
Abstract
Despite a significant improvement with enhanced recovery programmes (ERP), gastro-intestinal (GI) functions that are impaired after colorectal resection and postoperative ileus (POI) remain a significant issue. In the literature, there is little evidence of the distinction between the treatment assessed within or outside ERP. The purpose was to evaluate the efficiency of treatments to reduce POI and improve GI function recovery within ERP. A search was performed in PubMed and Scopus on 20 September 2019. The studies were included if they compared the effect of the administration of a treatment aiming to treat or prevent POI or improve the early functional outcomes of colorectal surgery within an ERP. The main outcome measures were the occurrence of postoperative ileus, time to first flatus and time to first bowel movement. Treatments that were assessed at least three times were included in a meta-analysis. Among the analysed studies, 28 met the eligibility criteria. Six of them focused on chewing-gum and were only randomized controlled trials (RCT) and 8 of them focused on Alvimopan but none of them were RCT. The other measures were assessed in less than 3 studies over RCTs (n = 11) or retrospective studies (n = 2). In the meta-analysis, chewing gum had no significant effect on the endpoints and Alvimopan allowed a significant reduction of the occurrence of POI. Chewing-gum was not effective on GI function recovery in ERP but Alvimopan and the other measures were not sufficiently studies to draw conclusion. Randomised controlled trials are needed.
Systematic review registration number CRD42020167339.
Similar content being viewed by others

Introduction
Postoperative ileus (POI) is the slowing or stopping of gastrointestinal (GI) functions after surgery. Enhanced recovery programmes (ERP) allows a reduction in the time until GI function recovery and a decrease of the incidence of POI1,2. However, it still remains a time-lapse of stop of the GI functions after surgery that can lead to an impairment going from increased length of stay or pneumonia to death3. Also, POI has been shown to be associated with anastomotic leakage4.
Many treatments or mean of prevention to reduce the occurrence of POI or to reduce the time to GI function recovery has been assessed and analysed through meta-analyses but the interpretation of such literature is difficult due to the lack of identification of the perioperative management within the different studies and meta-analyses whilst it can be a serious bias.
ERP first appeared in Scandinavia in the 2000s before being generalised and it is difficult to identify studies in which the patients have been treated using ERP, a conventional treatment or both. It is important to know this because it can influence the results and some items that work with conventional treatment do not work with ERP. For example, it has been shown that chewing gum was efficient in the conventional management literature5, but not in ERP6. To date, there is no systematic review that draws a picture of the therapeutics or prophylactics that have been assessed in literature within ERP. Such a review could help physicians in the management of their patients, in improving and simplifying ERP, and such a review could help researchers to have a better cartography of “what works, what does not work and what has been assessed”.
The main aim of this study is to provide a systematic review of literature to draw a picture of the different means that were used to prevent or to treat POI and to improve GI function recovery. The second aim of this study is to provide a meta-analysis and a network meta-analysis of all the previously described means of treatment or prevention in order to offer the strongest proof of the efficiency, or lack thereof, of such means.
Methods
The study was registered at PROSPERO (registration number CRD42020167339) and it was reported according to PRISMA guidelines.
The inclusion criteria were: studies comparing at least two treatments that are not a part of the ERP that could improve the time to the first flatus or the first bowel movement, or reduce the occurrence of POI after colorectal surgery during the ERP. Studies were excluded if they were reviews or meta-analyses, case reports, letters, study protocols, on children, on animals or in a language other than French or English. Studies were also excluded if the material and methods did not specify if the setting was an ERP or not, or if such section specified that the setting was not an ERP. Studies were not included in the meta-analysis if the intervention was a feature used in the ERP (such as multimodal analysis, early feeding…).
The first outcome measure was POI occurrence. The definition of POI was recorded for all the studies included in the meta-analysis. POI could be the first outcome measure or the secondary outcome measure as well as it was reported in the study.
Secondary outcome measures were the time to first flatus and the time to first bowel movement.
A systematic search of the PubMed and Scopus databases was performed until 20 September 2019. The search algorithm in PubMed was as follow: ("2000/01/01"[Date–Publication]: "3000"[Date–Publication]) AND (("colon"[Title/Abstract]) OR ("rectal"[Title/Abstract]) OR ("colorectal"[Title/Abstract])) AND (("surgery"[Title/Abstract]) OR ("postoperative"[Title/Abstract])) AND (("ileus"[Title/Abstract]) OR ("motility"[Title/Abstract])) (Table 1).
All the titles and abstracts were extracted into an Excel sheet. Duplicates were removed. The titles and abstracts were reviewed by the authors to identify those that met the inclusion criteria. Full text screening was conducted by two authors independently. The data extraction was also conducted by two independent authors.
When the time to first flatus or bowel movement was reported as a median and interquartile range (IQR) or as a mean and standard error of the mean (SEM) in the original articles, these values were transformed as mean and standard deviation by assuming a normal distribution, so as to allow them to be included in the network meta-analysis.
Risk of bias were assessed by two authors, using the ROB-2 tool when studying randomised controlled trials (RCTs) and the ROBINS-I tool when studying non-randomized studies. Consensus was performed with a third author, if necessary.
Meta-analysis
We conducted meta-analyses based on random-effects models using the Knapp-Hartung method and the Sidik-Jonkman estimator7,8,9. Direct and indirect evidence for all studied treatments were combined to evaluate their associations with the studied outcomes. Results were then presented as odds ratios when studying dichotomous endpoints like ileus, and as standardised mean difference when studying continuous endpoints like time to first flatus or bowel movement.
These pairwise meta-analyses were only conducted if at least three studies assessed the same process.
Statistical heterogeneity was quantified with the I2 and τ2 statistics and tested using the Q-test of heterogeneity. When a significant heterogeneity was highlighted, meta-analyses were carried out again, excluding outlier studies, to evaluate the consistency of the meta-analysis results. Publication bias was assessed by the Egger regression asymmetry test.
All analyses were done using R software with the Meta, Netmeta and Dmetar packages (R software, 3.6.3, https://www.R-project.org/). All the statistical tests were bilateral considering a p-value threshold set at 0.05.
Results
Literature search
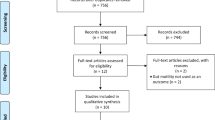
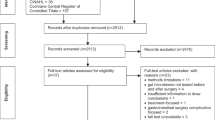
We identified 4442 articles after removing the duplicates, 4275 were excluded by screening the abstract because they did not meet the inclusion criteria and 167 full texts were analysed in their whole form (Fig. 1). Among these articles, 115 were excluded because the manuscript was not available or because the study did not take place within an ERP. Of the 52 remaining articles on studies, 24 concerned the ERP: analgesia or anaesthesia management for 17 studies10,11,12,13,14,15,16,17,18,19,20,21,22,23, exercise therapy for 124, type of anastomosis for 225,26, diet for 427,28,29,30 and the need for carbohydrate-rich beverages for 131. As these studies were concerned with different elements of ERP and not with specific supplementary treatments for GI function recovery, they were not included in the meta-analysis.

PRISMA flow chart.
Narrative synthesis
The other 28 processes are treatments or prophylaxis for POI or treatments to improve GI function recovery, such as alvimopan (n = 8)32,33,34,35,36,37,38,39, chewing gum (n = 6)40,41,42,43,44,45, coffee intake (n = 3)46,47,48, the use of prokinetic drugs (n = 5) such as ghrelin49,50, magnesium51, prucalopride 52, simethicone syrup 53; the use of non-steroidal anti-inflammatory drugs (NSAIDs) (n = 2)54,55, the use of furosemide (n = 1)56, the use of simvastatin (n = 1)57, the use of Gastrografin (n = 1)58 and the use of transcutaneous tibial nerve stimulation (TTNS) (n = 1)59. Of these, 18 were randomised controlled trials. The design of the studies is reported in Table 2.
Only one study assessed a curative treatment for POI. Indeed, in one RCT including 29 patients, the authors assessed the reduction of the time to resolve POI for patients receiving gastrografin as compared to a placebo58. No significant difference was shown between the placebo group (10.3 days (CI95% 6.96–10.29) and the Gastrografin group (9.1 CI95% 6.51–11.68) (p = 0.878).
The other 27 studies assessed treatment to reduce the time to GI function recovery to prevent POI (Table 3).
The Alvimopan was the most studied preventive treatment of POI but it was only assessed through non RCT studies35,37,39,40,41. Those studies exclusively compared the rate of POI and 4 of them showed a significant reduction of the rate of POI in the patients taking Alvimopan (2–10.8%) as compared to the patients not taking Alvimopan (12–20%)32,33,35,36. Ludwig et al.34 assessed the efficiency of Alvimpan to reduce the time to GI2 recovery. They showed a non-significant difference (21% vs 34%).
The chewing gum has been assessed in 6 RCTs42,43,44,45,46,47. Three of those compared the rate of POI but none reported significant difference between chewing gum (7.4–10%) and the control group (6.6–17%)42,43,45. Finally, only 1 of those 6 studies reported a significant reduction of the time to first flatus40 and 2 of those studies reported a significant reduction of the time to first bowel motion40,42. The study from Yang et al.41 compared 3 arms of treatments (control, chewing-gum, simo-decoction + acupuncture). They reported a higher improvement of GI function by using simo decoction + acupuncture as compared to chewing-gum or as compared to the control group.
Three studies assessed the coffee to reduce the time to first flatus or first bowel motion. Two of them compared the coffee to hot water46,48 and one of them to tea47. The control group being different, no meta-analysis was performed. All those studies showed a reduction of the time to first bowel motion46,47,48 and only one showed a reduction of the time to first flatus48. This last study also interested in decaffeinated coffee. This coffee without caffeine reduced the time to first flatus and first bowel motion as compared to the control group and to coffee with caffeine.
The intake of furosemide significantly increased the time to first bowel motion in one RCT56 while NSAIDs significantly reduced the time to first bowel motion in one retrospective study54 and significantly reduced the rate of POI in one retrospective study55.
The prucalopride and the ghrelin showed a significant of the time to first flatus in 3 RCTs49,50,52. Finally, in per-protocol analysis, TTNS significantly reduced the rate of POI in one RCT59.
Risk of bias
Several studies were identified as presenting serious risks of biases, considering both randomized and non-randomized studies. Two factors explained the vast majority of them: the missing data management and the lack of identification of a single primary objective (Table 4, Fig. 2). The outcome assessment blinding process was not informed in many studies. Many studies did not mention the missing data rate. For those mentioning such a missing data rate, five studies presented a lost-to-follow-up rate greater than 10%. Two studies reported commercial funding for the study even if the data analysis was reported to be independent.

(A) Bias assessement bias assesment tool for RCT's (ROB-2) and (B) bias assesment tool for non randomized studies (ROBINS'I).
Meta-analysis
Alvimopan
Among the eight studies focusing on alvimopan, seven assessed its impact on POI and none assessed the impact on time to first flatus or to first bowel movement (Table 1). The pairwise meta-analysis highlighted a significant reduction of POI occurrence (OR = 0.41; CI95% 0.20–0.81) (Fig. 3A).

Meta-analysis of the risk of POI according to a treatment by (A) alvimopan and (B) chewing gum; (R software, 3.6.3, https://www.R-project.org/).
Chewing gum
Six RCTs studied the impact of chewing-gum on POI40,41,42,43,44. These six studies included both first flatus and first bowel movement as outcome measures. Only three included POI as an outcome measure (Table 1).
No significant effect of chewing gum was highlighted concerning the POI occurrence, the time to first flatus, nor the time to first bowel movement (respectively OR = 0.89; CI95% 0.26–3.07, SMD = − 0.07; CI95% − 0.19;0.06 and SMD = − 0.24; CI95% − 0.50–0.01) (Fig. 3B).
Significant heterogeneity was observed concerning studies focusing on the relationship between chewing gum and time to first flatus (Fig. 4A) or to first bowel movement (Fig. 5A). When excluding the outlier studies from these meta analyses, the effect of chewing gum on both time to first flatus and time to first bowel movement interestingly became closely significant (respectively SMD = − 0.07; 95%CI − 0.19:0.06 and SMD = − 0.24; 95%CI − 0.5;0.01) (Figs. 4B and 5B).

Meta-analysis of the time to first flatus according to a treatment by chewing gum (A) with and (B) without the outlier; (R software, 3.6.3, https://www.R-project.org/).

Meta-analysis of the time to first bowel movement according to a treatment by chewing gum (A) with and (B) without the outlier (R software, 3.6.3, https://www.R-project.org/).
Discussion
Among the analysed studies, 28 were concerned with the effect of different measures on preventing POI or reducing GI function recovery. 12 drugs were assessed but only two were assessed at least three times. The Alvimopan was the most studied preventive treatment of POI through non RCT studies. Four of them showed a significant reduction of the rate of POI in the patients taking Alvimopan. The chewing gum has been assessed in 6 RCTs. None of them reported a significant improvement in the chewing-gum group, one reported a significant reduction of the time to first flatus and 2 reported a significant reduction of the time to first bowel motion. Also, 3 studies assessed the coffee and showed a reduction of the time to first bowel motion and only one showed a reduction of the time to first flatus.
In the meta-analysis including six RCTs, chewing gum had no significant effect on the endpoint but was close to reducing the time to first flatus and first bowel movement. In the meta-analysis including seven non-RCTs, alvimopan allowed a significant reduction of the occurrence of POI.
Interestingly, many studies assessed the impact of chewing gum on GI functions before the ERP. These studies largely showed a significant reduction of the time to GI function recovery or of the occurrence of POI5,60,61,62,63,64. Some authors support the opinion that chewing gum is not cost effective in the ERP because patients are allowed to drink and eat at an early stage, leading to a natural vagal stimulation that reduces the duration of GI function impairment64. However, all these studies assessed chewing gum with a view to preventing POI or reducing GI function recovery, but none assessed the utility of sham feeding in patients already presenting nausea or vomiting or requiring a nasogastric tube. This may be a new way for using chewing gum, not as a prevention but as a treatment for POI. This may improve postoperative care when we know that early feeding tolerance has been shown to be a predictive factor of the outcomes of colorectal surgery.
Then, alvimopan showed considerable utility by reducing POI. Many meta-analyses performed using studies that took place during, or outside, the ERP showed a reduction of the occurrence of POI by using such a drug65,66. The fact that alvimopan was efficient on POI even within ERP is surprising because it inhibits the peripheric opioid receptors while, theoretically, the patients should not receive high doses of morphine in ERP67. This result should therefore be considered with caution because the studies included in the meta-analysis were not RCTs and had some bias, such as the POI definition that was different between the studies. Therefore, the effect of alvimopan could be overestimated. Despite these encouraging results, a well-designed RCT is probably needed to confirm this result.
Coffee was assessed in three RCTs and showed a significant effect on the reduction of the duration of GI function impairment. This is interesting while it was shown that it also reduced these outcomes outside the ERP68. The caffeine was supposed to reduce inflammation in the bowel by stimulating the vagal pathway69.
The narrative review showed a potentially beneficial effect of NSAIDs on the first bowel movement. This is possible because it could be explained by the physiopathology of the POI, and the involvement of the inflammation in the installation of such pathology70,71. This must, however, be confirmed with RCTs to improve the quality of proof.
Also, the intake of tea or ghrelin and acupuncture possibly improved the time to first flatus. Again, this could be explained by the physiopathology for the ghrelin. Indeed, ghrelin stimulates GI motility and contributes to energy homeostasis72. We have no explanation for why tea or acupuncture could improve GI function recovery, but the level of proof is very low in this case (only one study for each modality of treatment, with three arms for each study).
Despite these encouraging results, two major difficulties in the analysis of POI within ERP have to be raised. First of all, the definition of POI was significantly different between the studies or was not reported in the material and methods section. This lack of consensual definition has already been raised in literature in 2005 by Kelhet et al.73 and still existed in 2017 despite multiple effort from physician to better understand and define POI74. This lack of consensual definition is a common limitation in all the review on POI management or prevention. Unfortunately, the study of bowel function recovery cannot supply to the lack of definition of POI because the outcome measures for bowel function recovery is not much consensual and vary between studies75, leading to discrepancy between studies. A study is now in progress to improve this issue but the results are not yet available76.
The second issue is due to the heterogeneity of ERP between the different teams and countries. Some of the studies did not describe the ERP while the others reported different items. This bias has been raised in 201577 and is still an issue in current literature. Indeed, to improve the quality of studies reporting ERP management, the ERAS Society proposed a checklist containing 20 items to better assess ERP compliance78. This will probably homogenize the studies on the influence of ERP on diverse pathology such as POI. In this meta-analysis, only studies reporting the patients followed an ERP were included in order to homogenize the perioperative management of the patient and to specifically focus on the treatment assessed.
Finally, the treatment that seemed to be more efficient was only assessed in non-RCTs. This could represent a bias of recruitment, but also in the reproducibility of the study because the definition was different between the studies and could be different within a single study.
These limitations preclude a reliable metaanalysis. Unfortunately, until there is no consensual definition of POI and until the ERP is not consensually reported, it will be difficult to bring stronger conclusion on all those elements used in addition ERP. This narrative review and meta-analysis brings some evidence on the efficiency of such elements. The aim of this meta-analysis was therefore achieved because (i) it raised the difficulties on assessing the treatments of POI within ERP and (ii) it structured the different modalities of treatment. Further RCTs are therefore needed to confirm whether there are beneficial effects of such treatment.
Conclusion
This meta-analysis revealed that, in ERP, the improvement of GI function recovery by measures, and especially the POI, is poorly studied in literature, with high discrepancy on definitions of POI and ERP. No strong conclusions can be drawn, except that chewing gum and coffee had no beneficial effect on these endpoints. Alvimopan reduced the occurrence of POI but further RCTs are needed to confirm this effect.
References
Barbieux, J. et al. Does enhanced recovery reduce postoperative ileus after colorectal surgery?. J. Visc. Surg. 154, 79–85 (2017).
Grass, F. et al. Postoperative ileus in an enhanced recovery pathway—A retrospective cohort study. Int. J. Colorectal. Dis. 32, 675–681 (2017).
Venara, A. et al. Proposal of a new classification of postoperative ileus based on its clinical impact-results of a global survey and preliminary evaluation in colorectal surgery. Int. J. Colorectal. Dis. 32, 797–803 (2017).
Venara, A. et al. Postoperative ileus concealing intra-abdominal complications in enhanced recovery programs—a retrospective analysis of the GRACE database. Int. J. Colorectal. Dis. 34, 71–83 (2019).
Liu, Q., Jiang, H., Xu, D. & Jin, J. Effect of gum chewing on ameliorating ileus following colorectal surgery: A meta-analysis of 18 randomized controlled trials. Int. J. Surg. 47, 107–115 (2017).
de Leede, E. M. et al. Multicentre randomized clinical trial of the effect of chewing gum after abdominal surgery. Br. J. Surg. 105, 820–828 (2018).
Sidik, K. & Jonkmann, J. K. A simple confidence interval for meta-analysis. Stat. Med. 21, 3153–3159 (2002).
Hartung, J. & Knapp, G. On tests of the overall treatment effect in meta-analysis with normally distributed responses. Stat. Med. 20, 177–182 (2001).
Hartung, J. & Knapp, G. A refined method for the meta-analysis of controlled clinical trials with binary outcome. Stat. Med. 20, 3875–3889 (2001).
Mujukian, A. et al. A standardized multimodal analgesia protocol reduces perioperative opioid use in minimally invasive colorectal surgery. J. Gastrointest. Surg. 24,2286-2294(2020).
Brandstrup, B. et al. Which goal for fluid therapy during colorectal surgery is followed by the best outcome: Near-maximal stroke volume or zero fluid balance?. Br. J. Anaesth. 109, 191–199 (2012).
Gómez-Izquierdo, J. C. et al. Goal-directed fluid therapy does not reduce primary postoperative ileus after elective laparoscopic colorectal surgery: A randomized controlled trial. Anesthesiology 127, 36–49 (2017).
Merchea, A. et al. Efficacy and outcomes of intrathecal analgesia as part of an enhanced recovery pathway in colon and rectal surgical patients. Surg. Res. Pract. 1,8174579 (2018).
Pedrazzani, C. et al. Local wound infiltration plus transversus abdominis plane (TAP) block versus local wound infiltration in laparoscopic colorectal surgery and ERAS program. Surg. Endosc. 30, 5117–5125 (2016).
Colibaseanu, D. T. et al. Randomized clinical trial of liposomal bupivacaine transverse abdominis plane block versus intrathecal analgesia in colorectal surgery. Br. J. Surg. 106, 692–699 (2019).
Wongyingsinn, M. et al. Intravenous lidocaine versus thoracic epidural analgesia: A randomized controlled trial in patients undergoing laparoscopic colorectal surgery using an enhanced recovery program. Reg. Anesth. Pain. Med. 36, 241–248 (2011).
Holte, K. et al. Liberal or restrictive fluid administration in fast-track colonic surgery: A randomized, double-blind study. Br. J. Anaesth. 99, 500–508 (2007).
Wongyingsinn, M. et al. Spinal analgesia for laparoscopic colonic resection using an enhanced recovery after surgery programme: Better analgesia, but no benefits on postoperative recovery: A randomized controlled trial. Br. J. Anaesth. 108, 850–856 (2012).
Duffield, J. A. et al. Intraperitoneal local anesthetic instillation and postoperative infusion improves functional recovery following colectomy: A randomized controlled trial. Dis. Colon. Rectum. 61, 1205–1216 (2018).
Kahokehr, A., Sammour, T., Zargar Shoshtari, K., Taylor, M. & Hill, A. G. Intraperitoneal local anesthetic improves recovery after colon resection: A double-blinded randomized controlled trial. Ann. Surg. 254, 28–38 (2011).
Wan, Q., Ding, W., Cui, X. & Zeng, X. CONSORT-epidural dexmedetomidine improves gastrointestinal motility after laparoscopic colonic resection compared with morphine. Medicine 97, e11218 (2018).
Pirrera, B. et al. Transversus abdominis plane (TAP) block versus thoracic epidural analgesia (TEA) in laparoscopic colon surgery in the ERAS program. Surg. Endosc. 32, 376–382 (2018).
Zingg, U. et al. Influence of thoracic epidural analgesia on postoperative pain relief and ileus after laparoscopic colorectal resection: Benefit with epidural analgesia. Surg. Endosc. 23, 276–282 (2009).
Ahn, K.-Y. et al. The effects of inpatient exercise therapy on the length of hospital stay in stages I–III colon cancer patients: Randomized controlled trial. Int. J. Colorectal. Dis. 28, 643–651 (2013).
Ibáñez, N. et al. Isoperistaltic versus antiperistaltic ileocolic anastomosis. Does it really matter? Results from a randomised clinical trial (ISOVANTI). Surg. Endosc. 33, 2850–2857 (2019).
Lee, K.-H. et al. Comparison of anastomotic configuration after laparoscopic right hemicolectomy under enhanced recovery program: Side-to-side versus end-to-side anastomosis. Surg. Endosc. 30(5), 1952–1957 (2016).
Kim, H. O., Lee, S. R., Choi, W. J. & Kim, H. Early oral feeding following laparoscopic colorectal cancer surgery. ANZ. J. Surg. 84, 539–544 (2014).
Grass, F. et al. Ordering a normal diet at the end of surgery-justified or overhasty?. Nutrients 10, 1758 (2018).
Lau, C., Phillips, E., Bresee, C. & Fleshner, P. Early use of low residue diet is superior to clear liquid diet after elective colorectal surgery: A randomized controlled trial. Ann. Surg. 260, 641–647 (2014).
Peters, E. G. et al. Perioperative lipid-enriched enteral nutrition versus standard care in patients undergoing elective colorectal surgery (SANICS II): A multicentre, double-blind, randomised controlled trial. Lancet. Gastroenterol. Hepatol. 3, 242–251 (2018).
Hamamoto, H. et al. The impact of preoperative carbohydrate loading on intraoperative body temperature: A randomized controlled clinical trial. Surg. Endosc. 32, 4393–4401 (2018).
Hyde, L. Z. et al. Alvimopan significantly reduces length of stay and costs following colorectal resection and ostomy reversal even within an enhanced recovery protocol. Dis. Colon Rectum 62, 755–761 (2019).
Obokhare, I. D., Champagne, B., Stein, S. L., Krpata, D. & Delaney, C. P. The effect of alvimopan on recovery after laparoscopic segmental colectomy. Dis. Colon Rectum 54, 743–746 (2011).
Ludwig, K. et al. Alvimopan for the management of postoperative ileus after bowel resection: Characterization of clinical benefit by pooled responder analysis. World J. Surg. 34, 2185–2190 (2010).
Itawi, E. A., Savoie, L. M., Hanna, A. J. & Apostolides, G. Y. Alvimopan addition to a standard perioperative recovery pathway. JSLS 15, 492–498 (2011).
Adam, M. A. et al. Alvimopan provides additional improvement in outcomes and cost savings in enhanced recovery colorectal surgery. Ann. Surg. 264, 6 (2016).
Barletta, J. F., Asgeirsson, T., El-Badawi, K. I. & Senagore, A. J. Introduction of alvimopan into an enhanced recovery protocol for colectomy offers benefit in open but not laparoscopic colectomy. J. Laparoendosc. Adv. Surg. Tech. A 21, 887–891 (2011).
Wen, Y. et al. Alvimopan in the setting of colorectal resection with an ostomy: To use or not to use?. Surg. Endosc. 31, 3483–3488 (2017).
Keller, D. S., Flores-Gonzalez, J.-R., Ibarra, S., Mahmood, A. & Haas, E. M. Is there value in alvimopan in minimally invasive colorectal surgery?. Am. J. Surg. 212, 851–856 (2016).
Shum, N. F. et al. Randomized clinical trial of chewing gum after laparoscopic colorectal resection. Br. J. Surg. 103, 1447–1452 (2016).
Yang, Y. et al. Comparison of efficacy of simo decoction and acupuncture or chewing gum alone on postoperative ileus in colorectal cancer resection: A randomized trial. Sci. Rep. 7, 37826 (2017).
Byrne, C. M., Zahid, A., Young, J. M., Solomon, M. J. & Young, C. J. Gum chewing aids bowel function return and analgesic requirements after bowel surgery: A randomized controlled trial. Colorectal Dis. 20, 438–448 (2018).
Zaghiyan, K. et al. A prospective randomized controlled trial of sugared chewing gum on gastrointestinal recovery after major colorectal surgery in patients managed with early enteral feeding. Dis. Colon Rectum 56, 328–335 (2013).
Lim, P. et al. Sham feeding with chewing gum after elective colorectal resectional surgery: A randomized clinical trial. Ann. Surg 257, 1016–1024 (2013).
Atkinson, C. et al. Randomized clinical trial of postoperative chewing gum versus standard care after colorectal resection. Br. J. Surg. 103, 962–970 (2016).
Müller, S. A. et al. Randomized clinical trial on the effect of coffee on postoperative ileus following elective colectomy. Br. J. Surg. 99, 1530–1538 (2012).
Hasler-Gehrer, S. et al. Does coffee intake reduce postoperative ileus after laparoscopic elective colorectal surgery? A prospective, randomized controlled study: The coffee study. Dis. Colon Rectum 62, 997–1004 (2019).
Dulskas, A., Klimovskij, M., Vitkauskiene, M. & Samalavicius, N. E. Effect of coffee on the length of postoperative ileus after elective laparoscopic left-sided colectomy: A randomized, prospective single-center study. Dis. Colon Rectum 58, 1064–1069 (2015).
Popescu, I. et al. The Ghrelin agonist TZP-101 for management of postoperative ileus after partial colectomy: A randomized, dose-ranging, placebo-controlled clinical trial. Dis. Colon Rectum 53, 126–134 (2010).
Falkén, Y. et al. Intravenous ghrelin accelerates postoperative gastric emptying and time to first bowel movement in humans. Neurogastroenterol. Motil. 25, 474–480 (2013).
Andersen, J. et al. Effect of the laxative magnesium oxide on gastrointestinal functional recovery in fast-track colonic resection: A double-blind, placebo-controlled randomized study. Colorectal Dis. 14, 776–782 (2012).
Gong, J. et al. Randomised clinical trial: Prucalopride, a colonic pro-motility agent, reduces the duration of post-operative ileus after elective gastrointestinal surgery. Aliment Pharmacol. Ther. 43, 778–789 (2016).
Springer, J. E. et al. The effect of simethicone on postoperative ileus in patients undergoing colorectal surgery (SPOT), a randomized controlled trial. Int. J. Surg. 56, 141–147 (2018).
Lohsiriwat, V. Opioid-sparing effect of selective cyclooxygenase-2 inhibitors on surgical outcomes after open colorectal surgery within an enhanced recovery after surgery protocol. World J. Gastrointest. Oncol. 8, 543–549 (2016).
Raju, D. P., Hakendorf, P., Costa, M. & Wattchow, D. A. Efficacy and safety of low-dose celecoxib in reducing post-operative paralytic ileus after major abdominal surgery. ANZ J. Surg. 85, 946–950 (2015).
Danelich, I. M. et al. Early diuresis after colon and rectal surgery does not reduce length of hospital stay: Results of a randomized trial. Dis. Colon Rectum 61, 1187–1195 (2018).
Singh, P. P. et al. Perioperative simvastatin therapy in major colorectal surgery: A prospective, double-blind randomized controlled trial. J. Am. Coll. Surg. 223, 308-320.e1 (2016).
Biondo, S. et al. A double-blinded randomized clinical study on the therapeutic effect of gastrografin in prolonged postoperative ileus after elective colorectal surgery. World J. Surg. 40, 206–214 (2016).
Venara, A. et al. Perioperative transcutaneous tibial nerve stimulation to reduce postoperative ileus after colorectal resection: A pilot study. Dis. Colon Rectum 61, 1080–1088 (2018).
van den Heijkant, T. C. et al. Randomized clinical trial of the effect of gum chewing on postoperative ileus and inflammation in colorectal surgery. Br. J. Surg. 102, 202–211 (2015).
Lambrichts, D. P. V. et al. Nicotine chewing gum for the prevention of postoperative ileus after colorectal surgery: A multicenter, double-blind, randomised, controlled pilot study. Int. J. Colorectal Dis. 32, 1267–1275 (2017).
Vergara-Fernandez, O., Gonzales-Vargas, A. P., Constellanos-Juares, J. C., Salgado-Nesme, N. & Sanchez-Garcia, R. E. Usefulness of gum chewing to decrease postoperative ileus in colorectal surgery with primary anastomosis: A randomized controlled trial [Internet]. Rev. Investig. Clin. 68, 314–318 (2016).
Su’a, B. U. et al. Chewing gum and postoperative ileus in adults: A systematic literature review and meta-analysis. Int. J. Surg. 14, 49–55 (2015).
Short, V. et al. Chewing gum for postoperative recovery of gastrointestinal function. Cochrane Database Syst. Rev. CD006505 (2015).
Vaughan-shaw, P. G., Fecher, I. C., Harris, S. & Knight, J. S. A meta-analysis of the effectiveness of the opioid receptor antagonist alvimopan in reducing hospital length of stay and time to GI recovery in patients enrolled in a standardized accelerated recovery program after abdominal surgery. Dis. Colon Rectum. 55, 611–620 (2012).
Traut, U. et al. Systemic prokinetic pharmacologic treatment for postoperative adynamic ileus following abdominal surgery in adults. Cochrane Database Syst. Rev. CD004930 (2008).
Gustafsson, U. O. et al. Guidelines for perioperative care in elective colorectal surgery: Enhanced recovery after surgery (ERAS) society recommendations: 2018. World J. Surg. 43, 659–695 (2019).
Eamudomkarn, N. et al. Effect of postoperative coffee consumption on gastrointestinal function after abdominal surgery: A systematic review and meta-analysis of randomized controlled trials. Sci. Rep. 8, 17349 (2018).
Hibino, G., Moritani, T., Kawada, T. & Fushiki, T. Caffeine enhances modulation of parasympathetic nerve activity in humans: Quantification using power spectral analysis. J. Nutr. 127, 1422–1427 (1997).
Venara, A. et al. Anti-inflammatory effects of enhanced recovery programs on early-stage colorectal cancer surgery. World J. Surg. 42, 953–964 (2018).
Kalff, J. C., Schraut, W. H., Simmons, R. L. & Bauer, A. J. Surgical manipulation of the gut elicits an intestinal muscularis inflammatory response resulting in postsurgical ileus. Ann. Surg. 228, 652–663 (1998).
Kitazawa, T. & Kaiya, H. Regulation of gastrointestinal motility by motilin and ghrelin in vertebrates. Front. Endocrinol. 10, 278 (2019).
Kehlet, H., Williamson, R., Büchler, M. W. & Beart, R. W. A survey of perceptions and attitudes among European towards the clinical impact and management of postoperative ileus. Colorectal Dis. 3, 245–250 (2005).
Gero, D., Gié, O., Hübner, M., Demartines, N. & Hahnloser, D. Postoperative ileus: In search of an international consensus on definition, diagnosis, and treatment. Langenbecks Arch. Surg. 402, 149–158 (2017).
Chapman, S. J. et al. Systematic review of definitions and outcome measures for return of bowel function after gastrointestinal surgery. BJS Open 3, 1–10 (2018).
Chapman, S. J. et al. Establishing core outcome sets for gastrointestinal recovery in studies of postoperative ileus and small bowel obstruction: Protocol for a nested methodological study. Colorectal Dis. 22, 459–464 (2019).
Day, R. W. et al. Incomplete reporting of enhanced recovery after elements and its impact on achieving quality improvement. Br. J. Surg. 102, 1594–1602 (2015).
Elias, K. M. et al. The reporting on ERAS compliance, outcomes, and elements research (RECOvER) checklist: A joint statement by the ERAS and ERAS USA societies. World J. Surg. 43, 1–8 (2019).
Author information
Authors and Affiliations
Contributions
J.F.H.: conception, design, methodology, statistical analysis and interpretation. Final approval of the version to be published. C.S., A.A., J.M.R., T.V.: collection of data, Provided criticism of the manuscript, drafted the article and revised it for important intellectual content. Final approval of the version to be published. A.V.: conception, design, analysis and interpretation of data, manuscript author, provided criticism of the manuscript, drafted the article and revised it for important intellectual content. Final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hamel, J.F., Sabbagh, C., Alves, A. et al. Comparison of treatment to improve gastrointestinal functions after colorectal surgery within enhanced recovery programmes: a systematic review and meta-analysis. Sci Rep 11, 7423 (2021). https://doi.org/10.1038/s41598-021-86699-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-86699-w
This article is cited by
-
Framework, component, and implementation of enhanced recovery pathways
Journal of Anesthesia (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
