
Abstract
Cocaine use disorder (CUD) patients display heterogenous symptoms and unforeseeable responses to available treatment approaches, highlighting the need to identify objective, accessible biobehavioral signatures to predict clinical trial success in this population. In the present experiments, we employed a task-based behavioral and pharmacogenetic-fMRI approach to address this gap. Craving, an intense desire to take cocaine, can be evoked by exposure to cocaine-associated stimuli which can trigger relapse during attempted recovery. Attentional bias towards cocaine-associated words is linked to enhanced effective connectivity (EC) from the anterior cingulate cortex (ACC) to hippocampus in CUD participants, an observation which was replicated in a new cohort of participants in the present studies. Serotonin regulates attentional bias to cocaine and the serotonergic antagonist mirtazapine decreased activated EC associated with attentional bias, with greater effectiveness in those CUD participants carrying the wild-type 5-HT2CR gene relative to a 5-HT2CR single nucleotide polymorphism (rs6318). These data suggest that the wild-type 5-HT2CR is necessary for the efficacy of mirtazapine to decrease activated EC in CUD participants and that mirtazapine may serve as an abstinence enhancer to mitigate brain substrates of craving in response to cocaine-associated stimuli in participants with this pharmacogenetic descriptor. These results are distinctive in outlining a richer “fingerprint” of the complex neurocircuitry, behavior and pharmacogenetics profile of CUD participants which may provide insight into success of future medications development projects.
Similar content being viewed by others

Introduction
Combined cognitive and pharmacotherapeutic approaches optimize recovery from opioid use disorder [1], however, efforts to validate medication candidates for cocaine use disorder (CUD) have largely been negative. Participants are typically screened for inclusion in clinical trials based upon the diagnosis of CUD employing the Diagnostic and Statistical Manual (DSM) of Mental Disorders (DSM) [2, 3]. Recent consumption of cocaine is detected by its metabolite benzoylecgonine in urine [4], and the number of clean urine days is a common endpoint for success in clinical trials of CUD therapeutics [5]. However, the diagnosis and detection of cocaine do not encapsulate the profound heterogeneity of individual patients which arises due to developmental and genetic distinctions and interrelated CUD-related pathologies [6,7,8,9]. These factors likely contribute to the poor signal detection in clinical trials for CUD medications, and the field recognizes the need to identify and tailor new strategies for maximizing the success of treatment to suppress relapse and extend recovery [10, 11]. One concept is to validate a “biobehavioral signature” which reflects indicators of underlying neurobiological processes and pathogenesis to predict therapeutic success [12, 13]. For example, several genetic markers have been identified as predicting depression, an observation which has recently been validated within an independent cohort of participants with clinically severe depression [14, 15]. Similarly, beyond DSM criteria and identification of a drug-positive urine, readily accessible and objective indicators of CUD processes will allow clinically informed distinctions between CUD patients with the goal to align treatment options to biobehavioral profiles.
Exposure to cocaine-associated cues contributes to continued cocaine use as well as relapse during abstinence and recovery [6, 16, 17]. Our understanding of brain responses to these cues has been greatly enriched by studies employing functional imaging technologies. Notably, fMRI studies have illustrated that CUD impacts not only the function of single brain regions of interest, but importantly the interactions between brain regions which drive behavioral features of the disorder [6]. For example, we recently discovered that the amplified deployment of attentional bias toward cocaine-related stimuli in CUD participants associates with increased anterior cingulate cortex (ACC) to hippocampus effective (directional) connectivity (EC) [18], an observation replicated in opioid use disorder participants [19]. In the present study, this cue-associated ACC→ hippocampus EC activation was selected as a dependent variable to test hypotheses related to the proposed involvement of the serotonergic system in cue-activated brain mechanisms in CUD participants.
Preclinical observations support a prominent role for the serotonin (5-HT) 5-HT2A receptor (5-HT2AR) and 5-HT2CR systems in the neurobiology of relapse vulnerability [17, 20]. Long-term cocaine self-administration is associated with increased cortical 5-HT2AR availability in monkeys [21], suggesting that the sensitivity to cocaine-associated cues during abstinence may be related to the degree of higher 5-HT2AR expression (and function) consequent to cocaine self-administration. Notably, selective 5-HT2AR antagonists (e.g., M100907, pimavanserin) [22,23,24,25,26,27,28,29,30,31,32,33,34,35] and the 5-HT2A/2CR antagonist mirtazapine [26,27,28,29] exhibit potency and efficacy to suppress cue-evoked cocaine-seeking in animals and decrease craving, cocaine use, and some psychiatric symptoms in CUD participants [30]. Relatedly, a cortical 5-HT2CR knockdown elevated cocaine-seeking and increased local 5-HT2AR expression [36, 37], suggesting that the 5-HT2CR system is an important regulator of endogenous 5-HT2AR control of the neural bases of cocaine cue-evoked behaviors.
The single nucleotide polymorphism (SNP) in the 5-HT2CR gene (rs6318) results in hypofunctional cellular signaling in vitro [38, 39]. This SNP also predicts the highest attentional bias toward cocaine-associated stimuli in CUD participants [40]. Given preclinical observations, we postulated that mirtazapine would exhibit greater effectiveness to suppress attentional bias-linked ACC → hippocampus EC in CUD participants with the wild-type HTR2C relative to the hypofunctional HTR2C SNP. The outcomes confirm a behavioral and pharmacogenetic-fMRI signature of CUD participants which may ultimately aid in maximizing therapeutic success in this persistent disorder.
Methods
Participants
This study was approved by the local ethics committee and performed in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki). Twenty-eight, non-treatment seeking participants who met DSM-IV criteria for CUD were included in the study (Table 1). Each was genotyped (Taqman Assays-on-Demand, ThermoFisher Scientific, Foster City, CA) for the HTR2C gene using an automated allele scoring platform [41], as previously described [40]. Participants were blinded and randomized to receive placebo and mirtazapine (15 mg) two hours prior to the first and second scans, respectively; scans were scheduled approximately two weeks apart. Each participant provided written informed consent, was negative for physical and medical histories as well as psychiatric disorders assessed by the Structured Clinical Interview for DSM-IV [42]. Immediately prior to MRI scanning, each participant was verified to be negative for breath alcohol, and urinalysis for cocaine and other abusable stimulants, barbiturates, benzodiazepines, opioids, Δ [9]-tetrahydrocannabinol, tricyclic antidepressants, and pregnancy (for females). Eight subjects were excluded from the 36 original participants (10 females) who initiated the experiment (see Supplementary Table 1). The remaining 28 participants (n = 15 wild-type HTR2C and n = 13 HTR2C SNP) were included for final analysis. Each participant was financially compensated for their time.
Cocaine-word Stroop task
We employed the cocaine-word Stroop task [18] within the fMRI scanner to assess attentional bias towards cocaine-related stimuli (see Supplementary Information for details). As in our previous studies [18], attentional bias to cocaine cues was calculated as the mean reaction time (RT) during the cocaine word (CW) blocks minus the mean RT during the neutral word (NW) blocks, i.e., ΔRT = RT (CW) minus RT (NW). Only correct-response trials were included when calculating the mean reaction times.
fMRI data acquisition
MRI scans were acquired using a Philips Medical Systems (Best, Netherlands) Ingenia wide-bore dStream 3 T MRI scanner, with a 32-channel receive head coil. A spin-echo echo planar pulse sequence was used with: parallel imaging acceleration-factor 2.0, repetition-time 2500 ms, echo-time 75 ms, flip-angle 90 degrees, field-of-view 240 mm (anterior to posterior) × 240 mm (left to right) × 123.75 mm (foot to head), in-plane resolution 3.75 mm × 3.75 mm, 25 axial slices, slice-thickness 3.75 mm, interslice-gap 1.25 mm, 112 repetitions per run after 10 dummy acquisitions. Total duration per run was approximately 5 min.
fMRI preprocessing
See Supplementary Information for the description of fMRI preprocessing.
Dynamic causal modeling
Dynamic causal modeling (DCM) [43] was used to measure the ECs elicited by the cocaine-word Stroop fMRI task [18, 19] following acute oral administration of placebo or mirtazapine with experimenters blinded to the drug condition until the initiation of data analysis. fMRI-based DCM is a biophysical model of the underlying neuronal connectivity and how the neuronal connectivity generates the observed BOLD signal [43]. DCM with the deterministic option, as implemented in Statistical Parametric Mapping 12 (SPM12) software (Revision 7219; http://www.fil.ion.ucl.ac.uk/spm/) was used for EC analysis. The use of DCM in drug-related, attentional bias studies has been described [18, 19].
Candidate a priori DCM nodes
Based on studies suggesting similarity in attentional bias for drug cues across drug classes [18, 44,45,46], we used left (L) and right (R) ACC, L and R medial orbitofrontal cortex (MOFC), L and R posterior cingulate cortex (PCC), L and R insula, L and R hippocampus, and L and R striatum as the a priori selected DCM nodes as recently published [19]. The DCM nodes were specifically constrained by the task-related brain activation (see Supplementary Information) in two steps: (1) to determine if a candidate DCM node was selected as a final DCM node (to be selected, the brain region corresponding to the candidate DCM node needed to exhibit at least 10 active voxels on the brain activation found by any of the SPM second level analyses), and (2) to localize the position of each selected DCM node, i.e., to use the voxel with the local maximum t value as the center of the sphere (the DCM node). After constraint by the brain activations found in this study, the following six brain regions were selected as final DCM nodes: (1) L-ACC (x = −4, y = 47, z = 4); (2) R-MOFC (x = 4, y = 51, z = −11); (3) L-PCC (x = −8, y = −56, z = 20); (4) L-insula (x = −34, y = −19, z = 5); (5) R-hippocampus (x = 31, y = −13, z = −20); and (6) R-putamen (x = 20, y = 6, z = −6). Each node was a sphere with 6 mm radius, and the x, y, z values (in mm) are the MNI coordinates of the center of each node determined by the t-test maximum within the fMRI activation cluster corresponding to that node. For each node, the functional activation BOLD time-series, which was used for DCM analysis, was extracted using the previous methods [47, 48].
Driving/modulatory inputs for the DCM analyses from placebo scans
Based on two types of task blocks (CW and NW), two parametric regressors, called “Placebo All-Words” and “Placebo CW-minus-NW,” respectively, were created for the DCM analyses. The All-Words regressor was All Words (CW and NW) minus implicit baseline, and the CW-minus-NW regressor was CW minus NW. In other words, the first regressor was non-specific word effects, relative to the implicit baseline, while the second modeled the special effect of CW over NW. The All-Words regressor was used as a single input to all the nodes of the DCM (driving input), and the CW-minus-NW regressor was used as a putative modulator (modulatory input) of all ECs (i.e., a modulatory input is an experimental factor eliciting change in EC). The detailed method of constructing these regressors can be found online (https://github.com/HaukeHillebrandt/SPM_connectome).
Driving/modulatory inputs for the DCM analyses testing the effects of mirtazapine
In a separate DCM analysis, the effects of mirtazapine were evaluated based on the contrast between the mirtazapine CW-modulation (similarly defined as above for the placebo scan) and the placebo CW-modulation. Towards that end, the placebo and mirtazapine scans were combined using the SPM12 command “spm_fmri_concatenate”. Then, two DCM parametric regressors, called “Two-scan All-Words” and “mirtazapine-minus-placebo,” respectively, were created for these DCM analyses. The “Two-scan All-Words” parametric regressor reflects the common features of the CW and NW in both placebo and mirtazapine scans, and was used as a single input to the DCM (driving input). The mirtazapine-minus-placebo parametric regressor was defined as the mirtazapine CW-modulation minus the placebo CW-modulation. This parametric regressor reflects the specific effects of mirtazapine CW-modulation over placebo CW-modulation. In this study, the change of EC (relative to the endogenous connectivity) for the mirtazapine-CW modulation minus placebo CW-modulation is termed as “mirtazapine-minus-placebo modulatory change”.
Parametric Empirical Bayes (PEB) analysis to detect most parsimonious EC model
After specifying an initial fully connected model (i.e., there were two bidirectional endogenous connectivities between any two nodes, the driving input affected all the DCM nodes, and the modulatory input affected all the endogenous connectivities, see Fig. 1), the PEB analysis [49], as implemented in DCM for SPM12 (Revision 7219), was used to conduct DCM group level analyses for the EC parameters. Corresponding to the three hypotheses (i.e., the replication of the positive association between ACC → hippocampus EC and attentional bias; the magnitude of the cue-related ACC → hippocampus EC would be reduced after mirtazapine administration; this mirtazapine-induced ACC → hippocampus EC reduction would be greater in the CUD participants with wild-type HTR2C gene compared to those with HTR2C SNP, the following PEB analyses were conducted: (1A) test the placebo CW-modulation (vs. zero) across all participants; (1B) test the linear regression of placebo CW-modulation on attentional bias across all participants; (2) test the mirtazapine-minus-placebo modulatory change (vs. zero) across all participants; and (3) test the difference in mirtazapine-minus-placebo modulatory change between the participants with the wild-type HTR2Cand the HTR2C SNP. Here, an EC finding was considered reliable (e.g., a modulatory effect is different from zero) if Bayesian posterior probability (PP) > 0.95 (corresponding to a Bayes-factor of 3). See Supplementary Information for more information about PP and the advantages of DCM-PEB posterior inferences, including the avoidance of multiple-comparison problem [43, 50, 51]. In DCM, EC is in unit of hertz (Hz) because it is rate of change (rate constants) [52]. For example, placebo CW-modulation is the rate of change in the EC due to the modulatory inputs (CW relative to NW).

The six DCM nodes are illustrated as gold spheres, and the dark red lines with arrows represent the endogenous connectivities. The All-Words driving input (green line with arrow) affected all six nodes, and the modulator (e.g., mirtazapine CW-modulator) affected all endogenous connectivities. Whether the driving input effect to a node (or the modulatory effect on an EC) was different from zero was determined based on the posterior probability (see Results). ACC, anterior cingulate cortex; MOFC, medial orbitofrontal cortex; INS, insula; HIPP, hippocampus; PCC, posterior cingulate cortex; PUT, putamen. The left side of this figure aligns with the left brain hemisphere.
Results
Non-imaging results
As illustrated in Table 1, there were no significant differences in demographic or substance use parameters, difference in abstinence time between the first and second scans (three participants had missing data), route of cocaine administration, nor the number of days between the placebo and mirtazapine scans for the wild-type and HTR2CSNP subgroups. The frequency (~50%) of the HTR2C SNP in our largely African American pool was higher than expected in the general population (~20%) (1000 Genome [53]). Among all the 28 participants, 22 smoked cocaine and six used cocaine intranasally (Table 1). All participants exhibited clean urines prior at both visits. Table 2 shows that baseline values in accuracy in the task based, cocaine-word Stroop task were comparable across the entire sample, indicating that there were no obvious evidence of withdrawal symptoms (e.g., hypersomnia) in the participants who were negative for cocaine and other substances [54, 55]. Attentional bias did not differ in participants with the wild-type and HTR2C SNP during the placebo (t26 = 0.55, p = 0.59) or mirtazapine scan (t26 = 1.29, p = 0.21), nor was the change of attentional bias from placebo scan to mirtazapine scan different (t = 0.67, df = 26, p = 0.51). Non-parametric statistical methods were used to analyze accuracy which is non-Gaussian distributed (see Supplementary Information for details).
Brain activation results for localizing DCM nodes
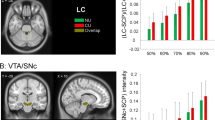
The brain activation results used to constrain the DCM nodes are shown in the Supplementary Information. See Fig. 2 and Supplementary Table 2 for detailed information regarding the brain activations used to constrain the L-ACC and the R-MOFC nodes. See Fig. 3 and Supplementary Table 3 for detailed information regarding additional brain activations used to constrain the remaining four DCM nodes.

The brain activation clusters shown were identified by a SPM second level one-sample t-test analysis for the placebo scan and for all participants (CW minus NW > 0), with cluster-defining threshold t = 2.4 and uncorrected two-tailed cluster level p < 0.05. Scale on the color bar represents voxel t values. The nodes (spheres) are larger than the exact ones for demonstration purpose.

These brain activations were found by a SPM second level t-test comparison of the two genotype groups, with cluster-defining threshold t = 2.4 and uncorrected two-tailed cluster level p < 0.05. This analysis found that, during the mirtazapine scan, the participants with the wild-type HTR2Cexhibited greater cocaine word-elicited activation than those with the HTR2C SNP. Scale on the color bar represents voxel t values. The nodes (spheres) are larger than the exact ones for demonstration purpose.
DCM-PEB connectivity results
The following PEB analyses were conducted in correspondence with our three hypotheses: (1) the positive association between ACC → hippocampus EC and attentional bias will be replicated; (2) the magnitude of the cue-related ACC → hippocampus EC will be reduced after mirtazapine administration; (3) mirtazapine-induced reduction in ACC → hippocampus EC will be greater in the CUD participants with wild-type HTR2C gene compared to those with HTR2C SNP. As mentioned above, the PEB analysis employs Bayesian posterior inference and eschews the multiple-comparison problem because of the lack of false positives without the need to correct the EC results for multiple comparisons.
PEB analysis for hypothesis #1
We first tested if the mean of placebo CW-modulation was different from zero (Hypothesis #1A) for each EC across all participants. For each EC, the mean placebo CW-modulation and the corresponding PP are shown in Supplementary Table 4. As shown in Fig. 4, and Supplementary Table 4, the mean placebo CW-modulation of the L-ACC → R-hippocampus EC (i.e., the hypothesized EC) was −0.1218 Hz, with PP = 1.We then tested the linear regression of the placebo CW-modulation on attentional bias (ΔRT) for each EC and across all the participants (Hypothesis #1B). For each EC, the regression slope (or regression coefficient) beta and the corresponding PP are shown in Supplementary Table 4. The regression of the placebo CW-modulation of the L-ACC → R-hippocampus EC (i.e., the hypothesized EC) on attentional bias scores exhibited a reliable positive regression slope (regression parameter beta = 0.0029, PP = 1. The positive linear relationship between the placebo CW-modulation of the L-ACC → R-hippocampus EC and attentional bias suggests that reduction of the CW-modulation of the L-ACC → R-hippocampus EC has the potential to reduce attentional bias.

PEB analysis for test of hypothesis #2
We tested if the mirtazapine-minus-placebo modulatory change was different from zero for each EC across all participants. For each EC, the mean mirtazapine-minus-placebo modulatory change and the corresponding PP are shown in Supplementary Table 4. Specifically, the mean mirtazapine-minus-placebo modulatory change in the L-ACC → R-hippocampus EC (i.e., the hypothesized EC) was negative with strong confidence (−0.2390 Hz; PP = 1), suggesting a reliable mirtazapine-related decrease of CW-modulation of the L-ACC → R-hippocampus EC for all participants (Fig. 4, blue line). Because the mirtazapine-minus-placebo modulatory change was relative to the placebo CW-modulation (baseline − 0.1218 Hz), the CW modulatory change upon mirtazapine scan was therefore −0.3608 Hz as shown in Fig. 4 (blue line). See Supplementary Information for the non-hypothesized ECs which were altered by the mirtazapine and also showed reliable (PP = 1) linear relationships between placebo CW-modulation and attentional bias.
PEB analysis for hypothesis #3
We tested if the difference of the placebo CW-modulation for each EC differed between the participants with the wild-type and HTR2C SNP. For each EC, the group difference on mean placebo CW-modulation and the corresponding PP are shown in Supplementary Table 5. Specifically, the mean of the placebo CW-modulation of the L-ACC → R-hippocampus EC was identical (−0.1218 Hz) for both wild-type and HTR2C SNP participants (Fig. 4). The difference of the mirtazapine-minus-placebo modulatory change for each EC was also assessed between the participants carrying the wild-type and HTR2C SNP. For each EC, the group difference (HTR2C SNP minus wild-type HTR2C) of mean placebo CW-modulation and the corresponding PP are shown in Supplementary Table 5. In particular, the group difference (HTR2C SNP minus wild-type HTR2C) of the mirtazapine-minus-placebo modulatory change of the L-ACC → R-hippocampus EC was 0.7355 Hz with PP = 1. In two post hoc analyses, we measured the mirtazapine-minus-placebo modulatory change separately in each of the two groups (HTR2C SNP and wild-type HTR2C). These post hoc analyses indicated that the mirtazapine CW-modulation was 0.0810 Hz for theHTR2C SNP group and −0.6545 Hz for the wild-type HTR2C group as shown in Fig. 3, suggesting that the decreased mirtazapine-minus-placebo modulatory change of L-ACC → R-hippocampus EC (−0.2390 Hz, PP = 1; found in the PEB analysis for test of hypothesis #2) was mainly seen in the wild-type HTR2C group (−0.6545 Hz for the wild-type HTR2Cvs. 0.0810 Hz forHTR2C SNP group).
Discussion
A primary challenge is to integrate brain, behavior, and genetic substrates of CUD to ultimately craft strategies to rectify the propensity to relapse during recovery. The present study objectively evaluated attentional bias toward cocaine-associated cues within the context of functional connectivity and a pharmacogenetic analysis in CUD participants. Using Bayesian posterior inference, we found that the L-ACC → R-hippocampus EC under the placebo condition positively associated with attentional bias, replicating previous findings [18, 19], and uncovered unique ECs of interest (see additional Results/Discussion in Supplementary Information). Intriguingly, compared to placebo, mirtazapine decreased the L-ACC → R-hippocampus EC in tandem with reduced attentional bias for all CUD participants, with effectiveness identified as greater in CUD participants carrying the wild-type HTR2C. These results are distinctive in outlining a deeper description of the complex neurocircuitry, behavior and pharmacogenetic profile of CUD participants [3, 9, 56].
We found that, across all CUD participants in the present study, the L-ACC → R-hippocampus EC positively associated with attentional bias, replicating outcomes in a different CUD participant cohort [18] and in an opioid use disorder sample [19]. We interpret this replicated, positive linear relationship as reflecting individual differences in one or more brain processes including, but not limited to, retrieval of hippocampus-mediated episodic memories related to drug use [18, 19], the level of drug cue-related plasticity in the hippocampus [19, 57], and/or the transformation of reward-related information from ACC → hippocampus [58]. The findings in the current study are consistent with our hypothesis that the ACC → hippocampus EC may be a neurocircuit related to drug cue reactivity generalized across substance use disorders [19]. We speculate that this neurocircuit may serve as a key brain substrate of craving in response to drug-associated cues.
The 5-HT2A/2CR antagonist mirtazapine decreased the L-ACC → R-hippocampus EC in tandem with reduced attentional bias for all CUD participants, with outcomes predicated on the HTR2C genotype. Given that cellular studies indicate reduced functionality of the 5-HT2CR carrying the rs6318 SNP [38, 39], the present observations suggest that mirtazapine effectiveness to suppress attentional bias-associated L-ACC → R-hippocampus EC is linked to the degree of 5-HT2CR functionality. Relatedly, CUD participants with the rs6318 SNP exhibit significantly higher attentional bias toward drug cues relative to carriers of the wild-type gene [40], and may be more resistant to mirtazapine in the absence of a maximally functional 5-HT2CR. Although speculative, this line of thought is consistent with observations that describe the interactivity of the 5-HT2AR and 5-HT2CR systems in vivo and in vitro (see Introduction) [16, 17]. Furthermore, we demonstrated that a selective 5-HT2CR antagonist augmented cocaine-mediated behaviors in rats, an outcome which is lost with repeated administration of cocaine [59]. These data suggest that 5-HT2CR systems may be dysregulated in carriers of the rs6318 SNP coupled to conditions of repeated cocaine administration which is likely the case for the CUD participants who have ~14 years of lifetime cocaine use. These data may be interpreted to suggest that the wild-type 5-HT2CR is necessary for the efficacy of mirtazapine to decrease activated EC in CUD participants. While future studies are required to further interrogate the interrelationship between 5-HT2CR and 5-HT2AR systems in drug-related behaviors in humans with CUD, our present results suggest that mirtazapine may serve as an abstinence enhancer to mitigate brain substrates of craving in response to cocaine-associated stimuli particularly for participants with the normal function HTR2C.
Reliable effects of mirtazapine were observed at the EC level; however, the effects of mirtazapine were not observed at the behavioral level, and at the contrast-elicited univariate brain activation level. The lack of statistically significant univariate brain activation results at the group level is consistent with previous studies investigating drug-cue related attentional bias [18, 60]. The reliable effects of mirtazapine on EC from the DCM analysis are consistent with the theory that the brain connectivity approach is more sensitive than univariate activation analysis in detecting neuronal alterations in neurological disorders [61]. The findings on the ACC → hippocampus EC are consistent with the results found in a separate CUD population [18] and in a population with opioid use disorder [19]. Considering findings that individual differences in attentional bias have been predictive of treatment dropout and relapse within CUD treatment populations [45, 62], we believe that our EC findings may have important clinical implications and support further research on the utility of DCM in detecting effects of the treatment.
These findings should be interpreted within several limitations. (1) Both within-group [18, 60, 63, 64] and between-group designs [65,66,67,68] have been used to study drug cue reactivity. The present study employed a within-group design as non-drug users are unlikely to exhibit attentional bias toward cocaine-associated cues. However, larger studies employing strategies such as drug images and/or tactile stimuli, or actual gaze-fixation as captured by eye-tracking [69] provide assays with perhaps greater saliency than drug-related-words in the study of attentional bias in the future. (2) The brain activation and the EC modulatory changes were based on the contrast between CW trials and NW trials in a block design, and thus may have been slightly confounded by the sporadic incorrect responses (less than 9% for all trials) [62]. (3) As discussed previously [18], a limited number of nodes are practical in DCM analysis, but inclusion of additional DCM nodes will allow for more complete interrogation of neurocircuitry important for cocaine cue reactivity in the future. (4) Mirtazapine is a potent 5-HT2AR/5-HT2CR antagonist, but does exhibit affinity for histamine and norepinephrine receptors, actions that could contribute to the observed outcomes through central or peripheral actions, including sedative effects [70]. (5) The sample size was small for the between-group analysis. However, the findings related to the ACC → hippocampus EC are consistent with the results found across samples investigating CUD [18] and opioid use disorder [19]. This consistency reduces the likelihood that the results of the between group analysis are chance findings, and future studies will expand on our initial findings.
In summary, the current study replicated the previous findings that the ACC → hippocampus EC is positively associated with drug cue related attentional bias. Importantly, mirtazapine decreased this ACC → hippocampus EC, with greater effectiveness in those CUD participants carrying the wild-type 5-HT2CR gene relative to the 5-HT2CR SNP rs6318. These results implicate serotonergic substrates that underlie sensitivity to cocaine-associated stimuli in CUD participants with a specific pharmacogenetic descriptor, outlining a richer “fingerprint” of the complex neurocircuitry, behavior and pharmacogenetics profile of CUD participants which may provide important implication for future medications development for CUD.
References
Sofuoglu M. Cognitive enhancement as a pharmacotherapy target for stimulant addiction. Addiction. 2010;105:38–48.
NSDUH. Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality. (September 4, 2014). The NSDUH Report: Substance Use and Mental Health Estimates from the 2013 National Survey on Drug Use and Health: Overview of Findings. Rockville, MD: NSDUH, 2014.
Hasin DS, O’Brien CP, Auriacombe M, Borges G, Bucholz K, Budney A, et al. DSM-5 criteria for substance use disorders: recommendations and rationale. Am J Psychiatry. 2013;170:834–51.
Schmitz JM, Green CE, Stotts AL, Lindsay JA, Rathnayaka NS, Grabowski J, et al. A two-phased screening paradigm for evaluating candidate medications for cocaine cessation or relapse prevention: modafinil, levodopa-carbidopa, naltrexone. Drug Alcohol Depend. 2014;136:100–7.
McCann DJ, Ramey T, Skolnick P. Outcome measures in medication trials for substance use disorders. Curr Treat Options Psychiatry. 2015;2:113–21.
Koob GF, Volkow ND. Neurobiology of addiction: a neurocircuitry analysis. Lancet Psychiatry. 2016;3:760–73.
Regier PS, Jagannathan K, Franklin TR, Wetherill RR, Langleben DD, Gawyrsiak M, et al. Sustained brain response to repeated drug cues is associated with poor drug-use outcomes. Addict Biol. 2021;26:e13028.
Land MA, Ramesh D, Miller AL, Pyles RB, Cunningham KA, Moeller FG, et al. Methylation patterns of the HTR2A associate with relapse-related behaviors in cocaine-cependent participants. Front Psychiatry. 2020;11:532.
Bough KJ, Amur S, Lao G, Hemby SE, Tannu NS, Kampman KM, et al. Biomarkers for the development of new medications for cocaine dependence. Neuropsychopharmacology. 2014;39:202–19.
Lopez-Quintero C, Hasin DS, de Los Cobos JP, Pines A, Wang S, Grant BF, et al. Probability and predictors of remission from life-time nicotine, alcohol, cannabis or cocaine dependence: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Addiction. 2011;106:657–69.
Lopez-Quintero C, Perez de los Cobos J, Hasin DS, Okuda M, Wang S, Grant BF, et al. Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug Alcohol Depend. 2011;115:120–30.
Strimbu K, Tavel JA. What are biomarkers? Curr Opin HIV AIDS. 2010;5:463–6.
Trivedi MH, McGrath PJ, Fava M, Parsey RV, Kurian BT, Phillips ML, et al. Establishing moderators and biosignatures of antidepressant response in clinical care (EMBARC): Rationale and design. J Psychiatr Res. 2016;78:11–23.
Niculescu MD, Craciunescu CN, Zeisel SH. Dietary choline deficiency alters global and gene-specific DNA methylation in the developing hippocampus of mouse fetal brains. FASEB J. 2006;20:43–9.
Le-Niculescu H, Roseberry K, Gill SS, Levey DF, Phalen PL, Mullen J, et al. Precision medicine for mood disorders: objective assessment, risk prediction, pharmacogenomics, and repurposed drugs. Mol Psychiatry. 2021;26:2776–804.
Cunningham KA, Anastasio NC. Serotonin at the nexus of impulsivity and cue reactivity in cocaine addiction. Neuropharmacology. 2014;76:460–78.
Cunningham KA, Howell LL, Anastasio NC. Serotonin neurobiology in cocaine use disorder. In: Müller CP, Cunningham KA, editors. Handbook of the behavioral neurobiology of serotonin. London, United Kingdom: Academic Press, 2020, pp 745–802.
Ma L, Steinberg JL, Cunningham KA, Bjork JM, Lane SD, Schmitz JM, et al. Altered anterior cingulate cortex to hippocampus effective connectivity in response to drug cues in men with cocaine use disorder. Psychiatry Res Neuroimaging. 2018;271:59–66.
Ma L, Steinberg JL, Bjork JM, Taylor BA, Arias AJ, Terplan M, et al. Cingulo-hippocampal effective connectivity positively correlates with drug-cue attentional bias in opioid use disorder. Psychiatry Res Neuroimaging. 2019;294:110977.
Howell LL, Cunningham KA. Serotonin 5-HT2 receptor interactions with dopamine function: implications for therapeutics in cocaine use disorder. Pharm Rev. 2015;67:176–97.
Sawyer EK, Mun J, Nye JA, Kimmel HL, Voll RJ, Stehouwer JS, et al. Neurobiological changes mediating the effects of chronic fluoxetine on cocaine use. Neuropsychopharmacology. 2012;37:1816–24.
Nic Dhonnchadha BA, Fox RG, Stutz SJ, Rice KC, Cunningham KA. Blockade of the serotonin 5-HT2A receptor suppresses cue-evoked reinstatement of cocaine-seeking behavior in a rat self-administration model. Behav Neurosci. 2009;123:382–96.
Sholler DJ, Stutz SJ, Fox RG, Boone EL, Wang Q, Rice KC, et al. The 5-HT2A Receptor (5-HT2AR) Regulates Impulsive Action and Cocaine Cue Reactivity in Male Sprague-Dawley Rats. J Pharm Exp Ther. 2019;368:41–9.
Murnane KS, Winschel J, Schmidt KT, Stewart LM, Rose SJ, Cheng K, et al. Serotonin 2A receptors differentially contribute to abuse-related effects of cocaine and cocaine-induced nigrostriatal and mesolimbic dopamine overflow in nonhuman primates. J Neurosci. 2013;33:13367–74.
Barnes NM, Ahern GP, Becamel C, Bockaert J, Camilleri M, Chaumont-Dubel S, et al. International union of basic and clinical pharmacology. CX. Classification of receptors for 5-hydroxytryptamine; Pharmacology and function. Pharm Rev. 2021;73:310–520.
Barbosa Mendez S, Salazar-Juarez A. Mirtazapine decreased induction and expression of cocaine + nicotine-induced locomotor sensitisation in rats. World J Biol Psychiatry. 2020;21:595–611.
Barbosa Mendez S, Salazar-Juarez A. Mirtazapine attenuates anxiety- and depression-like behaviors in rats during cocaine withdrawal. J Psychopharmacol. 2019;33:589–605.
Barbosa-Mendez S, Leff P, Arias-Caballero A, Hernandez-Miramontes R, Heinze G, Salazar-Juarez A. Mirtazapine attenuates cocaine seeking in rats. J Psychiatr Res. 2017;92:38–46.
Salazar-Juarez A, Barbosa-Mendez S, Jurado N, Hernandez-Miramontes R, Leff P, Anton B. Mirtazapine prevents induction and expression of cocaine-induced behavioral sensitization in rats. Prog Neuropsychopharmacol Biol Psychiatry. 2016;68:15–24.
Nanni-Alvarado R, Gonzalez M, Lima C, Marín-Navarrete R, Barbosa-Méndez S, Salazar-Juárez A. Effect of mirtazapine on craving in cocaine-dependent patients. Int J Mental Health Addict. 2021.
Graves SM, Rafeyan R, Watts J, Napier TC. Mirtazapine, and mirtazapine-like compounds as possible pharmacotherapy for substance abuse disorders: evidence from the bench and the bedside. Pharm Ther. 2012;136:343–53.
Hoyer D. Functional correlates of serotonin 5-HT1 recognition sites. J Recept Res. 1988;8:59–81.
de Boer T. The pharmacologic profile of mirtazapine. J Clin Psychiatry. 1996;57:19–25.
Marek GJ, Carpenter LL, McDougle CJ, Price LH. Synergistic action of 5-HT2A antagonists and selective serotonin reuptake inhibitors in neuropsychiatric disorders. Neuropsychopharmacology. 2003;28:402–12.
Cunningham KA, Anastasio NC, Fox RG, Stutz SJ, Bubar MJ, Swinford SE, et al. Synergism between a serotonin 5-HT2A receptor (5-HT2AR) antagonist and 5-HT2CR agonist suggests new pharmacotherapeutics for cocaine addiction. ACS Chem Neurosci. 2013;4:110–21.
Anastasio NC, Stutz SJ, Fink LH, Swinford-Jackson SE, Sears RM, DiLeone RJ, et al. Serotonin (5-HT) 5-HT2A Receptor (5-HT2AR):5-HT2CR Imbalance in Medial Prefrontal Cortex Associates with Motor Impulsivity. ACS Chem Neurosci. 2015;6:1248–58.
Anastasio NC, Stutz SJ, Fox RG, Sears RM, Emeson RB, DiLeone RJ, et al. Functional status of the serotonin 5-HT2C receptor (5-HT2CR) drives interlocked phenotypes that precipitate relapse-like behaviors in cocaine dependence. Neuropsychopharmacology. 2014;39:370–82.
Land MA, Chapman HL, Davis-Reyes BD, Felsing DE, Allen JA, Moeller FG, et al. Serotonin 5-HT2C receptor Cys23Ser single nucleotide polymorphism associates with receptor function and localization In Vitro. Sci Rep. 2019;9:16737.
Okada M, Northup JK, Ozaki N, Russell JT, Linnoila M, Goldman D. Modification of human 5-HT(2C) receptor function by Cys23Ser, an abundant, naturally occurring amino-acid substitution. Mol Psychiatry. 2004;9:55–64.
Anastasio NC, Liu S, Maili L, Swinford SE, Lane SD, Fox RG, et al. Variation within the serotonin (5-HT) 5-HT(2)C receptor system aligns with vulnerability to cocaine cue reactivity. Transl Psychiatry. 2014;4:e369.
van den Oord EJ, Jiang Y, Riley BP, Kendler KS, Chen X. FP-TDI SNP scoring by manual and statistical procedures: a study of error rates and types. Biotechniques. 2003;34:610–6. 618-620, 622 passim
First MB, Spitzer RL, Gibbon M, Williams JBW. Structured clinical interview for DSM-IV axis I disorders--patient edition (SCID-I/P, Version 2.0). New York: Biometrics Research Department, New York State Psychiatric Institute, 1996.
Friston KJ, Harrison L, Penny W. Dynamic causal modelling. Neuroimage. 2003;19:1273–302.
Hanlon CA, Dowdle LT, Gibson NB, Li X, Hamilton S, Canterberry M, et al. Cortical substrates of cue-reactivity in multiple substance dependent populations: transdiagnostic relevance of the medial prefrontal cortex. Transl Psychiatry. 2018;8:186.
Zhang M, Ying J, Wing T, Song G, Fung DSS, Smith H. A systematic review of attention biases in opioid, cannabis, stimulant use disorders. Int J Environ Res Public Health. 2018;15:1138.
Ma L, Steinberg JL, Bjork JM, Taylor BA, Arias AJ, Terplan M. et al. Cingulo-hippocampal effective connectivity positively correlates with drug-cue attentional bias in opioid use disorder. Psychiatry Res Neuroimaging. 2019;294:110977.
Ma L, Steinberg JL, Cunningham KA, Lane SD, Bjork JM, Neelakantan H, et al. Inhibitory behavioral control: a stochastic dynamic causal modeling study comparing cocaine dependent subjects and controls. NeuroImage Clin. 2015;7:837–47.
Ma L, Steinberg JL, Cunningham KA, Lane SD, Kramer LA, Narayana PA, et al. Inhibitory behavioral control: a stochastic dynamic causal modeling study using network discovery analysis. Brain Connect. 2015;5:177–86.
Friston KJ, Litvak V, Oswal A, Razi A, Stephan KE, van Wijk BC, et al. Bayesian model reduction and empirical Bayes for group (DCM) studies. Neuroimage. 2016;128:413–31.
Friston KJ, Penny W. Posterior probability maps and SPMs. Neuroimage. 2003;19:1240–9.
Van Overwalle F, Van de Steen F, Marien P. Dynamic causal modeling of the effective connectivity between the cerebrum and cerebellum in social mentalizing across five studies. Cogn Affect Behav Neurosci. 2019;19:211–23.
Zeidman P, Jafarian A, Corbin N, Seghier ML, Razi A, Price CJ, et al. A guide to group effective connectivity analysis, part 1: first level analysis with DCM for fMRI. Neuroimage. 2019;200:174–90.
Paes LA, Torre OHD, Henriques TB, de Mello MP, Celeri E, Dalgalarrondo P, et al. Association between serotonin 2C receptor gene (HTR2C) polymorphisms and psychopathological symptoms in children and adolescents. Braz J Med Biol Res. 2018;51:e7252.
Gawin FH, Kleber HD. Abstinence symptomatology and psychiatric diagnosis in cocaine abusers. Clinical observations. Arch Gen Psychiatry. 1986;43:107–13.
Coffey SF, Dansky BS, Carrigan MH, Brady KT. Acute and protracted cocaine abstinence in an outpatient population: a prospective study of mood, sleep and withdrawal symptoms. Drug Alcohol Depend. 2000;59:277–86.
Kwako LE, Bickel WK, Goldman D. Addiction biomarkers: dimensional approaches to understanding addiction. Trends Mol Med. 2018;24:121–8.
Dacher M, Nugent FS. Opiates and plasticity. Neuropharmacology. 2011;61:1088–96.
Rolls ET. The cingulate cortex and limbic systems for emotion, action, and memory. Brain Struct Funct. 2019;224:3001–18.
Filip M, Bubar MJ, Cunningham KA. Contribution of serotonin (5-hydroxytryptamine; 5-HT) 5-HT2 receptor subtypes to the hyperlocomotor effects of cocaine: acute and chronic pharmacological analyses. J Pharm Exp Ther. 2004;310:1246–54.
Goldstein RZ, Tomasi D, Rajaram S, Cottone LA, Zhang L, Maloney T, et al. Role of the anterior cingulate and medial orbitofrontal cortex in processing drug cues in cocaine addiction. Neuroscience. 2007;144:1153–9.
Rowe JB. Connectivity analysis is essential to understand neurological disorders. Front Syst Neurosci. 2010;4:20948582.
Smith DG, Ersche KD. Using a drug-word Stroop task to differentiate recreational from dependent drug use. CNS Spectr. 2014;19:247–55.
Hester R, Garavan H. Neural mechanisms underlying drug-related cue distraction in active cocaine users. Pharm Biochem Behav. 2009;93:270–7.
Marhe R, Luijten M, van de Wetering BJ, Smits M, Franken IH. Individual differences in anterior cingulate activation associated with attentional bias predict cocaine use after treatment. Neuropsychopharmacology. 2013;38:1085–93.
Li Q, Li W, Wang H, Wang Y, Zhang Y, Zhu J, et al. Predicting subsequent relapse by drug-related cue-induced brain activation in heroin addiction: an event-related functional magnetic resonance imaging study. Addict Biol. 2015;20:968–78.
Yang Z, Xie J, Shao YC, Xie CM, Fu LP, Li DJ, et al. Dynamic neural responses to cue-reactivity paradigms in heroin-dependent users: an fMRI study. Hum Brain Mapp. 2009;30:766–75.
Ray S, Haney M, Hanson C, Biswal B, Hanson SJ. Modeling causal relationship between brain regions within the drug-cue processing network in chronic cocaine smokers. Neuropsychopharmacology. 2015;40:2960–8.
Wang Y, Wang H, Li W, Zhu J, Gold MS, Zhang D, et al. Reduced responses to heroin-cue-induced craving in the dorsal striatum: effects of long-term methadone maintenance treatment. Neurosci Lett. 2014;581:120–4.
Potthoff J, Jurinec N, Schienle A. Placebo effects on visual food cue reactivity: an eye-tracking investigation. Front Psychiatry. 2019;10:525.
Abo-Zena RA, Bobek MB, Dweik RA. Hypertensive urgency induced by an interaction of mirtazapine and clonidine. Pharmacotherapy. 2000;20:476–8.
Xia M, Wang J, He Y. BrainNet Viewer: a network visualization tool for human brain connectomics. PLoS One. 2013;8:e68910.
Sokolov AA, Zeidman P, Erb M, Ryvlin P, Pavlova MA, Friston KJ. Linking structural and effective brain connectivity: structurally informed Parametric Empirical Bayes (si-PEB). Brain Struct Funct. 2019;224:205–17.
Hariri AR, Drabant EM, Weinberger DR. Imaging genetics: perspectives from studies of genetically driven variation in serotonin function and corticolimbic affective processing. Biol Psychiatry. 2006;59:888–97.
Hariri AR, Weinberger DR. Imaging genomics. Br Med Bull. 2003;65:259–70.
Acknowledgements
This work was financially supported by National Institute on Drug Abuse (NIDA) grants U54 DA038999 (FGM) and P50 DA033935 (KAC), and the Center for Addiction Research at the University of Texas Medical Branch, as well as UL1TR002649 (FGM) which supports the imaging infrastructure for VCU. We would like to extend our gratitude to those participants recruited into this study and to our research teams for adherence to study design and recruitment efforts.
Author information
Authors and Affiliations
Contributions
FGM, KAC, and LM designed the experiment. LM analyzed all data, and wrote up the original manuscript. LM, KAC, and FGM revised the manuscript. All authors edited and reviewed the manuscript and approved the final version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
FGM has past research funding from Indivior Pharmaceuticals and Nektar Therapeutics for research unrelated to this study. KAC and NCA have current research funding from VidaLibreBio, Inc., for research unrelated to this study. Other authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ma, L., Cunningham, K.A., Anastasio, N.C. et al. A serotonergic biobehavioral signature differentiates cocaine use disorder participants administered mirtazapine. Transl Psychiatry 12, 187 (2022). https://doi.org/10.1038/s41398-022-01934-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41398-022-01934-w
