
Abstract
Dysphagia is common in neurological disease. However, our understanding of swallowing and its central nervous control is limited. Sensory information plays a vital role in the initiation of the swallowing reflex and is often reduced in stroke patients. We hypothesized that the sensitivity threshold of the anterior faucial pillar could be facilitated by either electrical stimulation (ES) or taste and smell information. The sensitivity threshold was measured by ES in the anterior faucial pillar region. The measurement was repeated 5 min after baseline. Thirty minutes after baseline, the participants underwent a test for taste and smell. Immediately after the test, the ES was repeated. Thirty healthy volunteers with a mean age of 27 ± 5.1 participated in the trial. Mean sensitivity threshold at baseline was 1.9 ± 0.59 mA. The values 5 min after baseline (1.74 ± 0.56 mA, p = 0.027) and 30 min after baseline (1.67 ± 0.58 mA, p = 0.011) were significantly lower compared to the baseline, but there was no difference between the latter (p = 0.321). After 5 min, a potentially facilitating effect was found on oral sensitivity by ES of the faucial pillar area. Thirty minutes later, this effect was still present.
Trial registration Clinicaltrials.gov, NCT03240965. Registered 7th August 2017—https://clinicaltrials.gov/ct2/show/NCT03240965.
Similar content being viewed by others

Introduction
Dysphagia is encountered in various diseases and clinical specialties, especially in neurological patients, and has gained in scientific importance recently. It is associated with increased mortality, morbidity, a longer hospital stay, and high treatment costs1,2,3. In the acute phase of stroke, up to 80% of patients are diagnosed with swallowing disorders4. The most serious consequence of dysphagia after stroke is aspiration pneumonia, being the most common cause of death in stroke patients5. Therefore, dysphagia determines the immediate prognosis and is of particular relevance to neurological patients due to the functional link to the central and peripheral nervous system.
Although research in the field of dysphagia is increasing, there are still large gaps in our understanding of swallowing and its central nervous control.
Scientific literature on sensory functions in normal and disordered swallowing is heterogeneous. It differs on the importance or unimportance in the swallowing process of various oropharyngeal regions such as mucosa of the tongue base, faucial pillars, valleculae, epiglottis, or laryngeal folds. The heterogeneity stems from various experiments on human subjects (healthy controls or patients) or animals (rats, lambs, etc.) and different methods for measurement of sensory function or mode of swallowing (voluntary vs. involuntary)6. The mode of swallowing in particular is thought to have a significant effect on the swallowing process due to the fact that voluntary swallowing appears to be entirely different from involuntary swallowing7,8,9,10.
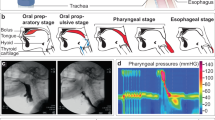
The hallmark of stroke-related dysphagia is loss of oropharyngeal sensitivity leading to uncontrolled leaking of the bolus from the oral cavity into the pharynx and a delayed triggering of the swallowing reflex, predisposing the patient to penetration of the bolus to the larynx and aspiration into the trachea without sufficient protective reflexes11,12,13,14.
Various approaches to assess oral sensory function already exist. Stimulation of oropharyngeal regions using air puffs, testing with Frey filaments, or simple bilateral testing using a cotton swab were described earlier15,16. An objective and quantifiable approach was first described by Power et al. using electrical stimulation (ES) of oral structures with an electrode mounted on a gloved finger17. Apart from the cotton swab, no method has been integrated into clinical routine.
To assess sensory function in a large cohort of stroke patients using the method described by Power et al., it was necessary to first generate data from healthy controls. The sensory threshold was examined in a specific region of the oral cavity, namely the anterior faucial pillar.
The faucial pillar region is of particular interest for our research, being the most distal area of the oropharyngeal tract that can be reached easily with the examiner’s index finger and without any side effects such as coughing or gagging. It is assumed that the faucial area plays a significant role in swallowing. Power et al. identified projections via the glossopharyngeal nerve from each faucial pillar to the sensory cortex of both hemispheres with ipsilateral predominance18. Data suggest that the contact of the bolus with the faucial pillar triggers the swallowing reflex19,20,21,22, although some authors found no evidence for this theory23,24. This theory stems from the observation that the elevation of the hyoid, which marks the time of pharyngeal swallowing, begins when the bolus makes contact with the faucial pillar region25,26.
ES of oral and pharyngeal regions has been implemented as a therapeutic approach to improve swallowing function. This is thought to activate neuroplasticity via sensory pathways27,28. Stimulation with a frequency of 5 Hz over 10 min over 3 days was found to have the largest effect29,30 on swallowing function.
We therefore hypothesized that the examination of oral structures via ES itself might facilitate the sensory function by lowering the sensory threshold, although we planned to use different parameters for stimulation (see below). A facilitating effect would be important for further trials, as this might change the results depending on the point of time or repetition of testing. To test our hypothesis, we repeated the examination of the bilateral sensory threshold in our participants to evaluate changes evoked by the stimulation itself.
As described in previous works, latency of swallowing reflex is reduced when olfactory and gustatory information is presented6,31,32,33. For this reason, the influence of taste or smell information on sensory function was investigated in our trial as well.
Results
Participants’ characteristics
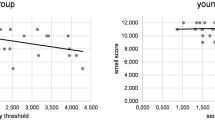
The median age in the group of volunteers was 27 ± 5.1, 16 persons (53.3%) were male, 2 (6.7%) were left-handed, and 5 (16.7%) reported cigarette smoking. The mean taste score was 11.83 ± 1.86, and the mean smell score was 11.13 ± 0.86.
Sensitivity threshold testing
In one person, we were unable to measure the sensitivity threshold of the left side, even when we increased the intensity to 100 mA.
A repeated-measures ANOVA showed a significant effect of time (F(1.839, 53.323) = 5.039; p = 0.012; Greenhouse–Geisser).
The sensitivity threshold was lower compared to baseline 5 min after the first measurement (1.9 ± 0.59 mA vs. 1.74 ± 0.56 mA; t(29) = 2.321; p = 0.027; Cohen’s d = 0.42; Bonferroni corrected p = 0.081). As this effect (although only significant by trend when corrected for multiple comparisons) could have been due to a training effect, we analysed the three values of the baseline measurement. The values for each individual side and the total of both sides showed high consistency (ICCleft = 0.75, ICCright = 0.66) and did not differ statistically (p > 0.05). This effect was also present after 30 min (1.9 ± 0.59 mA vs. 1.67 ± 0.58; t(29) = 2.721; p = 0.011; Cohen’s d = 0.49; Bonferroni corrected p = 0.033). The values 5 min after baseline and 30 min after baseline did not differ (1.74 ± 0.56 mA vs. 1.67 ± 0.58 mA; t(29) = 1.030; p = 0.321; Cohen’s d = 0.18; Bonferroni corrected p = 0.963). The results of the sensitivity measurements are depicted in Table 1 and Fig. 1.

Measurements of sensitivity threshold presented as mean and standard deviation. The values 5 min after baseline (1.74 ± 0.56 mA, p = 0.027, Bonferroni corrected p = 0.081) and 30 min after baseline (1.67 ± 0.58 mA; p = 0.011, Bonferroni corrected p = 0.033) are significantly lower compared to baseline, but there is no difference between 5 and 30 min after baseline (p = 0.321, Bonferroni corrected p = 0.963).
The order of smell and taste examinations had no impact on the 30-min value of the sensitivity threshold (smell first: 1.63 mA ± 0.64 vs. taste first: 1.7 mA ± 0.53; p = 0.728; t-test).
Discussion
Electrical threshold testing of the anterior faucial pillar is a simple, safe, and accurate diagnostic measure. By use of this method, we found a decrease over time in sensitivity threshold when the measurement was repeated 5 min and 30 min after baseline testing. A training effect seems unlikely, as the single values of the baseline measurement did not show this effect. The present data do not allow us to differentiate whether the lower sensitivity threshold 30 min after baseline is a prolonged facilitating effect of the ES or due to olfactory or gustatory information.
Stimulation of oropharyngeal structures with different modalities is used to improve the swallowing function of dysphagic patients. Olfactory information is thought to improve swallowing by activating the bilateral insular cortex, which is involved in central control of swallowing. Treating dysphagic patients with volatile black pepper oil improved their swallowing function31. Gustatory information is known to reduce the latency of the swallowing reflex. In particular, a sour bolus seems to have a large effect on the swallowing function6,32. Recently, the use of capsaicin has been evaluated for treating dysphagia. Capsaicin was found to increase substance P in the saliva. Substance P is a neuropeptide that enhances the swallowing and cough reflex34. Using capsaicin, Cabib et al. demonstrated a higher excitability of the motor cortex and enhancement of sensory conduction using transcranial magnetic stimulation35. Dysphagic patients showed an improvement in swallowing function when treated with capsaicin as compared to the placebo36. As olfactory and gustatory information has a positive impact on the swallowing function, it is conceivable that our test had an impact on the sensitivity threshold. With the present data, however, we are unable to distinguish between an effect of the ES or the taste and smell tests on the sensitivity threshold.
ES of oropharyngeal mucosa is an approved therapy for dysphagia following stroke. In theory, ES is thought to drive neuroplasticity by activating sensory fibres37. For pharyngeal electric stimulation (PES), an electrode mounted on a nasogastric tube is placed into the pharynx with contact to the posterior wall. The stimulation parameters with the largest effect were a stimulation at 5 Hz and a square wave duration of 200 µs with an individually adjusted stimulus intensity based on sensitivity threshold and maximum tolerated intensity29,38,39. PES was performed for 10 min on three consecutive days. Several smaller trials demonstrated a positive effect of PES on swallowing function30,39,40. However, a large multicentre trial failed to show this effect, which might be explained by the inclusion criteria and low stimulation intensity in the patients41. The same stimulation paradigm was used in a second multicentre trial in stroke patients tracheotomised due to dysphagia. This trial was terminated early because more patients receiving PES were ready for decannulation as compared to patients receiving sham stimulation42. ES of the faucial pillar region was also evaluated as a potential therapy method for dysphagia. Power et al. showed a facilitation of corticobulbar fibres using transcranial magnetic stimulation following a 10-min stimulation with a stimulus frequency of 0.2 Hz and a stimulus intensity of 75% of the maximum tolerated intensity17. When using this stimulation paradigm in dysphagic stroke patients, there was no effect on different swallowing parameters assessed by videofluoroscopy43. ES of the faucial pillar region has not been implemented into clinical routine. Our results might be explained by the effect of ES; however, our stimulation paradigm is different from the parameters that were used in prior experiments. Verifying our results in dysphagic patients regarding an improvement of swallowing function (using videofluoroscopy or flexible endoscopy of swallowing) would also be necessary to test for a clinical effect.
Thermal stimulation of oropharyngeal structures with ice (thermal-tactile stimulation = TTS) is a widely used approach in dysphagia therapy. This method is used to treat patients with an absent or delayed pharyngeal swallowing reflex. TTS is thought to improve the swallowing function by modulating the swallowing reflex. Alternatively, TTS may act as a heightened sensory input to central regions, facilitating a more rapid swallowing trigger44. An immediate effect of the swallowing function, such as increased speed of the swallowing trigger, has been described previously20,21. A review by Schwarz et al. did not show any evidence for a long-term effect on patients’ outcomes. The data on this matter must be interpreted carefully, as Schwarz et al. found large heterogeneity of the trials44.
As TTS and ES both include a mechanical component, the effect of mechanical stimulation has also been investigated. Sciortino et al. and Kaatzke-McDonald et al. found no effect of tactile stimulation on swallowing latency, using a probe to stroke the faucial pillar region45,46. As literature on the effect of pure tactile or mechanical stimulation in swallowing is sparse, the possibility remains that our results might at least partially be explained by the mechanical effect of the stimulation.
This study is limited by our inability to differentiate between an ongoing effect of the ES or an effect of the taste and smell tests, as described above. In case of an independent effect by smell or taste testing, it is not possible to determine which test is responsible for the effect. Repeating the test without sensoric testing or after a longer period (i.e., 24 h later) would help to further investigate the facilitating effect on the sensitivity threshold by ES. We are also unable to differentiate between an effect of the mechanical stimulation by the pressure of the finger-mounted electrode and the ES itself on the sensitivity. Further testing of patients in a clinical context is necessary to evaluate the clinical relevance of our findings. As we performed this experiment only in subjects below the age of 60, subjects with age 60 and above should be included, as dysphagia-related diseases (i.e., stroke or Parkinson’s disease) occur mainly in the elderly.
The facilitating effect must be kept in mind when sensitivity of the oral cavity is measured repeatedly in clinical trials. Measuring the sensitivity threshold in a standardized manner, as described below, offers the possibility of an objective and quantifiable measurement method for oral sensitivity. If the sensitivity threshold is assessed in the context of a clinical trial with dysphagic patients, we recommend measuring it first to circumvent a potential facilitating effect. In bedside screening, comprehensive examination of swallowing by a speech and language pathologist and endoscopic or videofluoroscopic evaluation of swallowing, the patient is usually given some amount of food and liquid. This might lead to a facilitating effect on the threshold, altering the results. By postponing the endoscopic evaluation of swallowing past ES and by conducting a standardized water-swallow test 4 h prior to ES, we estimate that the facilitating effect on sensitivity threshold will not occur and that the generated data might remain unbiased.
Methods
Participants
The study was conducted in a large German university hospital. The participants were healthy and below the age of 60.
The volunteers were included in the trial after providing written informed consent. The exclusion criteria comprised of a history of dysphagia (i.e., Parkinson’s disease, prior stroke, COPD, ENT tumours, dementia, etc.), known disturbances of smell and taste, known allergies to odorants or flavourings, or an implanted electrical device (i.e., cardiac pacemaker).
For the data acquisition and the use of findings for scientific analyses, an ethical approval was obtained from the local ethical committee (Justus-Liebig University, protocol number 149/16). All methods were carried out in accordance with relevant guidelines and regulations for involving human participants in the study. All participants gave informed consent.
The study was prospectively registered at www.clinicaltrials.gov (NCT03240965; registered 07/08/2017).
Sensitivity threshold
Sensitivity testing of the oral cavity was performed by measuring the sensitivity threshold of the faucial pillar, as described by Power et al.17. By this approach, we were able to acquire quantifiable and objectifiable measurements. A commercially available pudendal electrode (St Mark’s Pudendal Electrode, Natus Neurology Incorporated, Middleton, Wisconsin, USA) was used for stimulation. Delivering the stimulation to the wet mucosa of the oral cavity, does not pose much of a problem, as the pudendal electrode (designed for transvaginal or transrectal stimulation of the pudendal nerve) is designed for such an environment. The adhesive electrode was mounted on the finger, with the anode (diameter 6 mm) attached directly on the fingertip. The stimulation occurs directly underneath the anode. The anode was placed with moderate pressure on the medial part of the anterior faucial pillar in the lower third just above the height of the last molar tooth. The cathode (diameter 3 mm) had contact with the buccal mucosa. During stimulation, the position of the fingertip was visually controlled.
The pudendal electrode was connected to a common electroneurography device (Dantec Keypoint, Natus Neurology Incorporated, Middleton, Wisconsin, USA). The electric stimuli were delivered with the continuous stimulation setting at a frequency of 3 Hz with a square wave duration of 200 ms. We increased the stimulus intensity in 0.2 mA steps until the participant felt the stimulus. The measurement was repeated three times for each side in random order. We calculated the mean for each side, as well as the mean of both sides taken together.
Taste
To assess taste, we used a commercially available taste test kit (“Taste Strips”, Burghart Messtechnik, Wedel, Germany). This test was validated in a large study by Landis et al.47. A filter paper strip with a 2 cm2 tip area impregnated with different tastants (4 basic qualities in 4 different concentrations) was placed in the middle of the volunteer’s tongue. The taste strips featured the following concentrations: sweet: 0.4, 0.2, 0.1, 0.05 g/ml sucrose; sour: 0.3, 0.165, 0.09, 0.05 g/ml citric acid; salty: 0.25, 0.1, 0.04, 0.016 g/ml sodium chloride; and bitter: 0.006, 0.0024, 0.0009, 0.0004 g/ml quinine hydrochloride. A taste score was calculated from the number of correct answers.
Smell
Smell was tested with a commercially available screening test using 12 different felt-tip pens soaked with different odorants (“Sniffin Sticks,” Burghart Messtechnik, Wedel, Germany). Each odorant was presented to the middle of the participant’s nose. The test contained aromatic and trigeminal odorants. For each odorant, the participant had to choose the correct answer from a list of four different options. A smell score was calculated from the number of correct answers48.
Experimental procedure
Prior to testing, the participants fasted for at least one hour. The sensitivity was measured twice with a 5-min interval to test for facilitation of the threshold by the test procedure itself. Twenty-five minutes after the second measurement, we conducted the taste and smell tests to assess facilitation of the sensitivity threshold by those stimuli. The order of tests (smell first or taste first) was randomised. Afterwards, sensitivity was measured a third time. The workflow of the experiment is depicted in Fig. 2.

Workflow of the experiment.
Statistical analysis
Data are presented as mean and standard deviation. A repeated measures ANOVA was used to test for differences between the groups. For post-hoc tests, we used paired t-tests with correction for multiple comparisons (Bonferroni). For the remaining test, we used Student’s t-test. We also calculated Cohen’s d for the effect size. All statistical analyses were performed with SPSS, version 23.0 (©SPSS, Inc., IBM Company, 2015, Chicago, IL).
Ethics approval and consent to participate
For the data acquisition and the use of findings for scientific analyses, an ethical approval was obtained from the local ethical committee (Justus-Liebig University, protocol number 149/16). All methods were carried out in accordance with relevant guidelines and regulations for involving human participants in the study. All participants gave informed consent.
Data availability
The authors declare that the data supporting the findings of this study are available within the article.
Abbreviations
- ES:
-
Electrical stimulation
- PES:
-
Pharyngeal electrical stimulation
- TTS:
-
Thermal-tactile stimulation
References
Arnold, M. et al. Dysphagia in acute stroke: incidence, burden and impact on clinical outcome. PLoS ONE 11(2), e0148424. https://doi.org/10.1371/journal.pone.0148424 (2016).
Warnecke, T. et al. Fiberoptic endoscopic Dysphagia severity scale predicts outcome after acute stroke. Cerebrovasc. Dis. 28(3), 283–289. https://doi.org/10.1159/000228711 (2009).
Smithard, D. G., Smeeton, N. C. & Wolfe, C. D. A. Long-term outcome after stroke: does dysphagia matter?. Age Ageing 36(1), 90–94. https://doi.org/10.1093/ageing/afl149 (2007).
Martino, R. et al. Dysphagia after stroke: incidence, diagnosis, and pulmonary complications. Stroke 36(12), 2756–2763. https://doi.org/10.1161/01.STR.0000190056.76543.eb (2005).
Heuschmann, P. U. et al. Predictors of in-hospital mortality and attributable risks of death after ischemic stroke: the German Stroke Registers Study Group. Arch. Intern. Med. 164(16), 1761–1768 (2004).
Steele, C. M. & Miller, A. J. Sensory input pathways and mechanisms in swallowing: a review. Dysphagia 25(4), 323–333. https://doi.org/10.1007/s00455-010-9301-5 (2010).
Ertekin, C. Voluntary versus spontaneous swallowing in man. Dysphagia 26(2), 183–192. https://doi.org/10.1007/s00455-010-9319-8 (2011).
Costa, M. M. B. Neural control of swallowing. Arq. Gastroenterol. 55(Suppl), 61–75. https://doi.org/10.1590/S0004-2803.201800000-45 (2018).
Aida, S. et al. Peripheral and central control of swallowing initiation in healthy humans. Physiol. Behav. 151, 404–411. https://doi.org/10.1016/j.physbeh.2015.08.003 (2015).
Ertekin, C. et al. Voluntary and reflex influences on the initiation of swallowing reflex in man. Dysphagia 16(1), 40–47 (2001).
Aviv, J. E. Sensory discrimination in the larynx and hypopharynx. Otolaryngol. Head Neck. Surg. 116(3), 331–334 (1997).
Aviv, J. E. et al. Supraglottic and pharyngeal sensory abnormalities in stroke patients with dysphagia. Ann. Otol. Rhinol. Laryngol. 105(2), 92–97 (1996).
Dziewas, R. et al. Towards a basic endoscopic assessment of swallowing in acute stroke—development and evaluation of a simple dysphagia score. Cerebrovasc. Dis. 26(1), 41–47. https://doi.org/10.1159/000135652 (2008).
Sellars, C. et al. Swallowing abnormalities after acute stroke: a case control study. Dysphagia 14(4), 212–218 (1999).
Schimmel, M. et al. Oral tactile sensitivity and masticatory performance are impaired in stroke patients. J. Oral. Rehabil. 44(3), 163–171 (2017).
Theurer, J. A. et al. Effects of oropharyngeal air-pulse stimulation on swallowing in healthy older adults. Dysphagia 24(3), 302–313 (2009).
Power, M. et al. Changes in pharyngeal corticobulbar excitability and swallowing behavior after oral stimulation. Am. J. Physiol. 286(1), 45–50. https://doi.org/10.1152/ajpgi.00114.2003 (2004).
Power, M. L. et al. Deglutitive laryngeal closure in stroke patients. J. Neurol. Neurosurg. Psychiatry 78(2), 141–146 (2007).
Prosiegel, M. et al. Schluckstörungen bei neurologischen Patienten. Eine prospektive Studie zu Diagnostik, Störungsmustern, Therapie und Outcome. Nervenarzt 73(4), 364–370 (2002).
de Lama Lazzara, G., Lazarus, C. & Logemann, J. A. Impact of thermal stimulation on the triggering of the swallowing reflex. Dysphagia 1(2), 73–77 (1986).
Rosenbek, J. C. et al. Effects of thermal application on dysphagia after stroke. J. Speech Hear Res. 34(6), 1257–1268 (1991).
Rosenbek, J. C. et al. Thermal application reduces the duration of stage transition in dysphagia after stroke. Dysphagia 11(4), 225–233 (1996).
Ali, G. N. et al. Influence of cold stimulation on the normal pharyngeal swallow response. Dysphagia 11(1), 2–8 (1996).
Ali, G. N. et al. Influence of mucosal receptors on deglutitive regulation of pharyngeal and upper esophageal sphincter function. Am. J. Physiol. 267(4 Pt 1), G644–G649 (1994).
Veis, S. L. & Logemann, J. A. Swallowing disorders in persons with cerebrovascular accident. Arch. Phys. Med. Rehabil. 66(6), 372–375 (1985).
Robbins, J. et al. Oropharyngeal swallowing in normal adults of different ages. Gastroenterology 103(3), 823–829 (1992).
Suntrup, S. et al. Pharyngeal electrical stimulation can modulate swallowing in cortical processing and behaviour—magnetoencephalographic evidence. Neuroimage 104, 117–124. https://doi.org/10.1016/j.neuroimage.2014.10.016 (2014).
Hamdy, S. et al. Long-term reorganization of human motor cortex driven by short-term sensory stimulation. Nat. Neurosci. 1(1), 64–68 (1998).
Fraser, C. et al. Driving plasticity in human adult motor cortex is associated with improved motor function after brain injury. Neuron 34(5), 831–840 (2002).
Scutt, P. et al. pharyngeal electrical stimulation for treatment of poststroke dysphagia: individual patient data meta-analysis of randomised controlled trials. Stroke Res. Treat. 2015, 429053. https://doi.org/10.1155/2015/429053 (2015).
Ebihara, T. et al. A randomized trial of olfactory stimulation using black pepper oil in older people with swallowing dysfunction. J. Am. Geriatr. Soc. 54(9), 1401–1406 (2006).
Gatto, A. R. et al. Sour taste and cold temperature in the oral phase of swallowing in patients after stroke. Codas 25(2), 164–168 (2013).
Leopold, N. A. & Kagel, M. C. Dysphagia—ingestion or deglutition?: a proposed paradigm. Dysphagia 12(4), 202–206 (1997).
Suntrup-Krueger, S. et al. Effect of capsaicinoids on neurophysiological, biochemical, and mechanical parameters of swallowing function. Neurotherapeutics. https://doi.org/10.1007/s13311-020-00996-2 (2021).
Cabib, C. et al. Short-term neurophysiological effects of sensory pathway neurorehabilitation strategies on chronic poststroke oropharyngeal dysphagia. Neurogastroenterol. Motil. 32(9), e13887. https://doi.org/10.1111/nmo.13887 (2020).
Wang, Z. et al. Effects of capsaicin on swallowing function in stroke patients with dysphagia: a randomized controlled trial. J. Stroke Cerebrovasc. Dis. 28(6), 1744–1751. https://doi.org/10.1016/j.jstrokecerebrovasdis.2019.02.008 (2019).
Cheng, I., Sasegbon, A. & Hamdy, S. Effects of neurostimulation on poststroke dysphagia: a synthesis of current evidence from randomized controlled trials. Neuromodulation. https://doi.org/10.1111/ner.13327 (2020).
Jefferson, S. et al. Reversal of a virtual lesion in human pharyngeal motor cortex by high frequency contralesional brain stimulation. Gastroenterology 137(3), 841–849. https://doi.org/10.1053/j.gastro.2009.04.056 (2009) (849.e1).
Jayasekeran, V. et al. Adjunctive functional pharyngeal electrical stimulation reverses swallowing disability after brain lesions. Gastroenterology 138(5), 1737–1746. https://doi.org/10.1053/j.gastro.2010.01.052 (2010).
Vasant, D. H. et al. Pharyngeal electrical stimulation in dysphagia poststroke: a prospective, randomized single-blinded interventional study. Neurorehabil. Neural Rep. 30(9), 866–875. https://doi.org/10.1177/1545968316639129 (2016).
Bath, P. M. et al. Pharyngeal electrical stimulation for treatment of dysphagia in subacute stroke: a randomized controlled trial. Stroke 47(6), 1562–1570. https://doi.org/10.1161/STROKEAHA.115.012455 (2016).
Dziewas, R. et al. Pharyngeal electrical stimulation for early decannulation in tracheotomised patients with neurogenic dysphagia after stroke (PHAST-TRAC): a prospective, single-blinded, randomised trial. Lancet Neurol. 17(10), 849–859. https://doi.org/10.1016/S1474-4422(18)30255-2 (2018).
Power, M. L. et al. Evaluating oral stimulation as a treatment for dysphagia after stroke. Dysphagia 21(1), 49–55 (2006).
Schwarz, M. et al. Impact of thermo-tactile stimulation on the speed and efficiency of swallowing: a systematic review. Int. J. Lang. Commun. Disord. 53(4), 675–688. https://doi.org/10.1111/1460-6984.12384 (2018).
Sciortino, K. et al. Effects of mechanical, cold, gustatory, and combined stimulation to the human anterior faucial pillars. Dysphagia 18(1), 16–26 (2003).
Kaatzke-McDonald, M. N., Post, E. & Davis, P. J. The effects of cold, touch, and chemical stimulation of the anterior faucial pillar on human swallowing. Dysphagia 11(3), 198–206 (1996).
Landis, B. N. et al. “Taste Strips”—a rapid, lateralized, gustatory bedside identification test based on impregnated filter papers. J. Neurol. 256(2), 242–248 (2009).
Hummel, T. et al. ‘Sniffin’ sticks’: olfactory performance assessed by the combined testing of odor identification, odor discrimination and olfactory threshold. Chem. Senses 22(1), 39–52 (1997).
Acknowledgements
None.
Funding
Open Access funding enabled and organized by Projekt DEAL. The research project received no funding.
Author information
Authors and Affiliations
Contributions
T.B., M.P., S.H., T.G.: Conceptualisation; T.B., S.H., S.W., M.Y.: Methodology; T.B., M.Y., M.V., M.J.: Participant recruitment; L.P., M.T., M.Y., I.R.: Examinations performed; T.B., J.D., S.W., M.V.: Analysis of data and statistics; T.B., S.H., M.J.: Preparation of original draft; T.G., M.T.: Review and Editing; All authors: Review and editing; ICMJE criteria for authorship read and agree with manuscript results and conclusions.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Braun, T., Hamzic, S., Doerr, J.M. et al. Facilitation of oral sensitivity by electrical stimulation of the faucial pillars. Sci Rep 11, 10762 (2021). https://doi.org/10.1038/s41598-021-90262-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-90262-y
This article is cited by
-
Age-related changes in oral sensitivity, taste and smell
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
