
Abstract
The present study investigates different scenarios to project the chance of achieving SDG 3.4 in Iran. In this study, the Iranian Death Registry System data was employed to estimate the Unconditional Probability of Dying (UPoD) for the four major categories of NCDs; then, the Bayesian model averaging was used to project the UPoD at the national and sub-national levels. Also, the prevalence of the risk factors was projected by 2030 based on STEPs as well as some other study data. Plus, UPoD and the possibility of achieving the target were estimated once again based on the assumption that the global reduction in risk factors proposed by WHO would be adopted in Iran. The UPoDs for the four NCDs in Iran were 17.5% (95% UI: 16.3–19.2) and 14.7% (13.3–16.2) in 2010 and 2015 respectively and if the current trend continues, 2030 will mark the UPoD of 10.8% (7.9–14.3). However, If the risk factors are reduced to the WHO target level by 2030, the UPoDs will be reduced to 5.44% (3.51–7.39) and 6.55% (5.00–8.13) of the 2010 and 2015 baseline scenarios, respectively, to enable some provinces to meet SDG 3.4. If the current trend continues, Iran will and will not achieve the SDG 3.4 in 2010 and 2015 baseline scenarios, respectively. However, if the global target set for reducing risk factors is achieved, Iran will meet all expectations in SDG 3.4 except in Asthma and COPD. Therefore, effective interventions are recommended to be designed and followed to reduce Asthma and COPD.
Similar content being viewed by others
Introduction
All countries in the world are committed to achieve Sustainable Development Goals (SDGs) introduced by the United Nations (UN) in September 20151. The forth target of the third SDGs (SDG 3.4) is focused on Non-Communicable Diseases (NCDs). This target is expected to make a one-third drop in the Unconditional Probability of Dying (UPoD) from NCDs in 30–70 year age group by 20301. World Health Organization (WHO) has, also, developed a global monitoring framework for NCDs along with a set of targets for modifiable risk factors to tackle the global epidemic of NCDs2. Bringing these measures into account is necessary to meet SDGs in many countries.
Iran, as a developing country, is experiencing epidemiological transition. These epidemiological changes have led to non-communicable diseases to become the greatest public health problem in the country3. This problem will give rise to years of life lost from premature deaths with great impact on life expectancy, and social, political and economic developments4. However, we do not possess accurate data on current and future trends of Unconditional Probability of Dying from NCDs at national and provincial levels to trace the progress of achieving SDG 3.4. Also, trends for UPoD may vary by variation of a single risk factor or joint effect of the risk factors. Therefore, to achieve the SDG 3.4, evidence based planning should be strictly carried out. Plus, avoidable number of deaths resulted from reduction of the risk factors, and its impact on UPoD should be modeled and estimated. Given the limited resources, realizing the priorities is imperative for the policy makers to design cost-effective interventions according to the existing resources.
The aim of this study is to project chance of Iran in achieving SDG 3.4 through the different scenarios. These scenarios are based on a reduction of the risk factors to the target levels set by WHO. So far, no study has been conducted on this issue in Iran and only few similar studies have been performed in the world. This paper, additionally, studies the degree to which SDG 3.4 will be achieved at national and sub-national levels by sex. The results can be employed for planning and evidence based policy-making at national and sub-national levels.
Methods
After addressing the incompleteness and misclassifications in the Iranian Death Registry System (DRS), it was employed to estimate the trends of UPoD for four major categories of NCDs (cancers, cardiovascular diseases, asthma and COPD, and diabetes). Bayesian Model Averaging (BMA) was used to calculate UPoD in the four major NCDs categories and the projection was conducted at the national and sub-national levels by 2030 to estimate the chance of achieving SDG 3.4. In parallel with this, using BMA and Spatio-Temporal models, the prevalence of six major risk factors (Diabetes, Hypertension, Overweight and Obesity, Physical Inactivity, Cigarette Smoking, Salt Intake) were projected by 2030. Avoidable deaths resulted from reducing NCDs risk factors were calculated using Population Attributable Fraction (PAF). UPoD was projected again after reducing avoidable deaths and then the extent of achieving SDG 3.4 at national and sub-national levels was studied in different scenarios. Also, gain in life expectancy after elimination of major NCDs causes of death was estimated by 2030. Study flow is shown in Figs. 1 and 2.

Study workflow in current situation.

Study workflow in WHO-based scenario.
Definitions
Unconditional probability of dying (UPOD): Unconditional probability of dying between ages 30 and 70 years (premature deaths) from NCDs.
2010 Baseline Scenario: One third decrease in the UPoD compared to 2010, if current trend continued.
2015 Baseline Scenario: One third decrease in the UPoD compared to 2015 if current trend continued.
2010 WHO based scenario: One third decrease in the UPoD if the risk factors decreased to the recommended level by WHO compared to 2010.
2015 WHO based scenarios: One third decrease in the UPoD if the risk factors decreased to the recommended level by WHO compared to 2015.
Data sources
Death data
We used the Iranian death registration system (DRS). Misclassification and incompleteness of DRS were addressed via Death Distribution Methods. This is discussed in more detail elsewhere5, 6. Moreover, redistribution method was adopted to correct the misclassifications in the causes of death and the inconsistency of the causes with age and sex. Also, the records of deaths included many cases of duplicated data that were corrected. Over the course of time, the administrative provincial division in Iran was changed which resulted in an increase in the number of the provinces. Thus, the data was restructured to include the new provinces7. To evaluate all-cause mortality rates, the age-spatio-temporal, Gaussian Process Regression (GPR), and Generalized Linear Mixed Models were employed. The method is described in more detail elsewhere5, 6.
Due to the modifications done in the registry code and data collection institution before and after 2001, the data before 2001 was not used. The DRS for that period of time (before 2001) did not encompass the cities of Tehran and Isfahan. Therefore, we used information from the cemeteries of Behest-e Zahra in Tehran and Bagh-e Rezvan in Isfahan to complete our datasets. Detailed description has been included elsewhere7.
Prevalence of the risk factors
The main sources for estimating the trend of prevalence of risk factors was STEPs Surveys carried out for seven rounds in Iran. These surveys were conducted in 2005, 2009, 2011 and 2016. STEPs Surveys included a large sample size to represent Iranian population. Plus, to estimate the prevalence of diabetes, hypertension and obesity, and overweight, some additional studies were employed that had been conducted in Iran (Table 1). The trend of mean of salt intake was obtained from STEPs 2016 and the other Iranian studies (Table1).
Relative risk (RR)
RRs were extracted from the Global Burden of Disease (GBD) and NCD.RisC (NCD risk factor collaboration)8,9,10,11. These RRs were derived for each risk factor-disease pair and then were categorized by age and sex.
Population data
The population data came from censuses carried out in 1996, 2006, 2011, and 2016, as well as the Iranian statistical yearbook divided by sex, age and province. Spectrum software (version 5.72) was employed to project population by 2030.
Covariate data
We used household expenditure and income survey to estimate the variables of the wealth index, years of schooling, and urbanization until 2015 sorted by age, sex, and province of residence12. Also, the spline method was used to estimate these covariates of wealth index, years of schooling, and urbanization until 2030. Then the results were entered into the covariate model.
Statistical analysis
Unconditional probability of dying
UPoD was calculated based on WHO guidelines from 2001 to 201513. Also, Bayesian Model Averaging (BMA) was used for its projection. According to this model, the ten covariates (six risk factors, wealth index, years of schooling, the percent of urbanization and population) produced 1024 different models (210 = 1024). BMAs in all of the models were integrated and with regard to the marginal likelihood of each model, they were weighted. In this model, prior distribution was assumed to be uniform. The number of burn-ins, and iterations were respectively retained to be 5000 and 20,000. Plus, selecting the baseline for comparison was optional. In this study, we considered 2010 and 2015 the two baselines to conduct comparisons and project SDG 3.4 achievement status (2010 and 2015 baseline scenarios).
Risk factors
The prevalence of diabetes, hypertension and obesity, and overweight was estimated with Gaussian Process Regression (GPR). more details are available elsewhere14, 15.The prevalence of physical inactivity and smoking was extrapolated from 2001 to 2005 and the missing points were interpolated in with spatiotemporal model. The data for two risk factors are also available in 2000. We do not possess any data for the year of 2001 to 2005. The trend of prevalence of risk factors was projected with BMA and spatiotemporal models (more details in supplementary appendix 1).
Population attributable fraction (PAF)
PAF was calculated for each pair of the risk factor-disease (supplementary appendix 2) in different scenarios (2010 and 2015 baselines) by sex and province. Risk factor scenarios are presented in Table 1. Joint effect of risk factors was calculated as well (Eq. 1). Mortality rate by 2030 was projected with spatio-temporal model by sex, cause and province.
Then the number of deaths from the multiplication of the death rate in the population was calculated. After subtracting the avoidable deaths from projected deaths, the UPoD was calculated again.
Cause deleted life table
The impact of reducing major NCDs related causes of deaths on increasing life expectancy was estimated by cause-deleted life table and the composition method.
Results
Current situation
According to the results of our study, if the existing trend continues based on the 2010 baseline, a one-third reduction in UPoD will be achieved by 2030 (however, if the trend is broken down to the categories of NCDs, the trends of CVDs and diabetes, as two separate trends, will be very close to reaching the target but won’t meet the expected levels). On the flip side, there will be no reduction of risk factors in 2015 baseline scenario. The values of UPoD from cancers in Iran were 4.2% (95% UI: 3.8–4.6) and 3.2% (2.9–3.6) in 2010 and 2015 respectively. This value is projected to be 2.2% (1.5–3.1) by 2030.
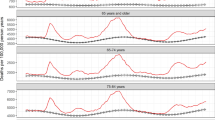
The corresponding values for 2010 baseline scenario, 2015 baseline scenario and the overall 2030 projected value for CVDs are 10.8% (9.8–12.0), 9.3% (8.3–10.3.), and 7.0% (5.1–9.3) respectively. The UPoDs from asthma and COPD in females were 1.7% (1.6–1.8) and 1.5% (1.4–1.6) in 2010 and 2015 respectively; and the overall asthma and COPD related UPoD is projected to drop to 1.0% (0.8–1.3) by 2030. The corresponding values for diabetes are 0.7% (0.6–0.7), 0.6% (0.5–0.6), and 0.4% (0.3–0.6) respectively. The trends and projections of UPoD in the 2001 to 2030 time-frame, are shown in Fig. 3a by categories. The trends and projections of UPoD for the years of 2001 to 2030 are indicated in Fig. 3 by sex and categories of NCDs.

Trends and projections of unconditional probability of dying in four categories of NCDs. (a) Females, (b) Males.
Prevalence of risk factors
Based on our projections, the age-standardized prevalence of diabetes, hypertension, obesity and overweight, and physical inactivity trend from 2015 to 2030 will increase in females by17%, 41, 32% and 29% respectively. The corresponding values in males will be 20%, 41%, 48% and 39%. The prevalence of smoking will be decreased by 27% in females and 28% in males in the same period. Also, mean of salt intake will be dropped by 12% and 16% in females and males, respectively.
The age-standardized prevalence and projection of diabetes, hypertension, obesity and overweight, physical inactivity, smoking, and mean of salt intake are shown in Table 2 in three time periods. The prevalence of risk factors at sub-national level are provided in supplementary appendix 3.
Avoidable deaths by 2030
According to the projected mortality rate and the prevalence of risk factors in 2030, avoidable deaths from the risk factors are categorized and estimated in three different scenarios. The number of avoidable deaths by sex, cause, and risk factor are shown in Table 3. The number of avoidable deaths at sub-national level is provided in supplementary appendix 4. The projected number of deaths in 2030 will be 47,847 among females and 64,784 among males in the 30–70 age group. The number of avoidable deaths from joint effects of risk factors in theoretical minimum exposure risk level (TMREL) will be 42,928 in females and 55,578 in males. The corresponding numbers in WHO-based scenarios will be 30,638 and 37,598 in females and males in 2010 baseline scenario. These same values in 2015 baseline scenario are calculated to be 24,853 and 29,566 in WHO-based scenario in females and males respectively.
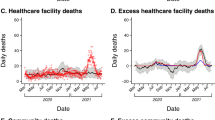
WHO-based scenario
If the risk factor targets determined by WHO are met, Iran will meet SDG 3.4 in both 2010 and 2015 baseline scenarios. Iran, at national level, will achieve the goal for each of the four NCD categories in 2010 baseline scenario (Fig. 4). However the country will not achieve a one-third reduction in asthma and COPD related UPoDs in 2015 baseline scenario (Fig. 5). By 2030, cancer, CVDs, asthma & COPD and diabetes related UPoDs will be respectively 1.59, 2.54, 1.07 and 0.22 in 2010 baseline scenario and 1.60, 3.55, 1.05, and 0.30 in 2015 baseline scenario. The rise in life expectancy is shown in Table 4.

Comparing the projected UPoD (if the current trend goes on) with the UPoD after reducing the avoidable deaths in 2010 WHO-based scenario.

Comparing the projected UPoD (if the current trend goes on) with the UPoD after reducing the avoidable deaths in 2015 WHO-based scenario.
Subnational
Current situation
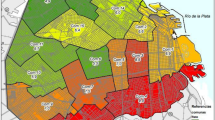
In 2010 baseline scenario, if the current trend prevails, 30 out of 31 provinces will meet SDG 3.4 among females in cancer by 2030. Also, by the same time-period, 21 provinces will achieve the targets in CVDs, asthma and COPD, and diabetes (Fig. 6a). Plus, 24, 22, 27, and 24 provinces will meet SDG 3.4 in cancer, CVDs, asthma and COPD, and diabetes among males respectively (Fig. 6b).

Achieving SDG 3.4 in current situation in the 2 scenarios. (a) Female in 2010 baseline scenario, (b) male in 2010 baseline scenario, (c) female in 2015 baseline scenario, (d) male in 2015 baseline scenario. The map was generated in R software version 4.0.1 (2020-04), https://cran.r-project.org/bin/windows/base/.
On the other hand, based on 2015 baseline scenario, by the year 2030, to total number of 21, 9, 16, and 18 provinces will reach the target in cancer, CVDs, asthma and COPD, and diabetes among females respectively (Fig. 6c). Moreover, 17, 9, 21, and 18 provinces will meet SDG 3.4 respectively in cancer, CVDs, asthma and COPD, and diabetes among males (Fig. 6d).
WHO-based scenarios
As indicated by the Joint effect of the risk factors in WHO based scenarios, all of the provinces in cancer and CVDs; 21 provinces in asthma and COPD, and 29 provinces in diabetes will achieve SDG 3.4 designed for females. The corresponding number of provinces are 27 and 30 for males (WHO-based scenario10). Also, 30 provinces will reach SDG 3.4 in cancer and CVDs in females; whereas, the number of the provinces meet SDG 3.4 in cancer and CVDs will be 26 and 30 in males respectively. Plus, 15 provinces in asthma and COPD, and 29 province in diabetes will achieve SDG 3.4 in females. On the other hand, 15 ad 29 provinces will reach SDG 3.4 in asthma and COPD and diabetes in males respectively (Fig. 7).

Achieving SDG 3.4 in WHO based scenario in the 2 scenarios. (a) Female in 2010 WHO based scenario, (b) male in 2010 WHO based scenario, (c) female in 2015 WHO based scenario, (d) male in 2015 WHO based scenario. The map was generated in R software version 4.0.1 (2020-04), https://cran.r-project.org/bin/windows/base/.
Discussion
The results showed that with continuation of the current trend (adjusted with the prevalence of risk factors), Iran will not achieve SDG 3.4; thus, in order to achieve a one-third drop in UPoD, some interventions should be conducted in 2015 baseline scenario. On the flip side, the country will be close to achieving the one-third reduction in UPoD (meeting SDG 3.4) in 2010 baseline scenario without any interventions. Obviously, SDG 3.4 wouldn’t be achieved by reducing just one single risk factor. In both 2010 and 2015 baseline scenarios, estimating the joint effect of risk factors could prevent 60.5 and 48% of the projected deaths by 2030, respectively. In 2010 baseline scenario, reducing avoidable deaths will result in achieving SDG 3.4 in Iran; whereas, in 2015 baseline scenario, the country will only achieve SDG 3.4 in cancer, cardiovascular disease, and diabetes; therefore, more efforts and serious interventions are needed in terms of asthma and COPD. It worth mentioning that there is considerable diversity among the provinces regarding the achievement of SDG 3.4.
Iran has been experiencing a downward trend in deaths from non-communicable diseases and this trend will be continued by 203016; however, this downward trend is not enough for achieving SDG 3.4. An international study showed that Iran will meet the target by 2030 in 2015 baseline scenario at national level17. The result of the aforementioned study is not consistent with those of our study. The reason behind this inconsistency may be the employed data. In our study, the total of 524,174 real data points were used for modeling. The data was divided by province, age, cause, sex in 15 years; whereas, the results from the other study17 were model driven.
Another study conducted in Mexico showed that, in 2010 baseline scenario, this country will not be able to achieve SDG 3.4 if the current situation prevails18. The mortality rate from non-communicable diseases in Mexico has declined to 22.9% which it not enough for the nation to achieve SDG 3.4. In our study, in 2010 baseline scenario, relative change of UPoD will be -39% in 2030. That is, the country will meet the target but the achievement will not be equally distributed in all the NCD categories and provinces. Also, Iran will experience a 27% decline in UPoD in 2015 baseline scenario.
Another study concluded that if the current trends in risk factors remain stable in China by 2030, 13.1% of premature deaths from NCDs will be decreased resulting in failure to achieve SDG 3.4. In the combined scenario, in which all the risk factor reduction targets are achieved, the mortality from cardiovascular and COPD will be reduced by one-third19. However, Iran will not meet the target in asthma and COPD category.
The present study was carried out using a huge bulk of integrated datasets, providing a projection for the risk factors (for the first time). Based on the current trend and given the targets set by the WHO for risk factors, the present study defined different scenarios and provided the benefits of intervention, or a series of interventions, in light of reducing in the number of deaths. The present study is one of the first few investigations conducted on the issue. It employs a comprehensive approach with modeling and projection to help policy-making and planning for NCDs.
The results of the study provide a brand new dashboard for decision making and optimal allocation of resources by policy makers in the health system. For projection of UPoD, several models were used; in order to employ all possible models and to avoid missing data, BMA was used for projection of UPoD. Another strength of the study is the use of valid RRs extracted from globally significant studies; as a result, the residual confounding was minimized. All analyses were performed by categorization of sex and province. Considering the vast spectrum of this study, there were some limitations; first, the alcohol consumption trend was not available in Iran and due to its low prevalence in 2016 STEPs data (supplement appendix 4), this risk factor was excluded from the study. We made an effort to confront data sacristy challenges with various modeling techniques including Sptio-temporal and GPR. Changes in provincial administrative divisions and increased number of provinces were addressed by Misalignment approach. Also, Alterations in definitions over the time were modified by Cross Walk method and lack of data on the prevalence of risk factors for the age group of 65–69 years in the STEPs before 2011 was addressed by Fractional Polynomial Models.
According to the projections performed in this study, Iran will face a critical situation in which people affected with multiple NCDs risk factors. Hypertension, physical inactivity, obesity, and diabetes are on the rise and despite the decreasing trend in mean of salt intake, this risk factor is, still, higher than the global standard. Therefore, there should be interventions designed and implemented at the individual, population and health system levels.
In this study, hypertension accounts for the highest number of avoidable deaths (this risk factor is prioritized at the interventions). According to the results of STEPs survey performed in 2016, 54% of people in 30–70 year age-group are aware of hypertension, of which 37% receive treatments. Hypertension in 37% of these individuals, is under control20. Therefore, the main measures for reducing the hypertension, would be boosting awareness and perusing effective coverage of the controlled hypertension. It is recommended to conduct national preparation program to identify and control hypertension and develop a set of self-care management strategies. Sensitization should be performed up to the extent that each person is aware of their own blood pressure number. Also, part of the hypertension related avoidable deaths is related to the high level of salt intake. Given that about 70% of the salt is sodium and it is added to the food outside the home21, it is suggested that intersectoral collaboration interventions for modification in the processes of production of food industry be conducted to reduce salt intake. At the population level, mass media can be employed to change the consumer behaviors; also, launching some strategic campaigns would reinforce the impact of mess media. At the individual level, the "table without shaker" campaign may be adopted as an effective intervention.
The second highest number of avoidable deaths (After hypertension) is associated with physical inactivity and obesity. To reduce avoidable deaths from physical inactivity, infrastructures should be provided at the macro level. Creating an appropriate and safe infrastructures to support hiking and cycling and providing social security to support individuals-especially women-to perform physical activity during their free time, is of significant importance. To increase public awareness and motivate the community to avoid physical inactivity, the mass media can be a game-changer in terms of the behavior at individual and group levels. Sports programs may be designed to be performed in places such as parks, streets, schools and the workplaces. An example of these programs is the ParticipACTION program proposed by the Canadian government to encourage the general population to increase physical activity and to achieve physical health. This program led to considerable reduction in health costs22. One of the benefits of a physically active population is the balance of energy and the prevention of obesity23. Given the challenges in the implementation of individual interventions to reduce obesity, the emphasis should be put on the population and intersectorial interventions. Apart from interventions designed for increasing physical activity level, it is suggested to educate public on nutrition and counsel them in different environments (such as schools, hospitals, and work environments, …), use food labels to reduce overall energy consumption, propose diet reform, and implement tax on sweet drinks and processed and Fast foods. Including consultation on non-communicable risk factors as part of the Primary Health Services (PHC) would, also, be a cost-effective measure.
Conclusions
Given the current trends, Iran is unlikely to achieve SDG 3.4. Therefore, it is recommended that the Ministry of Health, besides intersectorial collaboration with the other organizations, consider all life-style and pharmacological interventions at individual and population levels. Inter-sectorial health system interventions appears to produce clear path for public, health care community, policy makers, and insurance companies to achieve SDG 3.4 while there is still time to the end of SDGs deadline.
References
United Nations. Sustainable Development Goals 2015, https://www.un.org/sustainabledevelopment/sustainable-development-goals/.
World Health Organization. NCD Global Monitoring Framework (2011).
Institute for Health Metrics and Evalution. GBD Compare (IHME, University of Washington, 2015).
Abegunde, D. O., Mathers, C. D., Adam, T., Ortegon, M. & Strong, K. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet 370, 1929–1938 (2007).
Mohammadi, Y. et al. Levels and trends of child and adult mortality rates in the Islamic Republic of Iran, 1990–2013; protocol of the NASBOD study (2014).
Parsaeian, M. et al. Application of spatio-temporal model to estimate burden of diseases, injuries and risk factors in Iran 1990–2013 (study protocol). (2014).
Gohari, K., Rezaei, N. & Farshad Farzadfar, M. National and subnational patterns of cause of death in Iran 1990–2015: Applied methods. Arch. Iran. Med. 20, 2 (2017).
Kontis, V. et al. Contribution of six risk factors to achieving the 25 × 25 non-communicable disease mortality reduction target: A modelling study. Lancet 384, 427–437 (2014).
Gakidou, E. et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 390, 1345–1422 (2017).
Forouzanfar, M. H. et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1659–1724 (2016).
Kontis, V. et al. Regional contributions of six preventable risk factors to achieving the 25× 25 non-communicable disease mortality reduction target: A modelling study. Lancet Glob. Health 3, e746–e757 (2015).
Kasaeian, A. et al. Bayesian autoregressive multilevel modeling of burden of diseases, injuries and risk factors in Iran 1990–2013 (study protocol). (2014).
World Health Organization. Noncommunicable Diseases Global Monitoring Framework: Indicator Definitions and Specifications (2014).
Khosravi Shadmani, F. National and subnational levels achievement to Sustainable Development Goals (SDGs) for non-communicable diseases in Iran: modeling study with scenario-based projection (Kerman University of Medical Sciences, 2019).
Mehdipour, P. & Ghanbari, M. A. Package ‘GPRMortality’. (2018).
Khosravi Shadmani, F., Farzadfar, F., Larijani, B., Mirzaei, M. & Haghdoost, A. A. Trend and projection of mortality rate due to non-communicable diseases in Iran: A modeling study. PLoS ONE 14, e0211622 (2019).
Bennett, J. E. et al. NCD Countdown 2030: Worldwide trends in non-communicable disease mortality and progress towards Sustainable Development Goal target 3.4. Lancet 392, 1072–1088 (2018).
González-Pier, E. et al. Mexico’s path towards the Sustainable Development Goal for health: An assessment of the feasibility of reducing premature mortality by 40% by 2030. Lancet Glob. Health 4, e714–e725 (2016).
Li, Y. et al. Can China achieve a one-third reduction in premature mortality from non-communicable diseases by 2030?. BMC Med. 15, 132 (2017).
VISIT. Data Visualization System: Non-Communicable Diseases Research Center (2019).
Harnack, L. J. et al. Sources of sodium in US adults from 3 geographic regions. Circulation 135, 1775–1783 (2017).
Barnes, J. D. et al. Results from Canada’s 2016 ParticipACTION report card on physical activity for children and youth. J. Phys. Act. Health 13, S110–S116 (2016).
Committee on Accelerating Progress in Obesity Prevention. Accelerating Progress in Obesity Prevention: Solving the Weight of the Nation (National Academies Press, 2012).
Acknowledgements
This project has been granted by Kerman University of Medical Sciences. The authors would like to express their deep appreciation to Prof.Majid Ezzati, Dr.Vasilis Kontis and Non-Communicable Diseases Research Center (NCDRC) in Tehran University of Medical Sciences who contributed in conducting this study by providing useful data and valuable comments.
Funding
Kerman University of Medical Sciences (Iran).
Author information
Authors and Affiliations
Contributions
F.K.S., A.A.H., and F.F. designed the study. A.A.H., F.F., and B.L. supervised the study. F.K.S. and M.Y. processed the data. F.K.S., M.Y., and K.M., M.R.B., and did the statistical analysis. F.K.S., A.A.H., F.F., K.M., and M.R.B. interpreted the results. F.K.S., A.A.H., F.F., M.Y., K.M., M.R.B., and B.L. wrote the original draft. F.K.S., A.A.H., F.F., B.L. review and edit the final draft.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Haghdoost, A.A., Farzadfar, F., Yoosefi, M. et al. Iran to achieve the SDG 3.4 at national and sub-national levels. Sci Rep 12, 3705 (2022). https://doi.org/10.1038/s41598-022-07441-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-07441-8
This article is cited by
-
Policy analysis of nutrition stewardship for prevention and control of Non-communicable diseases in Iran
BMC Health Services Research (2023)
-
Social determinants of health inequity in Iran: a narrative review
Journal of Diabetes & Metabolic Disorders (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
