
Abstract
Human papillomavirus is one of the most common sexually transmitted diseases worldwide. The natural history of oral HPV infection is unclear and its risk factors have not been explored. Immunocompromised individuals, as exemplified by HIV patients, are at high risk for HPV-related diseases. The mean of this study is to determine the prevalence ofHPV in the oral tract of HIV-1-positive male subjects and its association with risk factors. A total of 283 oral wash samples from HIV-1-positive men were tested. The oral fluid samples were used for DNA extraction and conventional PCR amplification; HPV genotyping was performed by hybridization. HPV genotyping revealed that nine samples (3.5%) were positive for HPV DNA; the major high-risk HPV types identified were 51 and 66. Worldwide studies have shown a variable prevalence of oral HPV. The diversity of genotypes and the high prevalence of multiple infections in HIV-infected subjects can be better explained by the effects of HIV-induced immunosuppression. The most important risk factors are unprotected sexual intercourse, but other factors for this infection have been described elsewhere including smoking, age and HIV-positive serostatus. In this study, smoking was the most important risk factor for acquiring oral HPV in HIV-1-infected subjects in Brazil.
Similar content being viewed by others

Introduction
Taxonomy
Human papillomavirus (HPV) is one of the most common agents of sexually transmitted diseases worlwide1. More than 180 HPV genotypes have been classified into different subgroups, with 40 types identified in the genital mucosa2,3.
Human papillomavirus infection
The natural history of genital HPV infection in men is difficult to evaluate because it depends on the anatomical site, sample, sampling methods and HPV DNA detection assays4. The highest prevalence of HPV infection in males is found in anogenital sites and in men who have sex with men (MSM). The presence of HPV infection has also been associated with the acquisition of HIV infection4.
Oral HPV infection
The oral HPV infection has not been explored5,6,7,8. The prevalence of oral HPV varies from 0 to 70% in normal oral mucosa, ranges from 0 to 85% in potentially malignant oral disorders and ranges from 0 to 100% in oral malignances. This variability is attributed to discrepancies such as sampling variation and limitations of the molecular techniques used in different studies9.
Risk factors and HPV
Exposure is determined by risk factors common to most sexually transmitted infections10. Little is known about the factors contributing to oral HPV infection. Several studies have shown that the number of life-time sexual partners, frequency of sex, oral sex or other intimate skin-to-skin contact increase the chance of being infected by HPV10,11. Additionally, other risk factors have been reported to affect disease development related to HPV infection, including smoking, alcohol use and immunodeficiency12,13,14.
Immunodeficiency and HPV infection
HIV infection increases susceptibility to opportunistic infections caused by viruses15,16. Thus, several studies have found an increased prevalence of HPV in individuals who are also HIV-infected17. Likewise, HIV infection can influence the natural history of HPV, by increasing the likelihood of a persistent infection and achieving greater virulence15.
To date, limited information is available regarding the natural history of oral HPV infectionand which risk factors are associated with it. Similarly, little is known about the association between HPV and HIV infections in men18. The aim of this study was to measure the prevalence of HPV in the oral tract of HIV-1-seropositive men and to evaluate major risk factors for transmission.
Methods
Study population
Two-hundred and eighty-three HIV-1-seropositive male patients referred to the HIV-Out Clinic ADEE3002, Dermatology Department of hospital das Clinicas, University of São Paulo medical school - HC-FMUSP and the Institute of Infectious Diseases “Emilio Ribas” from December 2011 to May 2013were included in the study. All patients appeared to have healthy oral mucosa. The mean age was 43.81 years (22–72 years). After signing an informed consent form, patients answered a questionnaire containing information on their social-behavioral characteristics. The study was approved by the respective ethical boards from the Institute of Tropical Medicine of São Paulo and the from Hospital das Clinicas of FMUSP.
Sample collection
Oral washes were performed as follows. Patients wereinstructed to performance oral rinse with 10 ml of sterile saline solution (0,9% sodium chloride – Baxter International) and the rinses were submitted to sample collection. After collection, samples went through a process of washing and centrifugation. They were then aliquoted and stored at −20°C for later analysis.
Precautions for contamination prevention
Strict procedures were followed to avoid false-positive reactions due to contamination. DNA extraction, reagent preparation and addition of sample DNA were carried out separately. Each area has its own dedicated equipment and every test included a negative control amplification containing distilled water without a DNA sample. All working surfaces were decontaminated with sodium hypochlorite and alcohol (70%), before and after use.
Laboratory methods
Samples were subjected to a DNA extraction process using a commercially available kit (Illustra Tissue and Cells GenomicPrep Mini Spin kit, Easton Turnpike, Fairfield, USA) and, run according the manufacturer's instructions. After this procedure, the DNA was stored at −80°C for later analysis.
Beta-globin PCR was performed for all samples as a control for DNA quality. The protocol used was previously standardized in the laboratory where the research was conducted. PCR was performed in a final reaction volume of 50 ul, containing 5 ul of template DNA, 10 × PCR buffer, 50 mM of MgCl2, 10 mM of dNTPs, 5 U/ml of Taq DNA polymerase and 10 pmol of each primer. The PCR conditions were as follows: pre-heated at 95°C for 4 minutes followed by 35 cycles of 1 minute at 94°C, 1 minute at 55°C and 1 minute at 72°C, with a final extension of 7 minutes at 72°C.
HPV detection was carried out with a conventional PCR using the primers MY09/11. The protocol used was previously standardized in the laboratory where the research was conducted. PCR was performed in a final reaction volume of 50 ul, containing 5 ul of template DNA, 0.05 U/ul of Taq DNA polymerase, 4 mM of MgCl2, 0.4 mM of each dNTP, of PCR Mastermix(Thermo Scientific/Walthan - MA) and a final concentration 4 pmol of the MY09/11 primers. The PCR conditions were as follows: preheatedat 95°C for four minutes followed by 40 cycles of 1 minute at 94°C, 1 minute at 55°C and 1 minute at 72°C, with a final extension of 7 minutes at 72°C. The presence of HPV DNA was confirmed using electrophoresis on a 2% agarose gel containing ethidium bromide.
Finally, a commercially available kit was used for HPV genotyping(PapillomaStrip High + Low Risk − Operon Immune & molecular diagnostics − Cuarte de Huerva/Zaragoza − Spain). PapillomaStrip is a test based on the reverse blot technique that allows the genotyping of DNA samples and is capable of detecting 18 human papillomavirus subtypes of low-risk (subtypes 6, 11, 40, 42, 43, 44, 54, 61, 62, 67, 70, 71, 72, 74, 81, 83, 84 and 91) and 19 human papillomavirus subtypes of medium-high risk (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 69, 73 and 82). The methods were carried out in accordance with the approved guidelines.
Statistical data analysis
Descriptive statistics were performed with the statistics program SPSS 20.0 and displayed in tables showing frequencies and percentages. The bivariate analysis was performed with the epidemiological statistics of open code for public health – OpenEpi 3.01 software withoral HPV as the dependent variable and age, smoking and alcohol use status, use of condom in sexual relations, practice of oral sex, HIV viral load, CD4 count and use of HAART, as independent variables. Variables attaining a p value lower than 0.05 on the bivariate analysis were entered in a multivariate logistic model in a forward stepwise fashion. The multivariate analysis was performed with the aid of Stata 12.0 statistical software(StataCorp. 4905 Lakeway Drive, College Station, TX).
Results
Laboratory data and behavioral characteristics of all 283 patients were analyzed. All patients in this study were male and HIV-infected (data not shown), 83% were using HAART, 82.3% had T CD4 cell counts ≥ 350 cell/mm3 and 78.8% had undetected HIV viral loads (less than 50 copies).
Most of the patients had a college degree (45.2%), were single (53.4%), of white ethnicity (60.8%) and did not use drugs (62.5%). We also evaluated alcohol intake and tobacco use: 54.8% ingested some alcohol and 30.4% were current smokers, 3.9% of the patients had smoked for months and 26.5% had smoked for years.
In regards to sexual exposure, 41% reported having had sex with men in the last year, 73.9% reported using a condom with a casual partner and 53.4% reported having engaged in active oral sex. Furthermore, 54.3% had passive oral sex and 52.6% had active anal sex. Approximately 75.4% had no discharge and 80.2% had no warts or wounds on the genital site.
HPV DNA was found in ten of the 283 samples (3.5%) (data not shown). The mean age of the HPV+ group was 42 years (26–56 years), 70% were using HAART, 80% had T CD4 cell counts ≥ 350 cells/mm3 and undetectable HIV viral loads. Most of the patients were single (80%), 50% had a college degree, most were of white ethnicity and did use drugs. Among these patients, 80% are smokers and 60% smoke more once a day (Table 1).
For sexual exposure, all of the HPV-positive patients reported having sex with men in the last year, with active anal sex and using a condom with casual partners, 80% had active oral sex, 40% had passive oral sex, 80% had no discharge or wounds and 90% had no warts at the genital site.
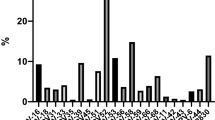
HPV DNA was genotyped, identify and classifythe subtypes in each sample (table 2). In the high-risk group, the most highly prevalent type was HPV-66 (60%) followedHPV-51 (40%). The HPV-58 type was found in three samples (30%) and the HPV-16, 56 and 69 types were each found once in different samples.
In the low-risk group, the HPV-6 and 83 types were found in two samples (20%) and the HPV- 44, 62, 67, 72 and 84 types were each found once in different samples. Three samples had multiple high-risk subtypes and two samples had multiple low-risk subtype.
Variables such as sexual exposure, alcohol consumption, cigarette smoking, HIV serostatus, HIV viral load, CD4 cell count and HAART use were assessed as possible risk factors for oral HPV (table 3). The bivariate analysis was performed comparing the distribution of factors between HIV-infected men HPV-HIV coinfected men.
The variables that had significant results based on a p value less than 0.05 were included in the multivariate logistic regression analysis to determine which factors are a risk for oral HPV infection (table 4). The only factor significantly associated the detection of HPV DNA was smoking [OR (CI) = 10.04 (1.98–50.92), p < 0.01].
Discussion
Worldwide studies have shown a variable prevalence of oral HPV in healthy individuals19. This variability may be due to factors such as the difference in the local mucosal immunity, saliva flow and immunoglobulins in the oral cavity, different methods of sample collection and analysis and propensity to micro trauma injuries20,21.
In HIV-infected subjects, oral HPV infection is more aggressive and more highly prevalent compared with a healthy population16,19,22. A comparative study including HIV-infected patients and healthy subjects foundthat 25.3% of HIV patients had an HPV infection in the oral tractcompared with 7.6% of healthy subjects23. In the United States, a study was conducted with 190 HIV-positive men and found that 6.3% them had detectable HPV in their oral fluid samples23. On the other hand, a study conducted in theUnited States and Spain with 166 patients showed a prevalence of 21% of oral HPV in HIV-positive MSM individuals, of which 11.1% were low-risk types and 66.6% were high-risk types24. In our study, oral HPV infection was detected in 3.5% of HIV-positive patients, in accordance withboth previous results and with the variability found in the prevalence of oral HPV in several studies9.
The diversity of genotypes and the high prevalence of multiple infections in HIV-positive subjects can be better explained by the effects of HIV-induced immunosuppression25. Our results demonstrate that most HPV-infected patients had more than one high-risk type.
When comparing the anogenital and oral genotypes, some types could be found at both sites. Regarding the low-risk groups, HPV-6 and 11 are the most prevalent26. In our study, HPV-6 was found in 20% of the samples. In the high-risk group, HPV-16 and 18 were the most prevalent at the anogenital site followed by HPV-31, 33, 39, 45, 51, 52, 53, 58, 59, 66 and 7327. In our study, several high-risk anogenital types were found, especially HPV-66.
The most important classical risk factors are unprotected sexual intercourse and multiple sexual partners20. Several studies have suggested that a high number of lifetime sexual partners and practices such as kissing, oral-penile sex and hand warts are predictive of oral HPV infection20,28.
Other factors for this infection have been described elsewhere, including smoking and HIV-positive serostatus20. Although some studies indicate that there is conflicting evidence on the relationship between cigarette smoking and HPV infection, several studies suggested that recent cigarette smoking was associated with a significantly increased risk of oral HPV29,30. According to Read and coworkers14, smoking causes oral epithelial thickening, periodontal disease and epithelial abrasion, thereby increasing the risk of HPV infection.
In this report, we examined the oral tract as a site associated with the presence of HPV infection. After controlling for potential confounding variables, the only risk factor remaining significantly associated with HPV infection in our patients was cigarette smoking (p < 0.001).
Studies suggest that HIV-infected individuals may have a higher risk of developing oropharyngeal cancer as well other HPV-associated cancers31,32,33. Some studies, indicate that highly active therapy (HAART) does not reduce the prevalence of oral HPV and that CD4 cell count increases the incidence, progression and persistence of HPV-induced lesion16,34.
In our study, there was no substantial difference between these factors, because the majority of our patients had undetectable HIV viral loads and their CD4 cell counts were greater than 350 cells/mm3.
We could not determine whether HPV in the oral cavity of our patients had caused any related disease, such as head and neck squamous cell carcinoma (SCCHN) associated with cigarette smoking. However, it is known that these HPV oral carriers are potential transmitters of the virus.
Finally, it is important to acknowledge that most HPV types found in our patients are high-risk types but that, those types are unfortunately not treated by the currently available marketed vaccines. As a highlight, more studies are needed to enable a better understanding of the association between oral HPV infection and its risk factors in HIV-positive people.
References
Reis, A. A. S. et al. Infecção viral e os estudos moleculares dos carcinomas associados ao papilomavírus humano. News Lab. 92, 100–108 (2009).
Zur Hausen, H. Papillomaviruses in the causation of human cancers-a brief historical account. Virol. 384, 260–265 (2009).
Muñoz, N. Epidemiological classification of human papillomavirus types associates with cervical cancer. New Engl J Med. 348, 518–527 (2003).
Esquenazi, D. et al. The frequency of human papillomavirus findings in normal oral mucosa of healthy people by PCR. Braz J Otorhinolaryngol. 76, 78–84 (2010).
Seifi, S. et al. Prevalence of Oral Human Papilloma Virus in Healthy Individuals in East Azerbaijan Province of Iran. Iranian J Publ Health. 42, 79–85 (2013).
Nureña, C. R. et al. HPV and genital warts among Peruvian men who have sex with men and transgenders people: knowledge, attitudes and treatment experiences. Plos One. 8, e58684 (2013).
Videla, S. et al. Natural history of Human Papillomavirus Infections involving anal, penile and oral sites among HIV-infected men. Sex Transm Dis. 40, 3–10 (2013).
Franceschi, S. et al. Human Papillomavirus and cancers of the upper aerodigestive tract: a review of epidemiological and experimental evidence. Cancer Epidemiol Biomarkers Prev. 5, 567–575 (1996).
Feller, L. et al. Epithelial maturation and molecular biology of oral HPV. Infec Agents and Cancer. 4, 01–09 (2009).
Alves, D. B. et al. Linfócitos CD4, CD8 e células NK no estroma da cérvice uterina de mulheres infectadas pelo papilomavírus humano. Ver Soc Bras Med Trop. 43, 425–429 (2010).
Stanley, M. HPV – Immune Response to Infection and Vaccination. Infec Agents and Cancer. 5, 1–6 (2010).
Gonçalves, M. A. et al. Immune cellular response to HPV: Current concepts. BJID. 8, 1–9 (2004).
Ciarra, G. et al. Critical Role of the Rb Family in Myoblast survival a fusion. Plos One. 6, e17682 (2011).
Smith McCune, K. K. et al. Type-Specific Cervico- vaginal Human Papillomavirus Infection Increases Risk of HIV Acquisition Independent of other sexually transmitted Infection. Plos One. 5, e10094 (2010).
Kreuter, A. et al. Human papillomavirus-associated induction of human beta-defensins in anal intraepithelial neoplasia. Br J Dermatol. 160, 1197–205 (2009).
Low, A. J. et al. Genital warts infection with human immunodeficiency virus in high-risk women in Burkina Faso: a longitudinal study. BMC Infec Dis. 11, 20 (2011).
Figlioulo, G. et al. Clinical and laboratorial study of HPV infection in men infected with HIV. Int Braz J Virol. 38, 411–8 (2012).
Baay, M. et al. HPV in cervix and vagina. Sex Transm Infect. 80, 249–250 (2004).
Amornthatree, K. et al. Impacts of HIV infection and long-term use of antiretroviral therapy and the prevalence of oral human papillomavirus type 16. J Oral Pathol Med. 41, 309–314 (2012).
Read, T. R. H. et al. Oral Human Papillomavirus in men having sex with men: Risk-factors and sampling. Plos One. 7, e49324 (2012).
Hagensee, M. E. et al. Human papillomavirus infection and disease in HIV-infected individuals. Am J Med Sci. 328, 57–63 (2004).
Stuardo, V. et al. Human Papillomavirus Infection in HIV-1 infected women in Catalonia (Spain): Implications for prevention of cervical cancer. Plos One. 7, e47755 (2012).
Vargas, L. O. S. et al. Detection of Human papillomavirus (HPV) in oral mucosa of women with cervical lesions and their relation to oral sex practices. Infect Agents Cancer. 5, 25 (2010).
McLemore, M. S. et al. Head and neck squamous cell carcinoma in HIV-positive patients: a preliminary investigation of viral associations. Head and Neck Pathol. 4, 97–105 (2010).
Hansson, B. G. et al. Strong Association between infection with Human Papillomavirus and oral and oropharyngeal squamous cell carcinoma: A population-based case-control study in Southern Sweden. Acta Otolaryngol. 125, 1334–1337 (2005).
Danielewski, J. A. et al. Human Papillomavirus type 6 and 11 genetic variants found in 71 oral and anogenital epithelial sample from Australia. Plos One. 8, e63892 (2013).
Darnel, A. D. et al. Correlation between the presence of High-risk human papillomaviruses and ID gene expression in Syrian women with cervical cancer. Clin Microbiol Infect. 16, 262–266 (2010).
Schuwartz, S. M. et al. Oral cancer risk in relation to sexual history and evidence of human papillomavirus infection. J Natl Cancer Inst. 90, 1626–1636 (1998).
Rangin, C. et al. Oral HPV Infection and sexuality: A cross-sectional study in woman. Int J Mol Sci. 12, 3928–3940 (2011).
Herrero, R. et al. IARC Multicenter Oral Cancer Study Group. Human Papillomavirus and oral cancer: International Agency of Research on Cancer Multicenter study. J Natl Cancer Inst. 95, 1772–1783 (2003).
IARC. International Agency for Research on Cancer. Human Papillomaviruses. Monogr Eval Carcinog Risk Human. 90, 1–670 (2007).
De Pyeon, S. M. et al. Establishment of human papillomavirus infection requires cell cycle progression. Plos Pathogens. 5, e1000318 (2009).
Dunne, E. F. et al. Prevalence of HPV infection among men: a systematic review of the literature. J Infect Dis. 194, 1044–1057 (2006).
Anic, G. M. et al. Genital HPV infection and related lesions in men. Prev Med. 53, 536–541 (2011).
Acknowledgements
Fapesp 2010/07076-4; 2011/16094-9. We thank Dr. Jose Vidal and Dr. Margareth Eira for patient referralsfrom the Emilio Ribas Institute and Dr. Ana Paula R. Veiga, Lucas Medeiros, Mauricio Ferreira, Arthur Paiva for patients from ADEE/HCFMUSP. We also thank Eduardo Martins and Noemia Orii for technical support.
Author information
Authors and Affiliations
Contributions
K.G., L.A.F.M. and J.C. wrote the main manuscript text; O.L., L.A.F.M. and K.G. performed the statistical analysis; T.A., F.C. and A.S.F. prepared tables 1–4 and A.J.S.D. helped with the discussion. All authors reviewed the manuscript and approved the final version.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article's Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder in order to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Gaester, K., Fonseca, L., Luiz, O. et al. Human papillomavirus infection in oral fluids of HIV-1-positive men:prevalence and risk factors. Sci Rep 4, 6592 (2014). https://doi.org/10.1038/srep06592
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep06592
This article is cited by
-
Sexual practices and HPV infection in unvaccinated young adults
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
