonly used to treat infection were often nephrotoxic. However, the mechanism of AKI induced by triazole antifungals remained unclear35. Liu et al. found that HLA mismatched was closely related to AKI after HSCT (OR = 3.6; 95%CI = 1.1–13.0)36. And ABO mismatched was found to be associated with a significantly increased risk of grade II-IV aGVHD37. This might be the reason why ABO mismatched were associated with AKI.
AKI after HSCT could seriously affect the survival and prognosis of patients, so it was important to identify the risk of AKI in advance. At present, studies were using the hematopoietic cell transplantation-specific comorbidity index (HCT-CI) to study the incidence of AKI after allogeneic HSCT. HCT-CI factors included high disease risk, related donor, myeloablative conditioning regimen, stem cell source, prior stem cell transplant38. At present, this study was the first time to use the nomogram model to predict the risk of AKI within 100 days after HSCT.
In this paper, we introduced perioperative parameters to develop the nomogram of predicting AKI risk. The C-index was 0.842 and 0.809 in the training and validation set respectively, which revealed that the prediction ability of the nomogram was characterized by high accuracy15. The study showed that the higher the C-index of internal validation, the better the efficiency of identification and comparison15. In addition, we performed the decision curve analysis to estimate the actual clinical benefit of the nomogram. The results of DCA also showed high validity and predictive effect. The risk of AKI after HSCT could be predicted in advance by using the nomograph model, which could guide the management of HSCT patients, improve the survival of patients and improve the quality of life of patients. The results of this study showed that the factors included in predicting the risk of AKI after HSCT were donor, HLA, blood type matching, FK506, aGVHD, infection and triazole antifungal drugs.
However, this paper had some limitations. (1) This study was a retrospective analysis without a prospective study. (2) More cases need to be added to verify the nomogram.
Conclusion
In the article, the nomogram had good clinical validity and reliability. We found some factors that can be used to predict the risk of AKI within 100 days after HSCT, including donor source, HLA, blood type matching, FK506, aGVHD, infection, and triazole antifungal drugs. The nomogram can be used to predict the risk of AKI to optimize patient management during the diagnosis and treatment of HSCT.
Data availability
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
References
Xu, Z. L. et al. Haploidentical hematopoietic stem cell transplantation for paediatric high-risk T-cell acute lymphoblastic leukaemia. Pediatr. Transplant. 20(4), 572–580 (2016).
Kogon, A. & Hingorani, S. Acute kidney injury in hematopoietic cell transplantation. Semin. Nephrol. 30(6), 615–626 (2010).
Piñana, J. L. et al. Study of kidney function impairment after reduced-intensity conditioning allogeneic hematopoietic stem cell transplantation. A single-center experience. Biol. Blood Marrow Transplant. 15(1), 21–29 (2009).
Lopes, J. A. et al. Contemporary analysis of the influence of acute kidney injury after reduced intensity conditioning haematopoietic cell transplantation on long-term survival. Bone Marrow Transplant. 42(9), 619–626 (2008).
Parikh, C. R. & Coca, S. G. Acute renal failure in hematopoietic cell transplantation. Kidney Int. 69(3), 430–435 (2006).
Abramson, M. et al. Acute kidney injury in the modern era of allogeneic hematopoietic stem cell transplantation. Clin. J. Am. Soc. Nephrol. 16, 1318–1327 (2021).
Matsuoka, D. et al. Impact of acute kidney injury on overall survival in children and young adults undergoing allogeneic hematopoietic stem cell transplantation. Pediatr. Blood Cancer 68(9), e29167 (2021).
Kemmner, S., Verbeek, M. & Heemann, U. Renal dysfunction following bone marrow transplantation. J. Nephrol. 30(2), 201–209 (2017).
Hu, X. et al. A clinical prediction model identifies a subgroup with inferior survival within intermediate risk acute myeloid leukemia. J. Cancer 12(16), 4912–4923 (2021).
Qi, J. et al. HLA-DQB1 mismatch increase risk of severe bleeding independently in recipients of allogeneic stem cell transplant. Ann. Hematol. 100, 2351–2361 (2021).
Hou, Z. L. et al. Pleural effusion-based nomogram to predict outcomes in unselected patients with multiple myeloma: A large single center experience. Ann. Hematol. 100(7), 1789–1801 (2021).
Li, S. et al. Procalcitonin and C-reactive protein predict infection in hematopoietic stem cell transplantation patients. Leuk. Res. 105, 106574 (2021).
Glucksberg, H. et al. Clinical manifestations of graft-versus-host disease in human recipients of marrow from HL-A-matched sibling donors. Transplantation 18(4), 295–304 (1974).
Przepiorka, D. et al. 1994 consensus conference on acute GVHD grading. Bone Marrow Transplant. 15(6), 825–828 (1995).
Li, M. et al. Unilateral limited laminectomy for debridement to treat localized short-segment lumbosacral spinal tuberculosis: A retrospective case series. Orthop. Surg. 13(4), 1170–1180 (2021).
Cohen, E. P. Renal failure after bone-marrow transplantation. Lancet 357(9249), 6–7 (2001).
Noël, C. et al. Renal failure and bone marrow transplantation. Nephrol. Dial Transplant. 13(10), 2464–2466 (1998).
Kersting, S. et al. Acute renal failure after allogeneic myeloablative stem cell transplantation: Retrospective analysis of incidence, risk factors and survival. Bone Marrow Transplant. 39(6), 359–365 (2007).
Perazella, M. A. Crystal-induced acute renal failure. Am. J. Med. 106(4), 459–465 (1999).
Hirano, D. et al. Independent risk factors and long-term outcomes for acute kidney injury in pediatric patients undergoing hematopoietic stem cell transplantation: A retrospective cohort study. BMC Nephrol. 21(1), 373 (2020).
Kizilbash, S. J. et al. Acute kidney injury and the risk of mortality in children undergoing hematopoietic stem cell transplantation. Biol. Blood Marrow Transplant. 22(7), 1264–1270 (2016).
Didsbury, M. S., Mackie, F. E. & Kennedy, S. E. A systematic review of acute kidney injury in pediatric allogeneic hematopoietic stem cell recipients. Pediatr. Transplant. 19(5), 460–470 (2015).
Yu, Z. et al. Risk factors for acute kidney injury in patients undergoing allogeneic hematopoietic stem cell transplantation. Chin. J. Cancer 29(11), 946–951 (2010).
Li, J. M. et al. Separating graft-versus-leukemia from graft-versus-host disease in allogeneic hematopoietic stem cell transplantation. Immunotherapy 1(4), 599–621 (2009).
Laughlin, M. J. et al. Outcomes after transplantation of cord blood or bone marrow from unrelated donors in adults with leukemia. N. Engl. J. Med. 351(22), 2265–2275 (2004).
Shaw, P. J. et al. Outcomes of pediatric bone marrow transplantation for leukemia and myelodysplasia using matched sibling, mismatched related, or matched unrelated donors. Blood 116(19), 4007–4015 (2010).
Koh, K. N. et al. Favorable outcomes after allogeneic hematopoietic stem cell transplantation in children with high-risk or advanced acute myeloid leukemia. J. Pediatr. Hematol. Oncol. 33(4), 281–288 (2011).
Mogul, M. J. Unrelated cord blood transplantation vs matched unrelated donor bone marrow transplantation: The risks and benefits of each choice. Bone Marrow Transplant. 25(Suppl 2), S58-60 (2000).
Parody, R. et al. Severe infections after unrelated donor allogeneic hematopoietic stem cell transplantation in adults: Comparison of cord blood transplantation with peripheral blood and bone marrow transplantation. Biol. Blood Marrow Transplant. 12(7), 734–748 (2006).
Radermacher, J. et al. Pronounced renal vasoconstriction and systemic hypertension in renal transplant patients treated with cyclosporin A versus FK 506. Transpl. Int. 11(1), 3–10 (1998).
Oyen, O. et al. Calcineurin inhibitor-free immunosuppression in renal allograft recipients with thrombotic microangiopathy/hemolytic uremic syndrome. Am. J. Transplant. 6(2), 412–418 (2006).
Karimzadeh, I. et al. The pattern of cyclosporine nephrotoxicity and urinary kidney injury molecule 1 in allogenic hematopoietic stem cell transplant patients. Exp. Clin. Transplant. 19(6), 553–562 (2021).
Molema, G. et al. Renal microvascular endothelial cell responses in sepsis-induced acute kidney injury. Nat. Rev. Nephrol. 18, 95–112 (2022).
Schrier, R. W. & Wang, W. Acute renal failure and sepsis. N. Engl. J. Med. 351(2), 159–169 (2004).
Raghavan, R. & Shawar, S. Mechanisms of drug-induced interstitial nephritis. Adv. Chronic Kidney Dis. 24(2), 64–71 (2017).
Liu, H. et al. A multicenter, retrospective study of acute kidney injury in adult patients with nonmyeloablative hematopoietic SCT. Bone Marrow Transplant. 45(1), 153–158 (2010).
Ciurea, S. et al. The European Society for Blood and Marrow Transplantation (EBMT) consensus recommendations for donor selection in haploidentical hematopoietic cell transplantation. Bone Marrow Transplant. 55(1), 12–24 (2020).
Kagoya, Y. et al. Pretransplant predictors and posttransplant sequels of acute kidney injury after allogeneic stem cell transplantation. Biol. Blood Marrow Transplant. 17(3), 394–400 (2011).
Author information
Authors and Affiliations
Contributions
Z.G. and wrote the article and prepared Figs. 1, 2, 3, 4, 5, 6 and tables. Yongrong Lai, corresponding author, to whom correspondence should be addressed. Email:laiyongrong@hotmail.com. All authors reviewed the article. Z.G and L.C. contributed equally to this work and should be considered co-first authors. Patient provided consent for publication of the data and images.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gan, Z., Chen, L., Wu, M. et al. Predicting the risk of acute kidney injury after hematopoietic stem cell transplantation: development of a new predictive nomogram. Sci Rep 12, 15316 (2022). https://doi.org/10.1038/s41598-022-19059-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19059-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
