
Abstract
The molecular mechanisms behind aneurysmal subarachnoid haemorrhage (aSAH) are still poorly understood. Expression patterns of miRNAs may help elucidate the post-transcriptional gene expression in aSAH. Here, we evaluate the global miRNAs expression profile (miRnome) of patients with aSAH to identify potential biomarkers. We collected 33 peripheral blood samples (27 patients with cerebral aneurysm, collected 7 to 10 days after the haemorrhage, when usually is the cerebral vasospasm risk peak, and six controls). Then, were performed small RNA sequencing using an Illumina Next Generation Sequencing (NGS) platform. Differential expression analysis identified eight differentially expressed miRNAs. Among them, three were identified being up-regulated, and five down-regulated. miR-486-5p was the most abundant expressed and is associated with poor neurological admission status. In silico miRNA gene target prediction showed 148 genes associated with at least two differentially expressed miRNAs. Among these, THBS1 and VEGFA, known to be related to thrombospondin and vascular endothelial growth factor. Moreover, MYC gene was found to be regulated by four miRNAs, suggesting an important role in aneurysmal subarachnoid haemorrhage. Additionally, 15 novel miRNAs were predicted being expressed only in aSAH, suggesting possible involvement in aneurysm pathogenesis. These findings may help the identification of novel biomarkers of clinical interest.
Similar content being viewed by others


Introduction
Subarachnoid haemorrhage (SAH) is caused by bleeding into the subarachnoid space1,2. When caused by a ruptured cerebral aneurysm, is called aneurysmal subarachnoid haemorrhage (aSAH). The aSAH presents high rates of mortality, ranging from 8% to 67%, and a significant morbidity for those who survive the initial haemorrhage3,4. Cerebral vasospasm (CV), also known as delayed cerebral ischemia (DCI), can be a severe complication of aSAH, contributing to unfavourable outcomes2,5,6.
Risk factors for aSAH include smoking, hypertension, female gender, alcohol intake, and positive family history of SAH, suggesting an active genetic component in the pathophysiology of this condition7,8,9,10. Several studies have found an association between aSAH risk and different genetic polymorphisms, such as in eNOS11,12,13. Nor prevention, neither risk assessment of aSAH has been proposed in the screening protocol of the patients. Therefore, efforts must be made to search for biomarkers capable of indicate the disease status, progression, and treatment responsiveness. Potential biomarkers may include DNA mutations, proteins, mRNA transcripts, and non-coding RNAs (ncRNAs).
Among the ncRNA, microRNAs (miRNAs) are expected to have potential application in the clinical setting. MiRNAs are small RNA molecules (19–25 nucleotides) with well-known biogenesis, which includes processing through the DGCR8/DROSHA, Dicer, Exportin-5, and RISC molecular complexes. Over ~2,500 miRNAs have been identified in humans, which may regulate more than 60% of protein-coding genes14. MiRNAs are characterized by variable expression in cells and tissues, which is influenced by the molecular cell environment. Differential expression of miRNAs has been shown associated with cancer-related diseases15,16, cardiovascular diseases17,18, and neurological conditions19,20. In addition, miRNAs are more resistant to degradation than mRNA and can be detected in fresh, fixed, or frozen tissue and peripheral blood samples. Distinctive patterns of circulating miRNAs have been identified for vascular diseases such as myocardial infarction, atherosclerotic disease and hypertension21,22,23,24. To date, few studies concerning miRNA expression profile in aSAH were published, even less using NGS techniques25,26,27,28,29. Compared to other technologies like qRT-PCR and Microarray, NGS provides high accuracy and sensitivity, and precise identification of miRNA sequences. One of the main advantages of NGS is the possibility of detection of known and novel miRNAs. Other advantages include the detection of miRNA expression levels in species without complete genome available and the use of barcodes during library preparation, allowing sample multiplexing30. Therefore, the purpose of the present study is to apply NGS to evaluate the global miRNA expression profile (miRnome) of patients with and without vasospasm after aSAH and verify potential biomarkers of this condition.
Methods
Sample collection
This study was reviewed and approved by the Ethical Committee of the Ophir Loyola’s Hospital (protocol number: 48199715.2.0000.5550). All study participants or their legal guardian provided informed written consent in accordance with the Helsinki Declaration of 1964. A total of 33 peripheral blood samples, collected at Ophir Loyola’s Hospital between 2014 and 2015, were included in the present study, comprising: (a) six control individuals with no evidence of cerebral aneurysm (verified by exams); (b) 14 patients with cerebral vasospasm after aSAH (Group 1); and (c) 13 patients without cerebral vasospasm after aSAH (Group 2). aSAH patient’s samples were collected 7 to 10 days after the haemorrhage, period when usually is the cerebral vasospasm risk peak31,32. All aSAH patients (n = 27) and controls (n = 6) were submitted to specific examination including computed tomography angiography and evaluated by neuroradiologist specialist. All participants in this study are from Brazil, a miscegenated population. Table 1 shows a summary of the participant characteristics (detailed information is available in Supplementary Material - Additional File 1).
Total RNA extraction and quantification
Peripheral blood samples (5 mL) were collected using Tempus Blood RNA Tube (Thermo Fisher Scientific, US) and stored at −20 °C until extraction. Total RNA was extracted using MagMAX RNA Isolation Kit (Thermo Fisher Scientific, US) and quantified with NanoDrop-1000 spectrophotometer (Thermo Fisher Scientific, US). Agilent RNA ScreenTape assay and 2200 TapeStation Instrument (Agilent Technologies, US) were used to detect and ensure RNA integrity.
Small RNA library construction and sequencing
For small RNA-Seq, 1 (one) μg of total RNA per sample was used for library preparation using TruSeq Small RNA Sample Prep Kits (Illumina, San Diego, CA, USA). Size-distribution was measured with the DNA ScreenTape assay on a 2200 TapeStation system (Agilent Technologies, US) and a real-time PCR with KAPA Library Quantification Kit (Kapa Biosystem, US) was used to quantify and evaluate the quality of each library. A total library pool of 4 nM was sequenced using a MiSeq Reagent Kit v3 150 cycle on a MiSeq System (Illumina, San Diego, CA, USA).
Small RNA-Seq in silico quantification
For the quantification of miRNAs expression levels after sequencing, three steps were followed:
Reads trimming and filtering
We used the Trimmomatic software, version 0.3633 to remove adaptors, low-quality bases and reads with less than 16 nucleotides. The parameter “ILLUMINACLIP TruSeq3-SE.fa:2:30:10” was used to remove read adaptors according to Illumina-specific sequences. “LEADING” and “TRAILING” parameters were set equal to 10 to cut the low-quality bases at the beginning or end of a read. A sliding window cut was applied to remove bases with average quality below 22 using the parameter “SLIDINGWINDOW:3:22”, and reads with less than 16 nucleotides were removed using “MINLEN:16”.
Aligning miRNA read sequences to the human genome
Reads were aligned using STAR, version 02020134, against the human reference genome (Hg19) obtained at UCSC database35. The parameters used include the maximum number of mismatch equal to 3 (“–outFilterMismatchNmax 3”); maximum intron length equal to 1 (“–alignIntronMax 1”); and the minimum number of bases matched to report an alignment was set higher than 16 nucleotides (“–outFilterMatchNmin 16”). The results files, generated as “.sam” by STAR, were manipulated with a set of utilities from Samtools36 and converted to “.bam” files. The “.bam” files contain the same information of the “.sam” files but in a binary conformation.
Measuring miRNA expression levels
For quantification of the expression of each miRNA, we used the HTSeq software, version 0.6.037, using the human genome annotation file (“.gff”) and parameters set explicitly to miRNA and strand-specific modes.
Statistical analysis
Data exploratory analysis was performed with R version 3.4.038, RStudio and shell script. For storage and manage data, we use the relational database management system MySQL. MiRNAs that did not express in any sample (read count < 1) were excluded from downstream analysis. Differential expression analysis was performed using DESeq2 version 1.16.139 and edgeR version 3.18.140 according to their documentation. Two major parameters were considered in all differential expression analysis: adjusted p-value < 0.05 combined with |log2(foldchange)| > 1. Only miRNAs that met these criteria were considered differentially expressed (the complete list is available in Supplementary Material - Additional File 2). The statistical power analysis of the given sample sizes was evaluated using the R package RNASeqPower version 1.18.041. Parameters were estimated considering only data from the differentially expressed miRNAs found. Sequencing coverage by miRNA was averaged between all 33 samples (27 cases + 6 controls) and the overall dispersion (coefficient of variation) was calculated using edgeR’s function “estimateCommonDisp”. Power was estimated for effect values of fold change 1.25, 1.5, 1.75 and 2, and False Discovery Rate’ alpha 0.1, 0.05, and 0.01 (Supplementary Table S1).
For other analyses (presented as boxplots and principal component analysis) the raw data count was normalised by counts per million (CPM). This normalisation is a measure of reads abundance used to compare the expression of miRNA in different samples or libraries sizes. CPM is calculated as follows:
Wilcoxon signed-rank tests were performed to verify the statistical significance when comparing miRNA expression of patients against control.
In silico identification of target genes and novel miRNAs
To identify potential target genes of the differentially expressed miRNAs found, we conducted an in silico analysis using three databases: (i) miRTarBase42, a curated database of miRNA target interactions; (ii) DIANA Tools with Tarbase version 7.043, another manually curated target database; and (iii) miRTargetLink44, that offers detailed information on miRNA interactions in the form of interactive networks figures. All targets described by each database were stored in a local relational database to further manipulation of the information. For analysis, we considered only target genes with evidence of at least two distinct differentially expressed miRNAs (summed from Diana and miRTarBase).
Additionally, to take advantage of miRNA deep sequencing, we used the miRDeep245 software to search potential novel miRNAs molecules. First, an index of the human genome reference (Hg19) was created with Bowtie1 (default parameters)46, then the script “mapper.pl” (available in miRDeep2 package) was used to map reads to the reference and collapse repeated sequences. After that, the script “miRDeep2.pl” was used to identify known and novel miRNAs using human’s mature miRNAs and pre-miRNA hairpins sequences, and species-related miRNAs from chimpanzee and mouse, obtained from the miRBase database (version 21)47. Only miRNAs with a score higher than five were considered for downstream analysis.
Data availability
The raw sequencing reads of all libraries have been deposited at EBI-ENA (PRJEB24635).
Results and Discussion
Overview from small RNA-Seq
MiRNA sequence expression of 33 peripheral blood samples, comprising six control individuals and 27 aSAH patients, were analysed in order to identify potential biomarkers. From aSAH patients, 14 were associated with cerebral vasospasm (Group 1) and 13 without vasospasm (Group 2) (Table 1 and Supplementary Material - Additional File 1). Results section focus on the comparison of all aSAH patients against the control group. Result comparisons of specific subgroups (with and without vasospasm after an aneurysm) are available in Supplementary Material.
The average number of mapped reads per sample was 515,270, varying from 22,325 to 1,604,996. From a list of 2,576 known miRNAs, only 760 were found considered being expressed, with raw read count ≥1 in at least one sample. Considering the data from all samples (aSAH patients and controls), the most abundant miRNA detected was hsa-miR-486-5p (responsible for ~90% of the expression), followed by hsa-miR-92-3p and hsa-miR-181a-5p. Moreover, principal component analysis and hierarchical clustering of the Spearman correlation between the miRNA expression in each sample showed a clear contrast between patient and control samples (Supplementary Figs S1 and S2).
Differential expression analysis
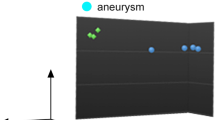
Search for differentially expressed (DE) miRNAs between Group 1 (patients with cerebral vasospasm) and Group 2 (patients without vasospasm) showed no results according to the statistical significance threshold employed (adjusted p-value < 0.05 and |log2(fold change| > 1) (Supplementary Material - Additional Files 2 and 3). Comparing Group 1 and control, two DE miRNAs were found down-regulated: let-7f-5p and hsa-miR-486-5p (Supplementary Fig. S3). For Group 2 against control, three DE miRNAs were found: let-7f-5p and hsa-miR-486-5p (down-regulated) and hsa-miR-146a-5p (up-regulated) (Supplementary Fig. S4). Since no significant differences were found between aSAH Group 1 and Group 2, we compared control samples to all aSAH patients to enhance our statistical power. This analysis identified eight DE miRNAs, with: let-7f-5p, hsa-miR-486-5p, hsa-miR-126-5p, hsa-miR-17-5p and hsa-miR-451a being down-regulated and hsa-miR-146a-5p, hsa-miR-589-5p, and hsa-miR-941 being up-regulated in aSAH patients. Figure 1 and Table 2 presents the statistical analysis results from DESeq2. Using EdgeR, a higher number of miRNAs could be identified being DE (Supplementary Table S2). However, methods showed overlapping results, with the same eight miRNAs being indicated by both (DEseq2 and EdgeR), supporting the results obtained.

DE miRNAs between aSAH patients and control. The x-axis represents the values of log2(fold change) and y-axis are p-value in the scale of log10. Yellow dots are considered DE miRNAs under the conditions of adjusted p-value < 0.05 and |log2(fold change)| > 1. Grey dots are non-DE miRNAs. Note that, the three miRNAs on right of the figure are up-regulated, and five on the left are down-regulated.
Analysis of DE miRNAs expression data showed differences between expression levels of miRNAs among aSAH patients and controls (Fig. 2). Also, is possible to notice the elevated relative expression of hsa-miR-486-5p in both groups (~90% of all expression). The miRNA hsa-miR-486-5p (down-regulated in our results) has been described as one of the most down-regulated miRNAs in lung tumour and contributing to cancer progression by regulating Rho GTPase-activating protein48. This miRNA was described being differentially expressed in patients with gastric adenocarcinoma compared with healthy control49, and its deregulation was found as being a common event in both benign and malignant breast tumours50. In aneurysmal subarachnoid, the hsa-miR-486–5p was described in patients with a poor neurological admission status (WFNS score 4–5) compared with those with a good status (WFNS score 1–3)51. Additionally, another down-regulated miRNA found, hsa-miR-451a, commonly used in panels to evaluate haemolysis, has been related to the rupture or destruction of red blood cells51, which may indicate a relationship with aSAH clinical outcomes.

Heatmap and a hierarchical clustering of eight DE miRNAs. Green colour in top bar refers to aSAH patients and orange colour represents control individuals. In the Heatmap, dark-blue colour corresponds to lower expression, and dark-red colour corresponds to high expression in log scale.
Other miRNAs listed in this study as differentially expressed also has been found in related studies of stroke, subarachnoid haemorrhage or cerebral ischemia, providing additional support to our results and offering insights about the role of these miRNAs. In brief, we comment and discuss each one below.
The hsa-let-7f-5p, whose nomenclature was maintained without “miR”, for historical reasons due to the first description of the Let-7 miRNA precursor in a developmental timing study in Caenorhabditis elegans52, and later found conserved from worms to humans, was observed here being down-regulated in aSAH patients. The hsa-let-7f-5p was also found significantly down-regulated in stroke cases53 and showing similar expression among various stroke samples54.
Another DE miRNA found being down-regulated in aSAH, was the hsa-miR-126-5p. The miR-126 family is expressed in endothelial cells and modulates angiogenesis in vivo55. Targeted deletion of miR-126 in mice has shown to result in vascular leakage and hemorraging56. This miRNA also has been described as down-regulated in different human stroke cases53, validated by stem-loop real-time PCR in young stroke patients (aged between 18–49 years)54 and differentially expressed in circulating blood of patients after stroke29.
The hsa-miR-146a-5p (up-regulated in aSAH patients), is involved in the regulation of inflammation and regulation of innate immune responses in monocytes and macrophages57. Taganov et al. screened for up-regulated miRNAs in monocytic cell line and showed that miR-146a and miR-146b unveiled a pattern of induction in response to a variety of microbial components and proinflammatory cytokines58. Yamasaki et al. in a study with 15 patients with osteoarthritis concluded that miR-146 is intensely expressed and might play a role in osteoarthritis cartilage pathogenesis59. In the same way, hsa-miR-146a has been found up-regulated in brain tissues, that suppress expression of COX-2 in neurological disorders60. Bache et al. reported a relative increase in hsa-miR-146a-5p expression in cerebral fluid from SAH patients with Delayed cerebral ischemia (DCI), compared with those without DCI (P < 0.05)51.
The hsa-miR-17-5p appears to be closely linked to the early evolution of the vertebrate lineage61. However, as miRNAs hsa-let-7f-5p and hsa-miR-126-5p, the hsa-miR-17-5p was listed as differentially expressed in patients after stroke in a study of Tiedt et al.29 and it was one of the 66 miRNAs that exhibited an increase expression in cerebral fluid from SAH patients when compared to neurologically healthy control (p < 0.001) – Supplemental Table II from Bache et al.51.
The miRNAs hsa-miR-589-5p and hsa-miR-941 are still poorly described and found in few related studies. The hsa-miR-589-5p is described in a list of miRNAs induced by hypoxia, that contributes to the pathogenesis of various human diseases including hypertension, stroke and myocardial or cerebral infarction62. Additionally, the hsa-miR-589-5p was described in “The colorectal microRNAome”63 and in a “mammalian microRNA expression atlas”64. Regarding the miRNA hsa-miR-941, it has been described in cervical cancer65, human embryonic stem cells and neural precursors66, and was described as remained significantly associated with incident stroke risk in a study of “Stroke and Circulating Extracellular RNAs”67. More detailed analysis of expression levels between DE miRNAs is shown in Fig. 3. All up-regulated miRNA (hsa-miR-146a-5p, hsa-miR-589-5p and hsa-miR-941) showed a significant difference (p-value < 0.001 using Wilcoxon test) between expression levels of patient and control groups (Fig. 3A). Conversely, for the five down-regulated miRNAs let-7f-5p, hsa-miR-126-5p, hsa-miR-17-5p, hsa-miR-451a, and hsa-miR-486-5p, significant difference was found only for hsa-miR-486-5p (Fig. 3B).

Expression levels of DE miRNAs between groups. The x-axis shows the miRNA and y-axis represent the expression in log10 scale. Data is normalized as counts per million (CPM). Blue colour represents aSAH patients and yellow represents control group. Three asterisks (***) indicate if the data is statistically significant (p-value < 0.001) according to Wilcoxon test; ns is not significant. (A) Up-regulated miRNAs. (B) Down-regulated miRNAs.
Statistical power analysis
Several technical and biological aspects have effect on the variability of RNA-seq experiments68. For an inferential analysis, depending on the desired statistical power, a minimum of three biological replicates is usually enough to achieve reliable results69. For a differential expression analysis, it has been suggested that increasing the number of replicates is preferable over increasing the sequencing depth70,71, with studies recommending from six to 12 biological replicates72. Regarding specifically circulating miRNA studies for biomarkers discovery, it has been shown that small sample sizes can lead to an increase in false positive and false negative results, with studies suggesting at least 7 samples in order to detect with at least 80% of power a 2-fold change in expression levels with a false discovery rate (FDR) of 10%73.
Here we analysed sets of unpaired sample groups with a significant difference in number of replicates. Despite having a considerable number of aSAH case samples (n = 27), our control group size was restricted (n = 6). Therefore, we measured the statistical power estimated to our data, given parameters such as sequencing depth and sample variation. Power estimation was evaluated using the R package RNASeqPower, that accounts for RNA-seq specificities (e.g. technical variation between different runs) by considering negative binomial distributions41. We examined the overall sequencing depths and the coefficient of variation in expression across samples for all eight DE miRNAs found previously. As result we obtained a statistical power of 84% under criteria of at least 2-fold and FDR alpha equal 0.05 (Supplementary Table S1).
In silico identification of miRNA target genes
Target genes for each DE miRNA were retrieved from miRTarBase and DIANA Tools. These two databases accumulate data from different species, and all data are experimentally curated. Database validations are reported by western blot, microarray, and next-generation sequencing experiments. For the eight DE miRNA identified (let-7f-5p, hsa-miR-126-5p, hsa-miR-146a-5p, hsa-miR-17-5p, hsa-miR-451a, hsa-miR-486-5p, hsa-miR-589-5p and hsa-miR-941), miRTarBase indicates 1764 distinct target genes (Supplementary Material - Additional File 4) and DIANA Tools indicates 819 (Supplementary Material - Additional File 5), with 286 targets in common between both approaches. From those 286, 148 targets were found having at least two miRNAs associated considering the sum of the two databases. Some of these genes include proto-oncogenes (MYC, MDM2, and CRK); genes related with caspase activation and apoptosis (PMAIP1, BCL2); cyclin kinase regulators (CCND1, CDKN1A), and growth factors (TGFBR2, VEGFA). Interestingly, two target genes (THBS1 and VEGFA) are related with aSAH, due to their association with thrombospondin and vascular endothelial growth factor (Table 3).
DIANA Tools also provides for each target gene, the association with KEGG Pathway database. Some identified pathways include terms associated with different types of cancer as colorectal, pancreatic and renal; pathways of malaria, fatty acid degradation, PI3K-Akt signalling, focal adhesion, viral carcinogenesis, regulation of actin cytoskeleton, hepatitis B, endocytosis, hippo, WNT and sphingolipid signalling, among others (Supplementary Material - Additional File 5).
Associations between miRNA and its target genes were further explored using the mirTargetLink software. Considering only strong evidence targets, ten genes were found targeted by at least two miRNAs (Fig. 4). Among these genes, five were reported as representative by miRTarBase and DIANA Tools (Table 3, in bold). Notably, the MYC gene (orange rectangle in Fig. 4), had three down-regulated miRNAs associated: hsa-miR-451a, hsa-miR-17-5p, and hsa-miR-126-5p. This gene was also reported by DIANA and miRTarBase (Table 3), suggesting involvement with aneurysmatic subarachnoid haemorrhage. MYC is known for being involved in cell growth, apoptosis, and metabolism74, and was also described as an oncogenic transcription factor75. High-level expression of MYC can favour cell proliferation, inhibit cell differentiation and contributes to tumorigenesis76,77.

Network of DE miRNAs and targets associated. The figure shows only strong evidence associations indicated by the software mirTargetLink and plotted using Cytoscape. Blue colour represents genes with two miRNA interactions; yellow represents more than two miRNA interactions. Brow rectangles represent the miRNAs.
Novel miRNA prediction
The use of Next Generation Sequencing (NGS) technologies provides an excellent approach to identify possible novel molecules. In silico prediction of novel miRNAs was performed using the software mirDeep2. We found 33 potential novel miRNAs with a score higher than 5 (Supplementary Material - Additional File 6). Regions mapped with small differences in the beginning or end of alignments (1–4 nucleotides) were merged and considered being the same miRNA. As a result, 15 miRNAs were identified in distinct positions of the human genome with evidence of reads in 15 samples (Supplementary Material - Additional File 7). These possible novel miRNAs were found only in the aSAH samples, and not in control participants. The number of reads mapped in these molecules varies up to 52 depending on samples (Supplementary Fig. S5). The predicted pre-miRNA with the highest number (52) of mapped reads in a sample is shown in Fig. 5. This miRNA (provisional ID “ch1_125”) is located on chromosome 1 and present evidence of expression in a total of 11 samples from aSAH patients (Supplementary Fig. S5). The predicted secondary structures of the other predicted molecules are available in Supplementary Material - Additional File 8.

Possible novel miRNA identified by mirDeep2. This molecule is found only in 11 samples from aSAH patients, not present in the control samples. (A) Information and possible secondary structure of this novel miRNA. (B) Frequency of reads aligned in each pre-miRNA region. (C) Read alignment.
Conclusions
A global miRNA expression analysis profile of patients after aneurysmal subarachnoid haemorrhage (aSAH) was conducted using small RNA deep-sequencing on an Illumina MiSeq platform. Eight miRNAs were found differentially expressed in aSAH patients, three being up-regulated: hsa-miR-146a-5p, hsa-miR-589-5p, and hsa-miR-941; and five being down-regulated: let-7f-5p, hsa-miR-126-5p, hsa-miR-17-5p, hsa-miR-451a, and hsa-miR-486-5p. Moreover, 148 target genes were identified associated with at least two DE miRNAs indicated by two different approaches. The MYC gene was found having the highest number of strong-related DE miRNAs associated to its regulation, suggesting an important target involved in a complex of subarachnoid haemorrhage. Additionally, 15 potential novel molecules of miRNAs were found occurring only in samples from aSAH patients, as novel players in this complex disease. One specifically, mapped to the human chromosome 1, present in 11 aSAH samples showed an elevated number of reads mapped. These results provide resources for future researchers for identifying novel biomarkers to help the clinical management of patients with a predisposition to develop an aneurysmal subarachnoid haemorrhage.
References
van Gijn, J. & Rinkel, G. J. Subarachnoid haemorrhage: diagnosis, causes and management. Brain 124, 249–278 (2001).
Macdonald, R. L. Delayed neurological deterioration after subarachnoid haemorrhage. Nat. Rev. Neurol. 10, 44–58 (2013).
Nieuwkamp, D. J. et al. Changes in case fatality of aneurysmal subarachnoid haemorrhage over time, according to age, sex, and region: a meta-analysis. Lancet Neurol. 8, 635–642 (2009).
Rivero Rodríguez, D. et al. Predictor’s of mortality in patients with aneurysmal subarachnoid haemorrhage and reebleding. Neurol. Res. Int. 2015, 1–6 (2015).
Macdonald, R. L., Pluta, R. M. & Zhang, J. H. Cerebral vasospasm after subarachnoid hemorrhage: the emerging revolution. Nat. Clin. Pract. Neurol. 3, 256–263 (2007).
Wu, C. T., Wong, C. S., Yeh, C. C. & Borel, C. O. Treatment of cerebral vasospasm after subarachnoid hemorrhage–a review. Acta Anaesthesiol. Taiwan 42, 215–22 (2004).
Broderick, J. P. et al. Major risk factors for aneurysmal subarachnoid hemorrhage in the young are modifiable. Stroke 34, 1375–1381 (2003).
Inagawa, T. Risk factors for aneurysmal subarachnoid hemorrhage in patients in Izumo City, Japan. J. Neurosurg. 102, 60–67 (2005).
Feigin, V. L. et al. Risk factors for subarachnoid hemorrhage: an updated systematic review of epidemiological studies. Stroke 36, 2773–2780 (2005).
Feigin, V. L. et al. Global and regional burden of stroke during 1990–2010: findings from the Global Burden of Disease Study 2010. Lancet 383, 245–254 (2014).
Rosalind Lai, P. M. & Du, R. Role of genetic polymorphisms in predicting delayed cerebral ischemia and radiographic vasospasm after aneurysmal subarachnoid hemorrhage: a meta-analysis. World Neurosurg. 84, 933–941E2 (2015).
Paschoal, E. H. A. et al. Relationship between endothelial nitric oxide synthase (eNOS) and natural history of intracranial aneurysms: meta-analysis. Neurosurg. Rev. 41, 87–94 (2018).
Paschoal, E. H. A. Biomarcadores genéticos na hemorragia subaracnoidea aneurismática em pacientes da Amazônia. (Universidade de São Paulo, 2017).
Etheridge, A., Lee, I., Hood, L., Galas, D. & Wang, K. Extracellular microRNA: a new source of biomarkers. Mutat. Res. 717, 85–90 (2011).
Waingankar, N. et al. Validation of differential expression of microRNA profiles in prostate cancer specimens. J. Clin. Oncol. 32, 203–203 (2014).
Calin, G. A. & Croce, C. M. MicroRNA signatures in human cancers. Nat. Rev. Cancer 6, 857–866 (2006).
Chung, S. H., Gillies, M., Yam, M., Wang, Y. & Shen, W. Differential expression of microRNAs in retinal vasculopathy caused by selective Müller cell disruption. Sci. Rep. 6, 28993 (2016).
Song, M. A., Paradis, A. N., Gay, M. S., Shin, J. & Zhang, L. Differential expression of microRNAs in ischemic heart disease. Drug Discov. Today 20, 223–235 (2015).
Ziats, M. N. & Rennert, O. M. Identification of differentially expressed microRNAs across the developing human brain. Mol. Psychiatry 19, 848–852 (2014).
Wang, C., Ji, B., Cheng, B., Chen, J. & Bai, B. Neuroprotection of microRNA in neurological disorders (Review). Biomed. Rep. 2, 611–619 (2014).
Li, C., Pei, F., Zhu, X., Duan, D. D. & Zeng, C. Circulating microRNAs as novel and sensitive biomarkers of acute myocardial Infarction. Clin. Biochem. 45, 727–732 (2012).
Wang, F. et al. Atherosclerosis-related circulating miRNAs as novel and sensitive predictors for acute myocardial infarction. PLoS One 9, e105734 (2014).
Romaine, S. P., Charchar, F. J., Samani, N. J. & Tomaszewski, M. Circulating microRNAs and hypertension–from new insights into blood pressure regulation to biomarkers of cardiovascular risk. Curr. Opin. Pharmacol. 27, 1–7 (2016).
Kheyfets, V. O. et al. Circulating miRNAs in pediatric pulmonary hypertension show promise as biomarkers of vascular function. Oxid. Med. Cell. Longev. 2017, 1–11 (2017).
Stylli, S. S. et al. miRNA expression profiling of cerebrospinal fluid in patients with aneurysmal subarachnoid hemorrhage. J. Neurosurg. 126, 1131–1139 (2017).
Su, X. W. et al. Circulating microRNA 132-3p and 324-3p profiles in patients after acute aneurysmal subarachnoid hemorrhage. PLoS One 10, e0144724 (2015).
Lu, G. et al. Circulating microRNAs in delayed cerebral infarction after aneurysmal subarachnoid hemorrhage. J. Am. Heart Assoc. 6, e005363 (2017).
Lai, N. S. et al. Serum microRNAs are non-invasive biomarkers for the presence and progression of subarachnoid haemorrhage. Biosci. Rep. 37, BSR20160480 (2017).
Tiedt, S. et al. RNA-seq identifies circulating miR-125a-5p, miR-125b-5p, and miR-143-3p as potential biomarkers for acute ischemic stroke. Circ. Res. 121, 970–980 (2017).
Eminaga, S., Christodoulou, D. C., Vigneault, F., Church, G. M. & Seidman, J. G. Quantification of microRNA expression with next-generation sequencing. Curr. Protoc. Mol. Biol. 0 4, Unit-4.17 (2013).
Lominadze, G., Lessen, S. & Keene, A. Vasospasm risk in surgical ICU patients with grade I subarachnoid hemorrhage. Neurohospitalist 6, 20–23 (2016).
Shakur, S. F. & Farhat, H. I. Cerebral vasospasm with ischemia following a spontaneous spinal subarachnoid hemorrhage. Case Rep. Med. 2013, 934143 (2013).
Bolger, A. M., Lohse, M. & Usadel, B. Trimmomatic: a flexible trimmer for Illumina sequence data. Bioinformatics 30, 2114–2120 (2014).
Dobin, A. et al. STAR: ultrafast universal RNA-seq aligner. Bioinformatics 29, 15–21 (2013).
Kent, W. J. et al. The human genome browser at UCSC. Genome Res. 12, 996–1006 (2002).
Li, H. et al. The sequence alignment/map format and SAMtools. Bioinformatics 25, 2078–2079 (2009).
Anders, S., Pyl, P. T. & Huber, W. HTSeq–a Python framework to work with high-throughput sequencing data. Bioinformatics 31, 166–169 (2015).
Core Team, R. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria, ISBN 3-900051-07-0 (2012).
Love, M. I., Huber, W. & Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 15, 550 (2014).
Robinson, M. D., McCarthy, D. J. & Smyth, G. K. edgeR: a Bioconductor package for differential expression analysis of digital gene expression data. Bioinformatics 26, 139–140 (2010).
Hart, T., Komori, H. K., LaMere, S., Podshivalova, K. & Salomon, D. R. Finding the active genes in deep RNA-seq gene expression studies. BMC Genomics 14, 778 (2013).
Chou, C. H. et al. miRTarBase 2016: updates to the experimentally validated miRNA-target interactions database. Nucleic Acids Res. 44, D239–D247 (2016).
Vlachos, I. S. et al. DIANA-TarBasev7.0: indexing more than half a million experimentally supported miRNA:mRNA interactions. Nucleic Acids Res. 43, D153–D159 (2015).
Hamberg, M. et al. MiRTargetLink—miRNAs, genes and interaction networks. Int. J. Mol. Sci. 17, 564 (2016).
Friedländer, M. R. et al. Discovering microRNAs from deep sequencing data using miRDeep. Nat. Biotechnol. 26, 407–415 (2008).
Langmead, B., Trapnell, C., Pop, M. & Salzberg, S. L. Ultrafast and memory-efficient alignment of short DNA sequences to the human genome. Genome Biol. 10, R25 (2009).
Kozomara, A. & Griffiths-Jones, S. miRBase: annotating high confidence microRNAs using deep sequencing data. Nucleic Acids Res. 42, D68–D73 (2014).
Wang, J. et al. Downregulation of miR-486-5p contributes to tumor progression and metastasis by targeting protumorigenic ARHGAP5 in lung cancer. Oncogene 33, 1181–1189 (2014).
Chen, H. et al. Expression and prognostic malue of miR-486-5p in patients with gastric adenocarcinoma. PLoS One 10, e0119384 (2015).
Tahiri, A. et al. Deregulation of cancer-related miRNAs is a common event in both benign and malignant human breast tumors. Carcinogenesis 35, 76–85 (2014).
Bache, S. et al. MicroRNA changes in cerebrospinal fluid after subarachnoid hemorrhage. Stroke 48, 2391–2398 (2017).
Rougvie, A. E. Control of developmental timing in animals. Nat. Rev. Genet. 2, 690–701 (2001).
Sepramaniam, S. et al. Circulating microRNAs as biomarkers of acute stroke. Int. J. Mol. Sci. 15, 1418–1432 (2014).
Tan, K. S. et al. Expression profile of microRNAs in young stroke patients. PLoS One 4, e7689 (2009).
van Solingen, C. et al. Antagomir-mediated silencing of endothelial cell specific microRNA-126 impairs ischemia-induced angiogenesis. J. Cell. Mol. Med. 13, 1577–1585 (2009).
Wang, S. et al. The endothelial-specific microRNA miR-126 governs vascular integrity and angiogenesis. Dev. Cell 15, 261–271 (2008).
Sonkoly, E., Ståhle, M. & Pivarcsi, A. MicroRNAs and immunity: novel players in the regulation of normal immune function and inflammation. Semin. Cancer Biol. 18, 131–140 (2008).
Taganov, K. D., Boldin, M. P., Chang, K. J. & Baltimore, D. NF-kappaB-dependent induction of microRNA miR-146, an inhibitor targeted to signaling proteins of innate immune responses. Proc. Natl. Acad. Sci. USA 103, 12481–12486 (2006).
Yamasaki, K. et al. Expression of microRNA-146a in osteoarthritis cartilage. Arthritis Rheum. 60, 1035–1041 (2009).
Iyer, A. et al. MicroRNA-146a: a key regulator of astrocyte-mediated inflammatory response. PLoS One 7, e44789 (2012).
Tanzer, A. & Stadler, P. F. Molecular evolution of a microRNA cluster. J. Mol. Biol. 339, 327–335 (2004).
Wu, C. et al. Hypoxia potentiates microRNA-mediated gene silencing through posttranslational modification of Argonaute2. Mol. Cell. Biol. 31, 4760–4774 (2011).
Cummins, J. M. et al. The colorectal microRNAome. Proc. Natl. Acad. Sci. USA 103, 3687–3692 (2006).
Landgraf, P. et al. A mammalian microRNA expression atlas based on small RNA library sequencing. Cell 129, 1401–1414 (2007).
Lui, W. O., Pourmand, N., Patterson, B. K. & Fire, A. Patterns of known and novel small RNAs in human cervical cancer. Cancer Res. 67, 6031–6043 (2007).
Goff, L. A. et al. Ago2 immunoprecipitation identifies predicted microRNAs in human embryonic stem cells and neural precursors. PLoS One 4, e7192 (2009).
Mick, E. et al. Stroke and circulating extracellular RNAs. Stroke 48, 828–834 (2017).
Pereira, M. A., Imada, E. L. & Guedes, R. L. M. RNA‐seq: Applications and Best Practices in Applications of RNA-Seq and Omics Strategies (IntechOpen 2017).
Conesa, A. et al. A survey of best practices for RNA-seq data analysis. Genome Biology 17, 13 (2016).
Liu, Y., Zhou, J. & White, K. P. RNA-seq differential expression studies: more sequence or more replication? Bioinformatics 30, 301–304 (2014).
Ching, T., Huang, S. & Garmire, L. X. Power analysis and sample size estimation for RNA-Seq differential expression. RNA 20, 1684–1696 (2014).
Schurch, N. J. et al. How many biological replicates are needed in an RNA-seq experiment and which differential expression tool should you use? RNA 22, 839–851 (2016).
Kok, M. G. M. et al. Small sample sizes in high-throughput miRNA screens: a common pitfall for the identification of miRNA biomarkers. Biomol. Detect. Quantif. 15, 1–5 (2018).
Dang, C. V. c-Myc target genes involved in cell growth, apoptosis, and metabolism. Mol. Cell. Biol. 19, 1–11 (1999).
Zeller, K. I., Jegga, A. G., Aronow, B. J., O’Donnell, K. A. & Dang, C. V. An integrated database of genes responsive to the Myc oncogenic transcription factor: identification of direct genomic targets. Genome Biol. 4, R69 (2003).
Nesbit, C. E. et al. Genetic dissection of c-myc apoptotic pathways. Oncogene 19, 3200–3212 (2000).
Kim, J., Lee, J. & Iyer, V. R. Global identification of Myc target genes reveals its direct role in mitochondrial biogenesis and its E-box usage in vivo. PLoS One 3, e1798 (2008).
Acknowledgements
We would like to thank the patients (and their relatives) who initially consented to be selected for participating and have provided the follow-up for some time months that has contributed substantially to the Global miRNAs expression profile in this series. This study was financial supported by CAPES (Coordenacão de Aperfeicoamento Pessoal de Nível Superior), Rede de Pesquisa em Genômica Populacional Humana (RPGPH) - 3381/2013 CAPES-BioComputacional, CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico), and PROPESP/UFPA (Universidade Federal do Pará). ÂNDREA RIBEIRO-DOS-SANTOS supported by CNPq/Produtividade (CNPQ 304413/2015-1); SIDNEY SANTOS supported by CNPq/Produtividade (CNPq 305258/2013-3). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
Ândrea Ribeiro-dos-Santos, E.B., E.S.Y., E.H.A.P., F.M.P.J., M.J.T., S.S. designed and coordinated the study. V.A.P.A.B. collected and prepared the samples. A.F.V., P.P., T.V. performed the experimental analyses. Arthur Ribeiro-dos-Santos, F.M., K.P.L., R.A.V. performed the bioinformatical and statistical analyses. K.P.L., R.A.V., T.V. wrote the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lopes, K.d.P., Vinasco-Sandoval, T., Vialle, R.A. et al. Global miRNA expression profile reveals novel molecular players in aneurysmal subarachnoid haemorrhage. Sci Rep 8, 8786 (2018). https://doi.org/10.1038/s41598-018-27078-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-27078-w
This article is cited by
-
Identification and Characterization of miRNAs and Their Predicted mRNAs in the Larval Development of Pearl Oyster Pinctada fucata
Marine Biotechnology (2022)
-
Construction of competitive endogenous RNA network reveals regulatory role of long non-coding RNAs in intracranial aneurysm
BMC Neuroscience (2021)
-
Diagnostic and prognostic potential of circulating miRNAs for intracranial aneurysms
Neurosurgical Review (2021)
-
Inflammatory Responses Induced by the Rupture of Intracranial Aneurysms Are Modulated by miRNAs
Molecular Neurobiology (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
