
Abstract
Study design:
Retrospective population-based cohort study.
Objectives:
To provide national data on epidemiology of traumatic spinal cord injury (TSCI) among the population of Estonia from 1997 to 2007.
Setting:
All Estonian hospitals.
Methods:
Medical records of patients with TSCI from all regional, central, general and rehabilitation hospitals in Estonia were retrospectively reviewed. Epidemiological characteristics, etiology, neurological level and severity of injury, concomitant injuries were analyzed.
Results:
A total of 595 patients with TSCI from 1 January 1997 to 31 December 2007 were identified. The male to female ratio was 5.5:1. The mean age at injury was 39.0 years. The crude incidence rate was 39.7 (95% confidence interval: 36.6–43.0) per million population. The most frequent cause of TSCI was falls (41%), followed by traffic accidents (29%). Alcohol consumption preceded 43% of injuries. The lesion level was cervical in 59.4%, thoracic in 18.3% and lumbar/sacral in 22.3%.
Conclusion:
Compared to recent studies from Europe, where the incidence of TSCI is between 15 and 30 per million population, the incidence of TSCI in Estonia is among the highest. The rates are significantly higher in men compared with women and especially among the youngest men. The leading cause of TSCI is falls. A significant proportion of injuries are related to alcohol consumption before trauma in Estonia.
Similar content being viewed by others


Introduction
Traumatic spinal cord injury (TSCI) may cause long-term disability, which has a significant impact on quality of life and survival. The incidence rates differ markedly between countries and it has also been found that the causes are dissimilar.1, 2
Estonia covers an area of 45 227 km2 and is situated in the northeastern part of Europe. Estonia is a member of European Union since 2004 with its population of 1.34 million. The Estonian population is ageing rapidly and one cause is the high mortality because of injury among the young.3
Considering that mortality due to injuries is several times higher in Estonia than in most European countries, the incidence of TSCI should also be high. The aim of the study was to determine the incidence, cause, circumstances of TSCI and sociodemographic characteristics of TSCI victims in Estonia to plan prevention strategies.
Materials and Methods
The study design was retrospective and included all TSCI cases in Estonia between 1 January 1997 and 31 December 2007.
Several overlapping methods of case ascertainment were used to minimize the possible missing cases. There are no spinal cord units established in Estonia. As a rule, most patients with TSCI in Estonia are acutely admitted to the Departments of Neurosurgery of the North Estonia Medical Centre or Tartu University Hospital where the patients are evaluated and treated neurosurgically, if needed. At first, all medical records of the patients with possible TSCI diagnosis were retrospectively reviewed. The patients who are medically stable and neurosurgical management is not indicated are treated in central or general hospitals. For this purpose, all medical records of the patients with the TSCI diagnoses or suspected TSCI were also looked through in all Estonian rehabilitation hospitals, in central and general hospitals. As a whole, medical records from 22 Estonian hospitals (3 regional, 3 rehabilitation, 4 central and 12 general hospitals) were reviewed and all the cases of TSCI were registered.
We selected the cases under the International Classification of Disease-10 diagnosis codes suggesting TSCI (Table 1). Medical records with diagnosis codes suggesting spinal fractures were also reviewed in order not to lose cases.
The inclusion criteria were as follows: (1) traumatic spinal cord or cauda equina injury with neurological deficit found at discharge, (2) permanent resident of Estonia at the time of injury. The patients with only transient neurological symptoms (varying degrees of motor or sensory deficit) that lasted <7 days, and/or pain, or non-traumatic injury, were excluded. The fatal cases before hospitalization were not included.
Demographic data, length of admission, level of injury, extent of injury according to the American Spinal Injury Association Impairment Scale (AIS), cause of injury and alcohol consumption associated with trauma and the presence of spinal fracture were recorded.4 The causes of TSCI were divided into six groups (sports and leisure activities, assaults, transport activities, falls, other traumatic causes, unknown), as suggested by the Executive Committee for the International Spinal Cord Injury Data Sets Committees'.5
Severity of injury was reported by four categories according to the recent recommendations by the Executive Committee for the Development of the International Spinal Cord Injury Data Sets: C1-4 AIS A, B or C; C5-8 AIS A, B or C; T1-S5 AIS A, B or C; and AIS D at any injury level. Because of the small number of ventilator-dependent patients, they were analyzed together with the C1-4 AIS A, B, C patients.6
Alcohol consumption prior to a TSCI was registered when on admittance to the hospital signs of alcohol were detected in the blood or when alcohol consumption before trauma was recorded in medical documents.
Descriptive data were presented as percent, mean, median and standard deviation. For categorical data, frequencies and percentages were expressed in contingency tables and differences were assessed by the χ2-test. The incidence rates with 95% confidence intervals were calculated using Poisson distribution. The crude incidence rates were calculated using the mid-year population census for each year and were age- and gender-adjusted by direct standardization to Estonian population (census 2000).
Trends in incidence were calculated using the Poisson regression model. A quasi-Poisson model was used when overdispersion was present. Age (8 categories) and sex (2 categories)-specific incidence rates were calculated over time (11 categories).
The analysis of temporal trends was based on χ2-test for categorical data and one-way analysis of variance for continuous data.
A statistical level of significance of 5% was used (P<0.05), all confidence intervals (CIs) were expressed at 95% (95% CI).
The study was approved by the Research Ethics Committee of the University of Tartu, Estonia.
Results
Gender and age
The medical records of more than 3000 patients from 22 Estonian hospitals were retrospectively reviewed, of them 595 met the inclusion criteria of TSCI. The majority of patients were men (84.5%; Table 2). The male to female ratio was 5.5:1.
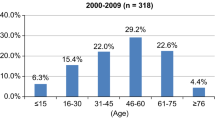
The mean age at injury was 39.0 years and it remained stable during the whole study period (P=0.3). The proportion of patients older than 60 years at injury was 15.0%. The youngest TSCI victim was 1 year old and the oldest was 93 years old.
Incidence
The annual crude incidence rate was 39.7 per million population (95% CI: 36.6–43.0) for all. After standardization to the Estonian population by age and gender, the annual incidence rate was 39.4 (95% CI: 36.2–42.6) for all, 72.0 (95% CI: 65.7–78.3) for men and 11.5 (95% CI: 9.2–13.9) for women.
There was no statistically significant change in the number of TSCI cases during the study period. The crude rate increased, but this was not statistically significant (incidence rate ratio 1.03, 95% CI: 1.00–1.05, P=0.051). After the adjustment by age and gender, the trend remained statistically nonsignificant (incidence rate ratio 1.02, 95% CI: 1.00–1.05, P=0.09). However, there was a statistically significantly (incidence rate ratio 1.06, 95% CI: 1.02–1.10, P=0.003) increasing trend from 1999 to 2007 (Figure 1).

Age-adjusted incidence rates of traumatic spinal cord injury (per 1 000 000 annually) with 95% confidence intervals in Estonia from 1997 to 2007.
The incidence was significantly higher among men compared with that of women in all age groups (incidence rate ratio 6.4, 95% CI: 5.1–8.1; Table 3).
International comparison
Recent studies from European countries have reported the incidence rate of TSCI 10.4 per million inhabitants in the Netherlands7 to 26.3 in Norway,8 with the median for the Western Europe 14.4 per million.9 The worldwide incidences of TSCI vary widely from 10.4 to 83 per million.1 In Estonia, the incidence rate of TSCI is among the highest rates in Europe and close to these from North America (Figure 2).9

Crude incidence rates of traumatic spinal cord injury per 1 000 000 globally.9 *Cases aged 15 years and older. **Cases aged 16 years and older. ***Prehospital mortalities included.
Causes of TSCI
The most common cause of TSCI was falls (41.0%), followed by traffic accidents (29.4%; Figure 3). Falls was significantly more common reason of TSCI in patients ⩾30 years, accounting for 51.5% of TSCI cases compared with 24.4% in those <30 years (P<0.001). The highest proportion of falls as a cause of TSCI was among patients ⩾60 years (72.4%). Traffic accidents were the most common cause among patients <30 years (P<0.001).

Number of traumatic spinal cord injury cases by cause in Estonia, 1997–2007.
Diving was the leading cause of sports injuries (91.4%). Among other injuries 31.0% occurred as a result of traumatic blows on tree felling.
Alcohol consumption preceded TSCI in 257 of cases (43.2%), whereas in 34.2% of cases alcohol consumption was unknown or not recorded in the medical documents. Significantly more men than women (46.0 vs 34.7%) had signs of alcohol consumption on admission to the hospital. Almost half of patients injured at diving had consumed alcohol (52.7%). There was no change in alcohol consumption preceding trauma from 1997 to 2007 (P=0.1).
The trauma was work-related in 15.2% of cases. The main external cause was falls (39.1%), followed by accidental tree felling (31.0%).
Level and extent of TSCI
The cervical part of spinal cord was the most common site of injury. The injury was at cervical level in 59.4%, at thoracic level in 18.3% and at lumbar or sacral level in 22.3%. Patients ⩾60 years had cervical SCI in 80% of cases. Table 2 presents the distribution of cases according to recently recommended guidelines.6 In 53% of cases the injury was motor complete (AIS: A and B) and in 47% of cases it was motor incomplete (AIS: C and D).
Spinal column fractures occurred in 76.3% of cases. Spinal column fractures were significantly associated with the severity of injury (P<0.001). The most common spine injury occurred at C5 (17.0%), C6 (13.0%) level and L1 (13.4%) level. In 31.6% of cases there was an associated injury, the most frequent was brain injury (30.6%).
Discussion
The present study shows high incidence of spinal cord injuries in Estonia.
Previous studies have been mostly hospital based7, 10 or limited to adult population.11 To our knowledge, our study is the first population-based study that included all age groups from all hospitals of the whole country.
The crude incidence of TSCI was 39.7 per million in Estonia from 1997 to 2007, which is one of the highest in Europe. Only the Portugal study, which included prehospital mortalities reported higher incidence rate.12
There was an increasing trend in incidence from 1999 to 2007. The possible explanation is that the prevention of TSCI has been ineffective in Estonia. Another explanation may be that we have missed some cases during the first study years. However, the incidence rates were fluctuating in the beginning of the period (Figure 1), and some other studies have reported an increasing trend in the TSCI incidence rates, too.8 No clear explanation for this phenomenon has been given yet.
Consistent with previous studies,1, 2, 13 men were more prone to TSCI in all age groups in Estonia. There is no clear explanation why men are at greater risk for TSCI. It has been suggested that women perform risky activities more cautiously than men and therefore may be exposed to lower risk of injury. An international comparative study from 19 European countries found that women drive safer than men.14 This study also showed that men below 55 have the most dangerous driving behavior.
Many developed countries have reported the bimodal distribution of TSCI incidence rates with the second peak after the age of 60 years.10, 15 This has been explained by the fact that the mean age at the time of injury is increasing because population is aging. The percentage of people older than 65 years is even higher in Estonia than the European region average.16 However, our data did not reveal this bimodal distribution. The incidence was very high in the age group of 20–29 years in Estonia and declined substantially with increasing age becoming similar to other European countries.
In the Baltic states the majority of the population engage in sedentary activities during leisure time.17 It is expected that leisure-time inactivity increases with age. We speculate that elderly in Estonia are less healthy and functionally not so active and do not get into the situations where they can fall. Another hypothesis is that the elderly in Estonia are prone to very severe falls and possibly they die before reaching the hospital. Mortality in the elderly group is higher within the acute phase of TSCI.18 It has also been shown that unhealthy lifestyle and inactivity increase the rate of mortality.19 As stated before, mortality due to injuries is many times higher in Estonia than in most European countries.6 Considering that, TSCI as a cause of death would also be high. Our further study will address the reasons of prehospital death of TSCI in Estonia.
Although fall was the main reason for TSCI in Estonia, persons between 20 and 29 years of age are most often injured in traffic accidents and diving. We also found that most of the sport injuries were caused by diving (12.4% of all cases). Consistent with a previous report,16 young healthy men in their early twenties are usually the victims of diving accidents. In our study, falls became the most prevalent cause of TSCI among persons older than 29 years.
Alcohol consumption is high in Estonia and alcohol abuse before TSCI was recorded in almost half of the cases in our study. Since 2005, the state alcohol policy has become more strict in Estonia and alcohol consumption has decreased since 2008.20 Our study included the cases until 31 December 2007 and there was no statistically significant decrease in alcohol consumption preceding trauma. Alcohol abuse is a clear risk factor for TSCI. There is a need for more effective preventive measures concerning alcohol.
Falls was the most prevalent external cause of TSCI occurring in the workplace, followed by blows to the vertebral spine. It shows that our workers as well as employers should be better educated on safety.
The strength of the study was that we included the whole Estonian population to the study. Several overlapping sources of information were reviewed to minimize errors and missing cases. Medical records were reviewed even in smallest local hospitals where patients with TSCI are usually not treated. Thus, we probably missed no cases.
The study had some limitations. First, we did not include the patients who died before the arrival to hospital. Only three studies have included the fatal cases before hospitalization so far and have presented higher incidence rates than other studies.1 The study of prehospital mortality is currently in progress in Estonia. Second, we identified the TSCI patients by diagnostic codes only. However, the list of International Classification of Disease-10 codes suggesting a TSCI was widened by spinal fractures at every level in order to catch up more cases. Third, as the study was performed with retrospective design the available information was probably limited. In order to show the trends of TSCI, a prospective register providing full coverage of the population in Estonia is necessary.
Taking into consideration that TSCI incapacitates higher proportion of inhabitants than in other European countries, preventive measures should be more efficacious. Special target should be the younger age groups, especially men.
Data archiving
There were no data to deposit.
References
Wyndaele M, Wyndaele JJ . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Chiu WT, Lin HC, Lam C, Chu SF, Chiang YH, Tsai SH . Review paper: epidemiology of traumatic spinal cord injury: comparisons between developed and developing countries. Asia Pac J Public Health 2010; 22: 9–18.
Lai T, Köhler K, Rooväli L . Injuries in Estonia. Ministry of Social Affairs of Estonia, Health Information and Analysis Department: Tallinn. 2009 p 15 Available at: http://www.sm.ee/fileadmin/meedia/Dokumendid/V2ljaanded/Toimetised/2009/series_20095eng.pdf.
Maynard FM, Bracken MB, Creasey G, Ditunno JF, Donovan WH, Ducker TB et al. International standards for neurological and functional classification of spinal cord injury. Spinal Cord 1997; 35: 266–274.
DeVivo MJ, Biering-Sorensen F, Charlifue S, Noonan V, Post M, Stripling T et al. International Spinal Cord Injury Core Data Set. Spinal Cord 2006; 44: 535–540.
DeVivo MJ, Biering-Sorensen F, New P, Chen Y . Standardization of data analysis and reporting of results from the International Spinal Cord Injury Core Data Set. Spinal Cord 2011; 49: 596–599.
van Asbeck FW, Post MW, Pangalila RF . An epidemiological description of spinal cord injuries in The Netherlands in 1994. Spinal Cord 2000; 38: 420–424.
Hagen EM, Eide GE, Rekand T, Gilhus NE, Gronning MA . 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord 2010; 48: 313–318.
Cripps RA, Lee BB, Wing P, Weerts E, Mackay J, Brown D . A global map for traumatic spinal cord injury epidemiology: towards a living data repository for injury prevention. Spinal Cord 2011; 49: 493–501.
Berg MV, Castellote JM, Mahillo-Fernandez I, de Pedro-Cuesta J . Incidence of traumatic spinal cord injury in Aragón, Spain (1972–2008). J Neurotrauma 2011; 28: 469–477.
Ahoniemi E, Alaranta H, Hokkinen EM, Valtonen K, Kautiainen H . Incidence of traumatic spinal cord injuries in Finland over a 30-year period. Spinal Cord 2008; 46: 781–784.
Martins F, Freitas F, Martins L, Dartigues JF, Barat M . Spinal cord injuries—epidemiology in Portugal's central region. Spinal Cord 1998; 36: 574–578.
Ackery A, Tator C, Krassioukov A . A global perspective on spinal cord injury epidemiology. J Neurotrauma 2004; 21: 1355–1370.
Golias I, Karlaftis MG . An international comparative study of self-reported driver behavior. Transp Res Part F Traffic Psychol Behav 2002; 4: 243–256.
Dryden DM, Saunders LD, Rowe BH, May LA, Yiannakoulias N, Svenson LW et al. The epidemiology of traumatic spinal cord injury in Alberta, Canada. Can J Neurol Sci 2003; 30: 113–121.
European Union.. Europe in figures: Eurostat yearbook 2010. Office for Official Publications of the European Union: Luxembourg. 2010 pp 149–203.
Pomerleau J, McKee M, Robertson A, Vaasc S, Kadziauskiene K, Abaravicius A et al. Physical inactivity in the Baltic countries. Prev Med. 2000; 31: 665–672.
Furlan JC, Bracken MB, Fehlings MG . Is age a key determinant of mortality and neurological outcome after acute traumatic spinal cord injury? Neurobiol Aging 2010; 31: 434–446.
de Groot LC, Verheijden MW, de Henauw S, Schroll M, van Staveren WA . SENECA Investigators. Lifestyle, nutritional status, health, and mortality in elderly people across Europe: a review of the longitudinal results of the SENECA study. J Gerontol A Biol Sci Med Sci 2004; 59: 1277–1284.
Lai T, Habicht J . Decline in alcohol consumption in Estonia: combined effects of strengthened alcohol policy and economic downturn. Alcohol Alcohol 2011; 46: 200–203.
Acknowledgements
The study was supported by the Estonian Science Foundation grant no. 7868 and the targeted financing no. SF0180064s07. We thank the medical staff of all Estonian hospitals for their kind help in the study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Sabre, L., Pedai, G., Rekand, T. et al. High incidence of traumatic spinal cord injury in Estonia. Spinal Cord 50, 755–759 (2012). https://doi.org/10.1038/sc.2012.54
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2012.54
Keywords
This article is cited by
-
Spinal cord injury: molecular mechanisms and therapeutic interventions
Signal Transduction and Targeted Therapy (2023)
-
A systematic review and meta-analysis of the global epidemiology of pediatric traumatic spinal cord injuries
European Journal of Pediatrics (2023)
-
Reliability and minimal detectable change of the Trunk Assessment Scale for Spinal Cord Injury (TASS) and the trunk control test for individuals with spinal cord injury
Spinal Cord Series and Cases (2022)
-
Current status of traumatic spinal cord injury caused by traffic accident in Northern China
Scientific Reports (2022)
-
Epidemiology of traumatic spinal cord injury in Finland
Spinal Cord (2021)
