
Abstract
To assess association between migraines and development of ocular motor cranial nerve palsy (CNP) and finding risk factors using the National Sample Cohort database from the Korea National Health Insurance Service. Data was analyzed from 4,234,341 medical screening examinees aged 20–90 years in 2009. Cox proportional hazard regression analysis was used to the adjusted hazard ratios (HR) for ocular motor CNP according to presence of migraine. Subgroup analysis was performed to evaluate effect of other factors on association of migraine with ocular motor CNP. A total of 5806 participants (0.14% of subjects) developed ocular motor CNP and were assigned to CNP group, 4,048,018 were assigned to control group, with an average of 8.22 ± 0.93 years of follow-up. Incidence of ocular motor CNP increased in migraine group compared to control. After adjusting potential confounding variables, HR for ocular motor CNP was 1.166 (confidence interval [CI] 1.013–1.343) in migraine group. Subgroups of relatively younger age less than 65 years (HR = 1.267, 95% CI 1.067–1.504), male gender (HR = 1.228, 95% CI 1.000–1.122), smokers (HR 1.426, 95% CI 1.127–1.803), and diabetes mellitus patients (HR = 1.378, 95% CI 1.045–1.378) showed a stronger association between migraines and development of ocular motor CNP. Our population-based cohort study demonstrated a significant association between presence of migraines and incidence of ocular motor CNP. Especially, relatively younger age, males, smokers, and diabetes patients with migraines could have a higher risk of developing ocular motor CNP.
Similar content being viewed by others

Introduction
The 3rd, 4th, and 6th cranial nerve palsies (CNP), which involve ocular muscles and lead to disabling symptoms including diplopia with or without abnormal head posture, are commonly encountered disease entities in neuro-ophthalmology practice1,2,3,4,5,6,7,8. The incidence of these diseases increases with age, and many previous reports revealed that ocular motor CNP had a close association with vasculopathic risk factors such as diabetes mellitus, hyperlipidemia, hypertension, and several diseases of the circulatory system, suggesting microvascular ischemia as the main etiology of ocular motor CNP, especially in elderly patients9,10,11. However, other conditions such as neoplasms, inflammation, infections, giant cell arteritis, trauma, and brainstem infarction were also reported as causes for ocular motor CNP development1,3,4,5,12,13,14,15,16,17,18,19,20, suggesting that heterogeneous mechanisms might be involved in the development of ocular motor CNP.
Migraine, a very common neurobiological headache disorder, is reported as one of the potential risk factors for ocular motor CNP development in one previous study21. In the previous study, a migraine diagnosis was associated with increased risks of developing subsequent, isolated 3rd, 4th, and 6th CNP compared to non-headache matched controls after a mean follow-up of 3.1 years21. However there was no mention of which factors increased the risk of ocular motor CNP in migraine patients.
The purpose of this study was to investigate the association between the presence of migraines and ocular motor CNP in the Korean adult population during long-term follow-up period using the National Sample Cohort (NSC) database from the Korea's National Health Insurance Service (NHIS) and identify other factors affecting the association between the risk of ocular motor CNP development and the presence of migraines. Registering in the NHIS has been mandatory for all citizens of Korea since 198922. The NHIS in Korea offers a biennial national health screening program (NHSP) for all beneficiaries aged ≥ 20 years, and especially, all citizens aged 40 years or older are strongly recommended to undergo biennial general health screening23. The participation rate in the general health screening program among eligible participants was 74.8% in 201424.
Materials and methods
Data sources and study population
In this nationwide, population-based, observational, retrospective cohort study, we utilized medical records from the Korea’s NHIS, a nationwide insurer that covers almost 97% of the entire Korean population. This mandatory, universal program offers comprehensive medical coverage including outpatient and inpatient services, emergency medicine, and prescription drugs for all Korean citizens. The NHIS manages and releases data to the public containing demographic factors, records of medical facility use, and diagnostic codes from the Korean Standard Classification of Diseases (KCD)-7 codes (7th Revision). In the KCD-7, diseases are classified according to the International Classification of Diseases-10 (10th Revision) system. The NHIS also provides a biennial health screening program to people aged ≥ 20 years, which collects past medical history and laboratory test results.
In this study, we analyzed the data from 4,234,341 medical screening examinees aged between 20 to 90 years in 2009. The study participants were followed up until December 31, 2018. After excluding (1) those who have been previously diagnosed with ocular motor CNP (n = 2873), (2) those with missing data (n = 166,941), and (3) those who were newly diagnosed with CNP or died within one year of testing (n = 10,703), we finally picked 4,053,824 eligible individuals. The reason we set the 1-year time lag was to avoid a situation where the causal relationship was reversed.
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Samsung Medical Center (IRB; IRB no. SMC 2020-09-050). The requirement for informed consent from the individual patients was waived from the Institutional Review Board of Samsung Medical Center (IRB; IRB no. SMC 2020-09-050) owing to the retrospective nature of the study and because the data used were public and anonymized under confidentiality guidelines.
Definition of ocular motor CNP, migraine, and confounders
Ocular motor CNP was identified based on the ICD-10 codes H49.0 (CN3), H49.1 (CN4), or H49.2 (CN6), and codes H06.2 (dysthyroid exophthalmos), E05 (thyrotoxicosis), or G70.0 (myasthenia gravis) were excluded. Migraine was diagnosed based on the ICD-10 codes of G43 for migraine and G431 for migraine with aura. We considered the variables including age, sex, smoking status, drinking amount, physical activity frequency, income status, and body mass index (BMI) as confounders in the relationship between ocular motor CNP and migraines. A standardized self-reported questionnaire was used to gather general health behaviors and lifestyles. The smoking status of the subjects was used to classify them as non-smokers, ex-smokers, or current smokers. The subjects were classified as non-drinkers, mild-to-moderate drinkers, and heavy drinkers according to the amount of alcohol consumed at once. Individuals who consumed more than 30 g of alcohol per day were defined as heavy drinkers. Regular physical activity was defined as doing high-intensity exercise for at least 20 min three times per week or at least 30 min of moderate-intensity exercise five times per week. The low-income level was defined as the bottom 20% of the total population. During the medical examination, height (cm) and weight (kg) were measured using an electronic scale at a medical facility. BMI was calculated as weight (kg) divided by height (m) squared. We also adjusted for the comorbidities of hypertension, diabetes mellitus, and dyslipidemia based on the following criteria. Hypertension was defined as a blood pressure (BP) of ≥ 140/90 mmHg, or a prescription at least once per year for antihypertensive drugs under ICD-10-CM codes I10–I13 or I15. Diabetes mellitus (DM) was defined as a fasting glucose of ≥ 126 mg/dL, or a prescription of one or more antidiabetic drugs at least once per year. Dyslipidemia was defined as a total cholesterol level of 240 mg/dL or higher, or a prescription of a lipid-lowering drug at least once per year under ICD-10-CM code E78.
Statistical analysis
The baseline characteristics according to the development of ocular motor CNP were compared using the Student’s t test for analysis of variance for the continuous variables and the chi-squared test for the categorical variables. All data are presented as mean ± standard deviation (SD). Cox proportional hazard regression analysis was performed for ocular motor CNP development according to the presence of migraine. To adjust for other confounders, we set and compared three models independently. Model 1 was analyzed with no adjustment. Model 2 adjusted for age, sex, smoking status, drinking amount, regularity of physical activity, and income status as potential confounding factors. Model 3 had additional adjustments for the calculated BMI and comorbidities including hypertension, diabetes mellitus, dyslipidemia, and glomerular filtration rate (GFR) in the setting of model 2. The hazard ratio (HR) and confidence interval (CI) were calculated, and we evaluated whether the incidence of ocular motor CNP was increased in the population with migraines compared to the population without them. To evaluate the effect of other factors on the association of migraine with ocular motor CNP, we performed subgroup analysis. We evaluated the effect of age over 65, sex, smoking status, diabetes mellitus, hypertension, and dyslipidemia in the subgroup analysis. The analyses were conducted with SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). A p-value of < 0.05 was considered statistically significant.
Ethics approval
This study adhered to the tenets of the Declaration of Helsinki and was approved by the Institutional Review Board of Samsung Medical Center (IRB; IRB no. SMC 2020-09-050).
Consent to participate
Consent from the individual patients was waived because the data used were public and anonymized under confidentiality guidelines.
Consent for publication
Consent for publication was waived because the data used were public and anonymized under confidentiality guidelines.
Results
Study population
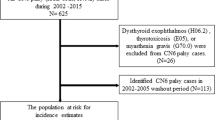
We followed up 4,053,824 eligible subjects for 33,323,032.76 person-years, during which 5806 (0.14% of subjects) developed ocular motor CNP and were assigned to the CNP group and 4,048,018 were assigned to the control group (Fig. 1). The average follow-up duration was 8.22 ± 0.93 years. The baseline characteristics were compared according to the presence of migraine (Table 1). Many factors were significantly associated with the presence of migraine, e.g., age, sex, smoking status, drinking amount, regularity of physical activity, income status, BMI, and comorbidities including hypertension, diabetes mellitus, dyslipidemia, and GFR. We considered these possible confounding variables when evaluating the independent relationship between migraines and ocular motor CNP.

Flowchart of the enrollment process of the current study cohort. N numbers, CNP ocular motor cranial nerve palsy.
The risk of ocular motor CNP according to the presence of migraine
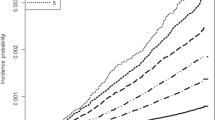
The incidence of ocular motor CNP was increased in the population with migraines compared to the population without migraines (Fig. 2). In model 1 without adjustment, the patients with migraines had an HR for ocular motor CNP of 1.252 (95% CI 1.088–1.440) compared to the population without migraines. In model 2, the HR was 1.168 (95% CI 1.015–1.345). After full adjustment for the comorbidities in model 3, the HR was 1.166 (95% CI 1.013–1.343).

Kaplan–Meier survival curve of outcomes for ocular motor cranial nerve palsy according to the presence of migraine.
The risk of ocular motor CNP in subgroup analysis according to age, sex, smoking status, and comorbidities including diabetes mellitus, hypertension, and dyslipidemia
Table 2 shows the incidence rates and multivariable-adjusted HRs for the development of ocular motor CNP according to age, sex, smoking status, and comorbidities including diabetes mellitus, hypertension, and dyslipidemia. The analysis was also adjusted for other variables such as age, sex, smoking status, drinking amount, regularity of physical activity, income status, calculated BMI, and comorbidities including hypertension, diabetes mellitus, dyslipidemia, and GFR. The subgroups of relatively younger age less than 65 years (HR = 1.267, 95% CI 1.067–1.504), male gender (HR = 1.228, 95% CI 1.000–1.122), smokers (HR = 1.426, 95% CI 1.127–1.803), and diabetes mellitus patients (HR = 1.378, 95% CI 1.045–1.378) showed a stronger association between migraines and the development of ocular motor CNP compared to the subgroups without them.
Discussion
This is a nationwide, population-based cohort study, demonstrating risk factors of ocular motor CNP in migraine patients. Migraine patients with young age, male gender, current smoking status, and diabetes mellitus showed a higher risk of ocular motor CNP development compared to those without them. The incidence of ocular motor CNP among Koreans appeared to be positively associated with the presence of migraine, which agrees with a previous study in Taiwan21. In our study, these outcomes were significant with or without adjustment for various confounders including age, sex, smoking status, drinking amount, regularity of physical activity, BMI, income status, and the comorbidities of hypertension, diabetes mellitus, dyslipidemia, and GFR.
Migraine is a very common neurobiological headache disorder that is caused by increased excitability of the central nervous system (CNS) and is characterized by various combinations of neurological, gastrointestinal, and autonomic changes25. It ranks high among global disabilities26. As the association between migraines and ocular motor CNP was raised in only one previous study21, there have not been extensive discussions on this association. The authors in the previous study suggested that the development of ocular motor CNP in patients with migraines may have been due to microvascular ischemia21. Although the exact mechanism of migraine generation is not completely understood, the now generally accepted mechanism for migraine headaches is the neurovascular hypothesis26,27,28,29,30,31,32,33. Study results have supported that migraine with aura begins with an event evolving cortical spreading depression (CSD), which in turn, activates the trigeminovascular system, the system that allows for nociceptive signals from the meningeal blood vessels to transmit to higher centers of the CNS27,28,29,30. When activated, the trigeminal sensory nerves trigger the release of vasoactive neuropeptides, which results in vasodilation and dural plasma extravasation, leading to neurogenic inflammation26. Pain impulses are then transmitted through the trigeminovascular system to the trigeminal nucleus caudalis, then to higher cortical pain centers in the brain26,34,35. CSD may predispose to CNS dysfunction by activating an inflammatory cascade, by hypoperfusion as spreading oligemia, and by a neurovascular coupling failure to provide a sufficient blood flow increase for the energy demand increase in CSD31,36,37,38,39,40. We could postulate that these complex cascades including neurogenic inflammation and the failure of neurovascular coupling may contribute to the development of ocular motor CNPs, although further studies are needed to validate this theory. Also, regarding the previous evidence suggesting that the vascular system in migraine patients is impaired at a systemic level including impaired compliance of the arterial system and endothelial dysfunction such as altered flow-mediated dilation and reduced endothelial progenitor cells41, we could not rule out the possibility that a peculiar vascular vulnerability of migraine patients contributes both to the development of migraines and the development of CNP.
In our study, we found that especially, migraine patients with young age, male gender, current smoking status, and diabetes mellitus showed a higher risk of ocular motor CNP development compared to those without them, which has not been reported in previous studies. Gender differences in migraine and comorbidities have been mainly studied for ischemic stroke42,43,44. The previous studies, including five meta-analyses, reported a significant association between migraines, particularly migraines with aura, and the development of stroke42,44,45,46,47, and those associations were reported to be stronger in women, and women younger than 45 years42,43,44. The authors of the previous studies on the association between ischemic stroke and migraines reported that because the prevalence of migraines is three times lower in men than in women, the association was more uncertain for men42. However, no previous data are available on gender differences in the risk of the ocular motor CNP in migraine patients. Our study showed a male gender in patients with migraines increased the risk of CNP development. Although it needs to be confirmed through other studies, our findings suggested the possibility that male gender, along with young age and diabetes mellitus can be potential risk factors for ocular motor CNP development in migraine patients.
There were several limitations to this study. First, due to the retrospective study design, we could not confirm a causal relationship between migraines and ocular motor CNP. Although we took into consideration confounders in this study, all confounders such as current medications or all past medical history could not be removed due to the nature of the NHIS. Second, we only included a Korean adult population. Therefore, the application of these data to other races may need to be qualified.
In conclusion, in this relatively long-term population-based cohort study, we demonstrated a significant association between the presence of migraines and the incidence of ocular motor CNP. Relatively younger age, male gender, smoking, and diabetes patients with migraines could have a higher risk of developing ocular motor CNP. The possible pathophysiology underlying these associations, such as neurogenic inflammation related to migraine, needs to be explored through further research.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Jung, E. H., Kim, S. J., Lee, J. Y. & Cho, B. J. The incidence and etiology of sixth cranial nerve palsy in Koreans: A 10-year nationwide cohort study. Sci. Rep. 9, 18419. https://doi.org/10.1038/s41598-019-54975-5 (2019).
Dosunmu, E. O., Hatt, S. R., Leske, D. A., Hodge, D. O. & Holmes, J. M. Incidence and etiology of presumed fourth cranial nerve palsy: A population-based study. Am. J. Ophthalmol. 185, 110–114. https://doi.org/10.1016/j.ajo.2017.10.019 (2018).
Fang, C. et al. Incidence and etiologies of acquired third nerve palsy using a population-based method. JAMA Ophthalmol. 135, 23–28. https://doi.org/10.1001/jamaophthalmol.2016.4456 (2017).
Jung, E. H., Kim, S. J., Lee, J. Y. & Cho, B. J. The Incidence and etiologies of third cranial nerve palsy in Koreans: A 10-year nationwide cohort study. Ophthalmic Epidemiol. 27, 460–467. https://doi.org/10.1080/09286586.2020.1773870 (2020).
Jung, E. H., Kim, S. J., Lee, J. Y. & Cho, B. J. The incidence and presumed aetiologies of fourth cranial nerve palsy in Korea: A 10-year nationwide cohort study. Eye (Lond.) https://doi.org/10.1038/s41433-020-01374-0 (2021).
Bagheri, A., Fallahi, M. R., Abrishami, M., Salour, H. & Aletaha, M. Clinical features and outcomes of treatment for fourth nerve palsy. J. Ophthalmic Vis. Res. 5, 27–31 (2010).
Jacobson, D. M. Relative pupil-sparing third nerve palsy: Etiology and clinical variables predictive of a mass. Neurology 56, 797–798. https://doi.org/10.1212/wnl.56.6.797 (2001).
Wilker, S. C., Rucker, J. C., Newman, N. J., Biousse, V. & Tomsak, R. L. Pain in ischaemic ocular motor cranial nerve palsies. Br. J. Ophthalmol. 93, 1657–1659. https://doi.org/10.1136/bjo.2008.155150 (2009).
Jung, J. S. & Kim, D. H. Risk factors and prognosis of isolated ischemic third, fourth, or sixth cranial nerve palsies in the Korean population. J. Neuroophthalmol. 35, 37–40. https://doi.org/10.1097/WNO.0000000000000214 (2015).
Greco, D., Gambina, F. & Maggio, F. Ophthalmoplegia in diabetes mellitus: A retrospective study. Acta Diabetol. 46, 23–26. https://doi.org/10.1007/s00592-008-0053-8 (2009).
Jacobson, D. M., McCanna, T. D. & Layde, P. M. Risk factors for ischemic ocular motor nerve palsies. Arch. Ophthalmol. 112, 961–966. https://doi.org/10.1001/archopht.1994.01090190109029 (1994).
Keane, J. R. & Ahmadi, J. Most diabetic third nerve palsies are peripheral. Neurology 51, 1510–1510. https://doi.org/10.1212/wnl.51.5.1510 (1998).
Lustbader, J. M. & Miller, N. R. Painless, pupil-sparing but otherwise complete oculomotor nerve paresis caused by basilar artery aneurysm. Case report. Arch. Ophthalmol. 106, 583–584. https://doi.org/10.1001/archopht.1988.01060130633009 (1988).
Park, U. C., Kim, S. J., Hwang, J. M. & Yu, Y. S. Clinical features and natural history of acquired third, fourth, and sixth cranial nerve palsy. Eye (Lond.) 22, 691–696. https://doi.org/10.1038/sj.eye.6702720 (2008).
Bendszus, M. et al. MRI in isolated sixth nerve palsies. Neuroradiology 43, 742–745. https://doi.org/10.1007/s002340100572 (2001).
Akagi, T., Miyamoto, K., Kashii, S. & Yoshimura, N. Cause and prognosis of neurologically isolated third, fourth, or sixth cranial nerve dysfunction in cases of oculomotor palsy. Jpn. J. Ophthalmol. 52, 32–35. https://doi.org/10.1007/s10384-007-0489-3 (2008).
Chou, K. L. et al. Acute ocular motor mononeuropathies: Prospective study of the roles of neuroimaging and clinical assessment. J. Neurol. Sci. 219, 35–39. https://doi.org/10.1016/j.jns.2003.12.003 (2004).
Murchison, A. P., Gilbert, M. E. & Savino, P. J. Neuroimaging and acute ocular motor mononeuropathies: A prospective study. Arch. Ophthalmol. 129, 301–305. https://doi.org/10.1001/archophthalmol.2011.25 (2011).
Tamhankar, M. A. et al. Isolated third, fourth, and sixth cranial nerve palsies from presumed microvascular versus other causes: A prospective study. Ophthalmology 120, 2264–2269. https://doi.org/10.1016/j.ophtha.2013.04.009 (2013).
Schultz, K. L. & Lee, A. G. Diagnostic yield of the evaluation of isolated third nerve palsy in adults. Can. J. Ophthalmol. 42, 110–115. https://doi.org/10.3129/canjophthalmol.06-099 (2007).
Yang, C. P., Chen, Y. T., Fuh, J. L. & Wang, S. J. Migraine and risk of ocular motor cranial nerve palsies: A nationwide cohort study. Ophthalmology 123, 191–197. https://doi.org/10.1016/j.ophtha.2015.09.003 (2016).
Song, S. O. et al. Background and data configuration process of a nationwide population-based study using the Korean national health insurance system. Diabetes Metab. J. 38, 395–403. https://doi.org/10.4093/dmj.2014.38.5.395 (2014).
Seong, S. C. et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 7, e016640. https://doi.org/10.1136/bmjopen-2017-016640 (2017).
National Health Insurance Service. National Health Screening Statistical Yearbook (National Health Insurance Service, 2014).
Silberstein, S. Migraine. Lancet (London) 363, 381–391 (2004).
Peters, G. L. Migraine overview and summary of current and emerging treatment options. Am. J. Manag. Care 25, S23–S34 (2019).
Vincent, M. B. & Hadjikhani, N. Migraine aura and related phenomena: Beyond scotomata and scintillations. Cephalalgia 27, 1368–1377. https://doi.org/10.1111/j.1468-2982.2007.01388.x (2007).
Tfelt-Hansen, P. C. & Koehler, P. J. One hundred years of migraine research: Major clinical and scientific observations from 1910 to 2010. Headache 51, 752–778. https://doi.org/10.1111/j.1526-4610.2011.01892.x (2011).
Tfelt-Hansen, P. C. History of migraine with aura and cortical spreading depression from 1941 and onwards. Cephalalgia 30, 780–792. https://doi.org/10.1111/j.1468-2982.2009.02015.x (2010).
Ayata, C. Spreading depression: From serendipity to targeted therapy in migraine prophylaxis. Cephalalgia 29, 1095–1114. https://doi.org/10.1111/j.1468-2982.2009.01982.x (2009).
Sacco, S. & Kurth, T. Migraine and the risk for stroke and cardiovascular disease. Curr. Cardiol. Rep. 16, 524. https://doi.org/10.1007/s11886-014-0524-1 (2014).
Dodick, D. W. A phase-by-phase review of migraine pathophysiology. Headache 58(Suppl 1), 4–16. https://doi.org/10.1111/head.13300 (2018).
Goadsby, P. J. & Holland, P. R. An update: Pathophysiology of migraine. Neurol. Clin. 37, 651–671. https://doi.org/10.1016/j.ncl.2019.07.008 (2019).
Noseda, R. & Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, cortical spreading depression, sensitization, and modulation of pain. Pain 154(Suppl 1), S44–S53. https://doi.org/10.1016/j.pain.2013.07.021 (2013).
Bigal, M. E., Ferrari, M., Silberstein, S. D., Lipton, R. B. & Goadsby, P. J. Migraine in the triptan era: Lessons from epidemiology, pathophysiology, and clinical science. Headache 49(Suppl 1), S21–S33. https://doi.org/10.1111/j.1526-4610.2008.01336.x (2009).
Lauritzen, M., Skyhoj Olsen, T., Lassen, N. A. & Paulson, O. B. Changes in regional cerebral blood flow during the course of classic migraine attacks. Ann. Neurol. 13, 633–641. https://doi.org/10.1002/ana.410130609 (1983).
Kurth, T., Chabriat, H. & Bousser, M. G. Migraine and stroke: A complex association with clinical implications. Lancet Neurol. 11, 92–100. https://doi.org/10.1016/S1474-4422(11)70266-6 (2012).
Hadjikhani, N. et al. Mechanisms of migraine aura revealed by functional MRI in human visual cortex. Proc. Natl. Acad. Sci. U.S.A. 98, 4687–4692. https://doi.org/10.1073/pnas.071582498 (2001).
Bigal, M. E., Kurth, T., Hu, H., Santanello, N. & Lipton, R. B. Migraine and cardiovascular disease: Possible mechanisms of interaction. Neurology 72, 1864–1871. https://doi.org/10.1212/WNL.0b013e3181a71220 (2009).
Attwell, D. et al. Glial and neuronal control of brain blood flow. Nature 468, 232–243. https://doi.org/10.1038/nature09613 (2010).
Sacco, S. et al. Peripheral vascular dysfunction in migraine: A review. J. Headache Pain 14, 80. https://doi.org/10.1186/1129-2377-14-80 (2013).
Schurks, M. et al. Migraine and cardiovascular disease: Systematic review and meta-analysis. BMJ 339, b3914. https://doi.org/10.1136/bmj.b3914 (2009).
MacClellan, L. R. et al. Probable migraine with visual aura and risk of ischemic stroke: The stroke prevention in young women study. Stroke 38, 2438–2445. https://doi.org/10.1161/STROKEAHA.107.488395 (2007).
Etminan, M., Takkouche, B., Isorna, F. C. & Samii, A. Risk of ischaemic stroke in people with migraine: Systematic review and meta-analysis of observational studies. BMJ 330, 63. https://doi.org/10.1136/bmj.38302.504063.8F (2005).
Spector, J. T. et al. Migraine headache and ischemic stroke risk: An updated meta-analysis. Am. J. Med. 123, 612–624. https://doi.org/10.1016/j.amjmed.2009.12.021 (2010).
Mahmoud, A. N. et al. Migraine and the risk of cardiovascular and cerebrovascular events: A meta-analysis of 16 cohort studies including 1 152 407 subjects. BMJ Open 8, e020498. https://doi.org/10.1136/bmjopen-2017-020498 (2018).
Hu, X., Zhou, Y., Zhao, H. & Peng, C. Migraine and the risk of stroke: An updated meta-analysis of prospective cohort studies. Neurol. Sci. 38, 33–40. https://doi.org/10.1007/s10072-016-2746-z (2017).
Funding
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No.NRF-2021R1A2C1007718) to Kyung-Ah Park and the Basic Science Research Program through the NRF funded by the Ministry of Science and ICT (2021R1F1A1047180) to Sei Yeul Oh.
Author information
Authors and Affiliations
Contributions
S.R. and K.P. wrote the main manuscript text and K.H. and J.Y. prepared and analyzed the data and prepared figures 1-2 and tables 1-2 and S.Y.O supervised the design and analyzing results of this study. All authors reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rhiu, S., Han, K., Yoo, J. et al. Association between migraine and risk of ocular motor cranial nerve palsy. Sci Rep 12, 10512 (2022). https://doi.org/10.1038/s41598-022-14621-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-14621-z
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
