
Abstract
Physical inactivity and low consumption of fruits and vegetables (FV) during adolescence may persist through adulthood, putting adolescents at risk of developing chronic diseases. Although studies from high-income countries have reported differences in FV consumption and physical activity (PA) between adolescent boys and girls, few exist from low-and-middle-income countries (LMICs). In this study, we examined patterns of FV consumption and PA among adolescent boys and girls in LMICs. Country selection was based on availability of Global School-Based Student Health Survey (GSHS) data from 2004 to 2013. The total analytic sample was 164,771 adolescents from 49 LMICs. Descriptive statistics were generated to determine adolescents meeting the World Health Organization (WHO) recommendations for FV and PA. A Rao-Scott adjusted chi-square statistic was computed to assess gender differences. Less than 30% of adolescents across all countries met the WHO guidelines for FV consumption or PA. Morocco (29.5%) and India (29.5%) however had the highest percentage of adolescents meeting recommendations for FV and PA, respectively. Adolescent boys were more active than girls, and this difference was more notable in the Middle East and North African region. Adolescents achieving the WHO recommendations for daily consumption of FV and PA were consistently low in all countries.
Similar content being viewed by others

Introduction
Non-communicable diseases (NCDs), such as cancer, diabetes, and cardiovascular disease, are the leading cause of death worldwide1. Currently, NCDs are responsible for about 70% of deaths1. NCDs are especially important in low- and-middle-income countries, where more than three-quarters of NCD deaths occur1. It is well known that risk of NCDs is primarily related to four behavioral risk factors: tobacco use, physical inactivity, an unhealthy diet, and excessive alcohol use2,3. It is a public health priority to promote healthy lifestyles as well as monitor levels of behavioral risk factors in all age groups, including children and adolescents. For this purpose, the WHO has established recommendations for adolescents for minimal levels of physical activity (PA) and dietary intake of fruits and vegetables (FV). Currently, the WHO recommends at least 60 minutes of moderate-to-vigorous physical activity each day4, and a dietary intake of at least 400 grams of FV each day (roughly equivalent to five servings of FV/day)5.
Despite these WHO recommendations, current evidence indicates that adolescents eat far less than the recommended five daily servings of FV. For example, a study by Peltzer & Pengpid6 in seven African countries (Botswana, Kenya, Senegal, Swaziland, Tanzania, Uganda, and Zambia) found that most adolescents (77.5%) did not meet the recommended daily servings of FV. Similarly, Doku et al.7 found that 56% and 48% of adolescents in Ghana rarely (≤3 days/week) consumed fruits and vegetables respectively. In China, Shi et al.8 found that less than 50% of school children ate fruits daily. Also, in the North Gaza strip of Palestinian Territories, Abudayya et al.9 found that only 11.6% of boys and 16.2% of girls consumed fruits daily. This shows that FV consumption is consistently low in many LMICs.
Studies have also shown gender differences concerning the daily intake of FV. For example, in a review of determinants of FV intake among children and adolescents, Rasmussen et al.10 found that of the 49 studies reviewed, 27 studies found that girls had a higher consumption of fruits and vegetables compared to boys. In 18 studies, there were no differences in the intake of FV between adolescents’ boys and girls. Lastly, in four studies, the authors found that boys had a higher FV intake compared to girls10.
Also, it appears children and youth between the ages of 5–17 commonly do not engage in at least 60 minutes of moderate- to vigorous-intensity PA daily4. Moreover, studies have shown that PA declines during adolescence, especially among girls11,12. In an examination of PA patterns among adolescents using the Global School-based Student Health Survey (GSHS) and the Health Behavior in School-aged Children (HBSC) survey, Hallal et al.13 found that 80.3% of adolescents between 13–15 years from 105 countries did not meet the recommended daily PA. The authors also found that girls were less active than boys13.
Similarly, in 2010, the WHO found that globally 81% of adolescents aged 11−17 did not meet the daily physical activity recommendation14. The study results showed that adolescent girls recorded a higher percentage (84%) of insufficient PA compared to adolescent boys (78%)14. When disaggregating the PA data by WHO regions, the Eastern Mediterranean Region (88%), the African Region (85%) and the Western Pacific Region (85%) were ranked highest among regions reporting insufficient PA among adolescents. In all WHO regions, adolescent girls were less active than boys14. Thus, the adolescence represents a critical period to encourage and create a conducive environment to be active, thereby minimizing the risk of NCDs, especially among girls.
However, there are few cross-national studies from LMICs examining patterns of FV consumption and physical activity among adolescent boys and girls. The purpose of this study was to compare FV consumption and PA behavior patterns among adolescent girls and boys in 49 LMICs. We hypothesize that there are differences between the FV consumption and PA behavior patterns among adolescent girls and boys in LMICs.
Methods
Study design and sampling method
This study utilizes an ecologic study design to compare patterns of FV consumption and PA among adolescents from countries and regions demarcated by the World Bank as LMICs. The World Bank regions are Sub-Saharan Africa, Middle East and North Africa, South Asia, Latin America and the Caribbean, Europe and Central Asia and East Asia and the Pacific15. The study sample of LMICs included countries from the regions demarcated by the World Bank if they had (1) publicly available data on FV intake and PA behaviors), and (2) data available to allow the assessment of differences between adolescent boys and girls for these health behaviors.
Data and Sample
The primary data source is the Global School-based Student Health Survey (GSHS). The GSHS is a standardized survey developed by the WHO in collaboration with the United Nations International Children’s Emergency Fund, the United Nations Educational, Scientific and Cultural Organization, and the United Nations Program on HIV/AIDS, with technical assistance provided by the Centers for Disease Control and Prevention. The GSHS is a collaborative surveillance project designed to help countries measure and assess health behaviors and protective factors among students between the ages of 13 to 17 years. It allows countries to develop priorities, establish programs, and advocate for resources for youth health programs and policies16.
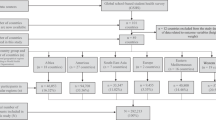
As of December 2013, 90 countries (mostly LMICs) had completed the GSHS, and representatives from over 120 countries have been trained to administer the GSHS16. GSHS data from 2004 to 2013 that were publicly available for LMICs15 were used. According to the World Bank, these are countries that had a gross national income (GNI) of less than $12,616 in 201215. A total of 49 countries with publicly available data on dietary behaviors and PA for adolescents met this definition for inclusion in our study. Figure 1 shows the LMICs included in the study (n = 49 countries).

Selection process for LMICs based on available GSHS national data between 2004–2013.
Survey Measures
The survey measures used were based on the following GSHS questions17:
Fruit; i) “During the past 30 days, how many times per day did you usually eat fruits, such as COUNTRY SPECIFIC EXAMPLES?” Response options were; (A) I did not eat fruit during the past 30 days (B) Less than one time per day (C) 1 time per day (D) 2 times per day (E) 3 times per day (F) 4 times per day (G) 5 or more times per day.
Vegetables; ii) “During the past 30 days, how many times per day did you usually eat vegetables, such as COUNTRY SPECIFIC EXAMPLES?”The response options were (A) I did not eat vegetables during the past 30 days (B) Less than one time per day (C)1 time per day (D) 2 times per day (E) 3 times per day (F) 4 times per day (G)5 or more times per day.
Physical Activity; iii) “During the past 7 days, on how many days were you physically active for a total of at least 60 minutes per day?” The response options; A) 0 days B) 1 day C) 2 days D) 3 days E) 4 days F) 5 days G) 6 days H) 7 days.
Data analysis
The data were analyzed using SPSS version 21 software (SPSS, Inc., Chicago, IL). The GSHS employs a complex sampling design, and the data were analyzed taking into account this sampling design. The weighting process was also used. This process adds weights, stratum and primary sampling unit (PSU) to every student record in the GSHS data file to reflect the weighting process and the 2-staged sampling design. The weight variable allows generalizability of the GSHS results to the entire students’ population whereas the stratum and PSU account for the 2-stage sample design used for the GSHS. Specifically, the stratum reflects the GSHS sampling process at the first level, which is done in schools and the PSU reflects the second level of the GSHS sampling process conducted in classrooms18.
Descriptive statistics were generated to determine the number and percentage of adolescents in each of the LMICs meeting the WHO recommendations of daily intake of FV and PA. In generating the descriptive statistics, the variables took values of 1 (two otherwise) for i) consumption of fruits: adequate (2 or more/day), ii) consumption of vegetables: adequate (3 or more/day), iii) consumption of FV: adequate (adequate on both FV), iv) PA: adequate (60 minutes/day).The Rao-Scott adjusted chi-square statistic was used to test if there was a statistically significant difference between adolescent boys and girls in meeting the WHO recommendations of daily fruit servings, daily vegetable servings, daily FV servings and daily PA for each country and odds ratios were also calculated. The Rao-Scott adjusted chi-square statistic takes into consideration the complex sample design utilized in the GSHS data collection. The p-value of the adjusted F- statistics generated was used in determining statistical significance because it provides a better approximation of the significance19.
Availability of data and material
The datasets generated and/or analyzed during the current study are available at http://www.who.int/chp/gshs/datasets/en/.
Results
Figure 2 summarizes the pattern of FV consumption and PA among adolescents in LMICs grouped by World Bank regions. The sample represented 164,771 adolescents from 49 LMICs. There was significant variability regarding the outcomes of interest throughout the different regions and countries included in this study. In all countries, less than 50% of adolescents consumed five or more FV per day (Fig. 2). Morocco had the highest proportion of adolescents consuming the recommended daily FV intake (29.5%). Lastly, adolescents in India were the most active (29.5%) in terms of meeting the WHO recommendation for daily PA (Fig. 3).

Percentage of adolescents meeting daily FV intake (5 servings) in LMICs grouped by World Bank regions.

Percentage of adolescents meeting the daily PA recommendations in LMICs grouped by World Bank regions.
Differences in the outcomes of interest between adolescent boys and girls were observed in some but not all countries. In the sub-Saharan African region, only two countries (Senegal and Swaziland) showed girls more likely to meet the daily recommended intake of fruits compared to boys. Similarly, in two other countries (Seychelles and Tanzania) girls were more likely (p < 0.05) to meet the daily recommended intake of vegetables (Table 1
).
In the Middle East and North African region, a significant difference was observed in the daily intake of fruits among adolescent boys and girls in 50% of the countries examined. In four (Algeria, Djibouti, Morocco and Tunisia) out of the five countries, adolescent girls were more likely to meet the daily recommended servings of fruit as compared to boys. In Lebanon, however, adolescent girls were less likely to consume two servings of fruits daily compared to adolescent boys {OR = 0.74; 95%CI (0.63–0.88); p-value = 0.002} (Table 1).
With regards to daily servings of vegetables (≥3 per day), a statistically significant difference between adolescent girls and boys was seen in three countries in the Middle East and North Africa. In two of the three countries (Lebanon and Tunisia), adolescent girls were less likely to consume ≥3 servings of vegetables per day than boys. Nonetheless, in Morocco {OR = 1.28; 95%CI (1.07–1.53); p-value = 0.01}, girls were more likely to consume the daily recommended intake of vegetables compared to boys (Table 1). In six countries there were significant differences between adolescent girls and boys meeting the recommended five servings of FV daily. In four countries (Lebanon, Syria, Tunisia, and Yemen), adolescent girls were less likely to consume the daily recommended servings of FV compared to boys. However, in Algeria {OR = 1.23; 95%CI (1.03–1.48); p-value = 0.026} and Morocco {OR = 1.31; 95%CI (1.08–1.60); p-value = 0.01}, girls were more likely to have five or more servings of FV daily than boys (Table 2).
In the South Asian region, only the Maldives recorded a significant difference between adolescent boys and girls meeting the recommended daily intake of fruit. Specifically, girls were less likely to consume ≥2 servings of fruit or vegetables daily compared to boys. Girls in Pakistan were also less likely to consume the recommended servings of vegetables compared to boys (Tables 1 and 2).
In the Latin American and the Caribbean region, 29% of countries recorded differences (p < 0.05) between adolescent boys and girls in terms of FV intake, particularly in Costa Rica, Dominica, Jamaica, and Peru. More boys met the recommendations for daily fruit intake than the girls in Costa Rica, Dominica and Jamaica. Adolescent girls in Peru on the other hand, were more likely to meet the ≥2 servings of fruit {OR = 1.26; 95%CI (1.05–1.51); p-value = 0.014} than adolescent boys. In Argentina, girls were more likely to have ≥5 servings of FV daily compared to boys {OR = 1.43; 95%CI (1.02–2.00); p-value = 0.037} (Tables 1 and 2).
Lastly, in the East Asian and Pacific region, girls were less likely to meet the daily intake of vegetables compared to boys in Malaysia and Mongolia. Also, in Malaysia, girls were less likely to have ≥5 servings of FV daily {OR = 0.88; 95%CI (0.79–0.96); p-value = 0.007} compared to boys (Tables 1 and 2).
Regarding the daily WHO recommendations for daily PA, differences were observed between adolescent boys and girls in 50% of countries examined in the sub-Saharan African region. In all five countries (Benin, Mauritania, Senegal, Seychelles, and Tanzania), boys were more likely to meet the recommended daily PA guidelines compared to adolescent girls (Table 3).
In the Middle East and North African region, almost all the countries recorded a significant difference between boys and girls except for Yemen. In all the countries that showed a statistically significant difference, adolescent boys were more active and were more likely to meet the recommended daily PA guidelines than girls. Also, in the South Asian region, adolescent boys in the Maldives and Sri Lanka were more active than the girls (Table 3).
In the Latin American and the Caribbean region, adolescent boys were more likely to have 60 minutes of daily PA compared to girls, especially in Argentina, Belize, Bolivia, Costa Rica, Guatemala, Honduras, St. Vincent and the Grenadines, and Suriname. In the Former Yugoslav Republic of Macedonia, boys were more active than girls as the results showed boys as being more likely to have 60 minutes of daily PA {OR = 1.52; 95%CI (1.21–1.89); p-value = 0.001} compared to girls (Table 3).
Six of the eight countries (75%) in the East Asian and Pacific region recorded a significant difference between adolescent boys and girls in meeting the daily recommended PA. Five of the six countries (83%) showed that adolescent boys were more likely to have 60 minutes of daily PA for seven days compared to adolescent girls, especially in Fiji, Malaysia, Mongolia, Myanmar, and Thailand. However, in Tonga, adolescent boys were less active, rather the girls were more likely to have 60 minutes of daily PA for seven days {OR = 0.70; 95%CI (0.52–0.94); p-value = 0.018} compared to the boys (Table 3).
Discussion
This study found that adolescent boys and girls living in LMICs commonly do not meet WHO recommendations for FV intake and physical activity. In all countries, less than 50% of adolescents consumed five servings of FV daily. Morocco had the highest percentage of adolescents meeting the WHO recommendations for the daily intake of FV. According to the FAO20, the Moroccan diet is Mediterranean and it is based on a high consumption of FV. Similar findings with respect to the low daily intake of FV among adolescents, have been observed among adolescents in Ghana where 48% rarely ate fruits7 and in China where less than 50% ate fruit daily8. The variation could be due to differences in dietary cultural preferences among countries or regions as well as the availability of FV in the countries, income and urbanization rate6.
The results showed a clear, although variable trend in the FV intake between boys and girls, in which girls were more likely to reach the WHO recommendations. In the case of fruit, 58% of the countries where sex differences were noted showed that girls were more likely to consume ≥2 servings of fruit daily than adolescent boys. On the contrary, for vegetables, 67% of the countries that recorded a sex difference showed that boys were more likely to consume ≥3 servings of vegetables daily than girls. Rasmussen et al.10, reviewed FV intake in several countries and found that most studies (27 out of 49) showed gender differences in which girls had a higher intake of fruits and/or vegetables. Studies have attributed this gender difference to a preference for FV. It has also been reported that boys do not eat FV because they do not like them as much as girls do21,22. In addition to preference, Bere et al.21 found that the gender differences could also be attributed to the perceived accessibility of FV at home. They found that girls have a greater knowledge, and stronger intentions and self-efficacy compared to boys21. Lastly, according to Cooke et al.22, girls liked fruits and vegetables more than boys. The boys preferred energy-dense foods such as fatty and sugary foods to adapt to their higher energy requirement more so than girls.
According to the WHO2, the prevalence of physical inactivity is increasing among LMICs and it is already one of the leading causes of death. Among LMICs, India showed the highest proportion of adolescents who engaged in PA 60 minutes daily. The results from this study are consistent with those from Hallal et al.13, who found that 80.3% of adolescents between 13–15 years from 105 countries did not meet the recommended daily PA.
The results showed that physical inactivity was more common among adolescent girls in LMICs. In almost all the countries (30 out of 31), boys were more likely to meet the WHO recommendations for PA daily compared to girls. This result is consistent with studies showing that PA declines during adolescence, especially among girls11,12. A notable statistical difference between adolescent boys and girls with respect to PA was seen predominantly in the Middle East and North African region. These differences may be attributable to cultural and gender norms. Evidence from the Middle East and North Africa suggest that a barrier for women to engage in PA among women is the lack of facilities separated by gender, where women feel more comfortable being physically active23,24.
Despite its design and results, the study had a few limitations. The study included the use of the GSHS data, which surveys adolescents in schools. Thus the results might not necessarily reflect the FV consumption pattern and PA behavior among all adolescents in the respective countries. Specifically, information from adolescents who are unable to attend school or have dropped out would not be captured. Second, in some countries, FV are seasonal staples. Hence their consumption might be high or low in a country based on the season in which the data were collected. As stated earlier, PA patterns may also be affected by cultural perspectives resulting in the differences observed between countries and regions.
Third, adolescents had to recall and self-report their FV consumption and PA behavior during the past 30 days and week, respectively. This approach may result in either overestimating or underestimating intake behaviors, leading to information bias. Finally, we cannot be certain that the 5 servings reported by the adolescents were equivalent to 400 grams since we could not quantify the servings from the GSHS data.
Conclusion
The WHO recommendations for daily consumption of FV and PA were not consistently met in all countries. All the countries had less than 50% of their adolescents consuming ≥5 servings of FV daily. In general, the study found adolescent boys to be more active than girls, and this difference was more notable in the Middle East and North African region.
References
World Health Organization. Noncommunicable Diseases Progress Monitor, 2017. https://doi.org/10.2766/120051 (2017).
World Health Organization. Global Health Risks mortality and burden of disease attributable to selected major risks. (2009).
World Health Organization. Global status report on noncommunicable diseases 2010. (2011).
World Health Organization. Global recommendations on physical activity for health. (2010).
Joint WHO / FAO Expert Consultation. Diet, Nutrition and the Prevention of Chronic Diseases. WHO Technical Report Series. (2003).
Peltzer, K. & Pengpid, S. Fruits and vegetables consumption and associated factors among in-school adolescents in seven African countries. Int. J. Public Health 55, 669–678 (2010).
Doku, D., Koivusilta, L., Raisamo, S. & Rimpelä, A. Socio-economic differences in adolescents’ breakfast eating, fruit and vegetable consumption and physical activity in Ghana. Public Health Nutr. 16, 864–72 (2013).
Shi, Z., Lien, N., Kumar, B. N. & Holmboe-Ottesen, G. S. Socio-demographic differences in food habits and preferences of school adolescents in Jiangsu Province, China. Eur. J. Clin. Nutr. 59, 1439–1448 (2005).
Abudayya, A. H., Stigum, H., Shi, Z., Abed, Y. & Holmboe-Ottesen, G. Sociodemographic correlates of food habits among school adolescents (12–15 year) in North Gaza Strip. BMC Public Health 9, 185 (2009).
Rasmussen, M. et al. Determinants of fruit and vegetable consumption among children and adolescents: a review of the literature. Part I: Quantitative studies. Int. J. Behav. Nutr. Phys. Act. 3, 22 (2006).
Nader, P. R., Bradley, R. H., Houts, R. M., McRitchie, S. L. & O’Brien, M. N. Moderate-to-Vigorous Physical Activity From Ages 9 to 15 Years. Children 300, 295–305 (2008).
Troiano, R. P. et al. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 40, 181–188 (2008).
Hallal, P. C. et al. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 380, 247–257 (2012).
WHO. Health for the World’ s Adolescents A second chance in the second decade. www.who.int/adolescent/second-decade (2014).
World Bank. World Bank list of economies. http://librarians.acm.org/sites/default/files/wdi2013.pdf (2013).
Centers for Disease Control and Prevention. Global School-Based Health Survey. Available at: http://www.cdc.gov/gshs/pdf/GSHSOVerview.pdf.
Global School-Based Student Health Survey (GSHS) CORE QUESTIONNAIRE MODULES. Available at: http://www.who.int/chp/gshs/GSHS_Core_Modules_2009_English.pdf). (Accessed: 1st August 2016)
Centers for Disease Control and Prevention, W. H. O. Global Student Health Survey (GSHS) Data User’s Guide. 1–16 (2013). Available at: http://www.who.int/chp/gshs/methodology/en/index.html\nhttp://www.cdc.gov/gshs/questionnaire/index.htm.
SAS/STAT® User’s Guide, S. E. The MCMC Procedure. (2009).
Food and Agriculture Organization (FAO).Agricultural and Consumer Protection Department. Nutrition and consumer protection. Nutrition country profile – Morocco. Available at: http://www.fao.org/ag/agn/nutrition/mar_en.stm. (Accessed: 20th June 2008) (2010).
Bere, E., Brug, J. & Klepp, K.-I. Why do boys eat less fruit and vegetables than girls? Public Health Nutr. 11, 1–5 (2007).
Cooke, L. J. & Wardle, J. Age and gender differences in children’s food preferences. Br. J. Nutr. 93, 741–746 (2005).
Mabry, R. M., Winkler, E. A. H., Reeves, M. M., Eakin, E. G. & Owen, N. Correlates of Omani adults’ physical inactivity and sitting time. Public Health Nutr. 1–20 (2012).
Shuval, K. et al. The role of culture, environment, and religion in the promotion of physical activity among Arab Israelis. Prev. Chronic Dis. 5, A88 (2008).
Acknowledgements
We are grateful to the World Health Organization and the Centers for Disease Control and Prevention for making the GSHS data publicly available. Our sincere thanks go to the Country coordinators and the students who participated in the GSHS data collection.
Author information
Authors and Affiliations
Contributions
S.A.D.O. and D.S.G.T. formulated the research question, S.A.D.O., D.M.B., J.E.A. and D.S.G.T. designed the study, S.A.D.O. carried it out, S.A.D.O. analyzed the data and S.A.D.O., D.M.B., J.E.A. and D.S.G.T. wrote the article. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Darfour-Oduro, S.A., Buchner, D.M., Andrade, J.E. et al. A comparative study of fruit and vegetable consumption and physical activity among adolescents in 49 Low-and-Middle-Income Countries. Sci Rep 8, 1623 (2018). https://doi.org/10.1038/s41598-018-19956-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-19956-0
This article is cited by
-
Primary-school-aged children inspire their peers and families to eat more vegetables in the KiiDSAY project: a qualitative descriptive study
BMC Pediatrics (2024)
-
Consumption of fruits and vegetables among adolescents in Arab Countries: a systematic review
International Journal of Behavioral Nutrition and Physical Activity (2023)
-
Modelling health and economic impact of nutrition interventions: a systematic review
European Journal of Clinical Nutrition (2023)
-
Clustering of multiple health risk factors among a sample of adolescents in Liberia: a latent class analysis
Journal of Public Health (2022)
-
Consolidating evidence on the effectiveness of interventions promoting fruit and vegetable consumption: an umbrella review
International Journal of Behavioral Nutrition and Physical Activity (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
