
Abstract
Understanding the epidemiology and risk factors of adverse drug events (ADEs) in pediatric inpatient is essential if we are to prevent, reduce or ameliorate the harm experienced. The Global Trigger Tool (GTT) is a method of retrospective medical record review that measures harm in hospitalized children. We employed a three-stage retrospective chart review of random samples of 1800 pediatric inpatients discharged from January 2013 to December 2015. 31 kinds of pediatric-specific triggers were made based on the previous trigger tool studies developed for use in adult or pediatric. Positive predictive value (PPV) of individual triggers, as well as ADEs detection rates were calculated. Stepwise logistic regression was performed to investigate risk factors associated with ADEs. Of 1746 patients, detected in 221 patients (12.7%) with 247 ADEs. The PPV of the trigger tool was 13.3%. Of the 247 ADEs, 82.6% were identified as category E, 11.7% category F and 5.7% category H. The pediatric-focused trigger tool is a feasible and useful tool for detecting pediatric ADEs. Especially for patients who have had more drugs, more doses or more admissions which needs to be closely monitored as triggers to improve the safety.
Similar content being viewed by others


Introduction
Adverse drug events (ADEs) are defined by the Institute of Medicine (IOM) as injuries resulting from a medical intervention related to a drug and can manifest as signs, symptoms or laboratory abnormalities1. This is more general definition than that provided by the World Health Organization, which defined an adverse drug reaction (ADR) as a response to a drug, which is noxious and unintended, and occurs at doses normally used in man for prophylaxis, diagnosis or therapy of disease, or for the modification of physiologic function2. Because this definition of ADR excludes overdose, drug abuse and treatment failure and drug administration errors. An adverse event was defined as any injury (not just that associated with medication or drug use) caused by medical management rather than by the underlying disease or condition of the patient3. We only concerned with medication associated adverse events, such as ADR and drug administration errors. ADEs are important causes of iatrogenic morbidity and mortality, especially for children, but the frequency of ADEs is unknown. The reported rates of ADEs range from 0.6% to 20%4,5, due to the differences in definitions of ADEs, methods, prescribing habits, age group, and clinical settings. Traditional methods to detect ADEs have focused on voluntary reporting. However, public health researchers have established that on average only 10–20% of errors are ever reported and of those, 90–95% cause no harm to patients6. The Global Trigger Tool (GTT) developed by the Institute for Healthcare Improvement (IHI) is a retrospective review of a random sample of inpatient hospital records using “trigger” to identify possible adverse events6. The GTT, which requires minimal training, appears to increase the rate of ADE detection 50-fold from traditional reporting methods7. Using the GTT, Classen et al. found at least ten times more confirmed, serious events than tradition methods8. A trigger is a clue condition believed to be associated with the occurrence of an adverse event. The triggers themselves represent specific events including the ordering of certain medications (e.g., antidotes, such as Naloxone), the result of certain abnormal laboratory values (e.g. supratherapeutic serum medication concentrations, such as vancomycin), change in clinical status or symptom (e.g., drug-related rash), and abrupt stop orders et al.3. In recent years, the GTT has been used in pediatric populations worldwide, such as in the US9,10, UK11, Norway12, Australia13, and Japan4, has been proved to be reasonable and reliable.
The occurrence of ADEs is associated with both patient characteristics and their health care utilization. With regard to risk factors associated with ADEs in pediatric patients, significant differences have been found in terms of the number of drugs14, length of hospital stay15, use of antibacterial15 and general anesthesia16. However, such findings are not always consistent; while some studies found that gender was not significantly associated with ADEs17, a study also found that males were at higher ADEs risk compared to females18. In addition, little is known about the performance of the GTT and risk factors associated with the occurrence of ADEs in Chinese pediatric inpatients. Practical and reliable methods are needed to identify and detect ADEs in hospital practice. Therefore, The aim of this study was to estimate the frequency of ADEs in Chinese pediatric inpatients in tertiary care hospitals and characteristics associated with the occurrence of ADEs.
Results
Patients Characteristics
A total of 1800 patients involved in 1800 cases were identified, of which 54 were excluded including 28 without drug exposure and 26 diagnosed with cancer. Among the final records of 1746 cases, 1135 (65%) were from males and 611 (35%) from females. The age range was between 0.08~17.75 years old with a mean of 3.84, the average length of hospital stay was 7.83 ± 5.28 days (1~63 days), average drugs per patient were 14 ± 7 (1~64), and doses per patient was 114 ± 105 doses (1~1206 doses). Among those 221 patients who had ADEs, 199 (11.4%), 18 (1.0%), 4 (0.2%) patients had one, two and three or more ADEs, respectively. There were no significant differences in age, gender, number of medical diagnoses, admission in the last year, type of admission, department or surgical operation (p > 0.05), whereas significant differences were identified in the length of stay, antibacterial use, number of drugs, doses, triggers and number of admissions between patients with and with no ADEs (P ≤ 0.01) (Table 1).
Triggers
We established 31 kinds of triggers, among which 24 were positive (77.4%) during the chart review, and 23 associated with ADEs. Among the final 1746 cases, 1213 (69.5%) had positive triggers. A total of 2291 triggers were detected resulting in a mean rate of 1.3 triggers per patient. Trigger Positive predictive value (PPV) is the number of times a specific trigger independently identified an ADE divided by the number of times a trigger was identified positive. The overall PPV of the aggregate Children’s Hospital of Chongqing Medical University (CHCMU) trigger list was 13.3%. The number of positive triggers, ADEs and PPV for each trigger are displayed in Table 2.
ADE Characteristics
A total of 247 ADEs (Table 3) were identified in 221 patients (12.7%), 80.2% (198/247) occurred during hospital stays, and 19.8% (49/247) pre-existed as the reasons for the hospital admission: 204 (82.6%) were determined to be the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) harm category E, 29 (11.7%) were category F, and 14 (5.7%) were category H.
The calculated rates of these 247 ADEs based on 1746 patient records were 13.7 (95% CI 11.2 to 16.1) ADEs per 100 patients, 17.4 (95% CI 14.1 to 20.7) per 1000 patient days, 1.2 (95% CI 1.0 to 1.4) per 1000 doses, and 9.9 (95% CI 8.3 to 11.5) per 1000 drugs.
Risk factors associated with the occurrence of ADEs
Univariate analysis showed that the length of hospital stay, antibacterial use, numbers of drugs, doses and admissions were risk factors for the occurrence of ADEs (Table 1). Logistic regression results showed that only numbers of drugs, doses and admissions had a statistical significance (p < 0.05), while antibacterial use (p = 0.957) did not. Among them, the length of hospital stay was a protective factor (β = −0.101), for it did not in accord with the report in the literature19 (Table 4). This may not be independent of the various risk factors, but there is a certain linear correlation, namely multicollinearity.
Multicollinearity diagnostic results showed that the largest condition index was 9.932, and the variance were 37%, 48%, and 68% for the length of hospital stay, number of drugs, and number of doses, respectively, suggesting collinearity (Table 5).
ADEs as a dependent variable, the number of drugs, doses, admissions and antibacterial use were screened into multivariate analysis. The significant factors associated with the occurrence of ADEs were the number of drugs, number of doses and number of admission (Table 6).
Discussion
We established 31 kinds of pediatric-focused triggers of ADEs. We increased the case of ‘A9 Nystatin and Sodium bicarbonate use’ and did not include the case of use for Vitamin K, which was different from the prior study. This may be relate to the fact that many people use Vitamin K for children post-operative supplement, ease bronchospasm and so on perhaps owing to cultural background. Thus, cases of use for Vitamin K were included, which led to many false positive results.
Our overall PPV of the trigger tool was 13.3%, within the range of other trigger tools in pediatric care from 3.7% to 38%9,10,11,12,20,21 that might reflect variations in practice. Among the 31 kinds of triggers, substantial differences in the PPV of individual triggers were found. Some triggers had shown a high PPV of >50%, such as ‘A2 Flumazenil use’,‘A9 Nystatin and Sodium bicarbonate use’, and ‘T1 Abrupt medication stop’; whereas four frequently identified triggers (≥300) had very low PPV, which might be due to the following reasons. First, in cases of anti-emetic use, false positives might have resulted from the common prophylactic use of anti-emetics in chemotherapy and post-operative care. Second, laxatives were often administered in patients with invasive procedures or surgical operations for preoperative preparation. Third, for the trigger ‘A1 Anti-allergic or Adrenaline use’ and ‘A7 Antidiarrheal or Antidiarrheal administration’, these drugs were commonly used for disease treatment as well as ADEs, leading to false positive results. Therefore, these triggers should be further specified for their use in treatment of disease or ADEs. In addition, some of the triggers were not identified in the review process such as blood drug concentrations, likely due to fewer pediatric patients on treatment or lack of monitoring.
The incidence of pediatric ADEs in this study was found to be similar to or lower than those found in other studies: Takata et al. reported 15.7 ADEs per 1000 patient-days9; Sakuma et al. reported 37.8 ADEs per 1000 patient-days4. These differences may reflect variations in local practices and study subjects. Among all ADEs identified in this study, there was no category G or I, and 94.3% were identified as temporary harm to the patient. This finding may be partially due to the short study duration and also explained by the fact that patients were excluded in the Hematology and Oncology, pediatric intensive care unit (PICU) or Neonatal Ward patients.
The risk factors for ADEs in pediatric inpatients included, but not limited to, the number of drugs, the number of doses, and the number of admissions in our study. Gender and age were not associated with the occurrence of ADEs in this study. This was consistent with previous findings17,22. A study showed that age is not an independent risk factor of ADEs, older children were likely to experience ADEs has been shown to be associated with they have more opportunities for the use of high-risk drugs17.
The increase in the number of drugs was most frequently found to be independent risk factors for ADEs. A systematic review of 26 studies with a total of 85212 patients confirmed that the number of drugs was an independent risk factor for ADEs14. This may be due to the additional risk of an ADEs when receiving several drugs, to drug-drug or drug-disease interactions, and to greater susceptibility of medication errors during hospital stay. Patients at an increase in the number of doses were more likely to experience ADEs, however additional studies are required to identify the risk factor for ADEs.
The number of admissions as a risk factor might due to the use of high-risk drugs. The children with more number of admissions in our study were mostly diagnosed with epilepsy, kidney disease, diabetes and other chronic diseases or recurrent infection, and for the treatment of specialist drug, such as anti-epileptics, systemic corticosteroids, immunosuppressive agents, analgesics, and antibacterial have been shown to be high risk for ADEs in hospitalized children by Rashed et al.17. Single factor analysis showed that the use of antibiotics was a risk factor for ADEs, while there was no significant difference between the stepwise logistic regression analysis, we could not rule out that it was not associated with the occurrence of ADEs.
The length of hospital stay as a risk factor for ADEs is controversial. Some studies have been considered that the length of hospital stay was a risk factor for ADEs, while others considered ADEs could be a cause of longer length of stay17,22. Length of hospital stay was significantly associated with the occurrence of ADEs, but the causal relationship need more research to confirm. Patients who stayed longer might have a need for more drugs, so they might have more opportunities to experience ADEs, while ADEs might result in a longer hospital stay. The number of drugs was an independent risk factor, and there was a linear relationship with the number of doses and the length of hospital stay, which may partly explain the relationship between hospital stay and ADEs. In line with Asia et al., we considered the length of hospital stay as a consequence of having an ADE but not as a risk factor for ADEs17.
This study showed that the IHI GTT was a useful method for the detection of ADEs in a Children’s hospital in China. However, there were some limitations. First, the 31 kinds of pediatric-focused triggers of ADEs could be improved to be more specific. Second, the triggers should be further tested in more pediatric including those in the Hematology and Oncology, PICU and Neonatal Units.
Conclusion
To our knowledge, this was the first study to investigate ADEs of pediatric inpatients using GTT in China. More than one fifth of the pediatric inpatients experienced at least one ADEs, and most of the experiences caused temporary harm. The most significant factors of ADEs included the number of drugs, the number of doses and the number of admissions. In addition, triggers that had high PPV could be incorporated into routine screen systems to improve inpatient safety in the future.
Methods
Study design, setting and sample
This study employed retrospective medical record reviews. We conducted this study in the CHCMU, a large tertiary teaching children’s hospital in China. The hospital had 1400 beds. The number of inpatients was 65 thousand in 2014 and that of outpatients and emergency patients was 2.18 million annually. The hospital has fully electronic medical record and bar code systems for administering medications.
The sample size was 600 cases per year. It was determined on the basis of the prior studies indicating that the rate of pediatric inpatients ADEs was about 15%. The annual number of inpatients set a precision of ±3% with a 0.05 probability of type 1 error, after it was considering not conformed to the standard records we appropriately expand.
Study source
Medical record management system was used to extract medical record conformed to the following standard patients from January 1, 2013 to December 31, 2015. Eligible patients were more than 28 days old and less than 18 years old, with a length of more than one days hospital stay and were discharged or died between January 1, 2013 and December 31, 2015. Patients were excluded if they were without drug exposure or when they were in PICU, in neonatal ward, in Hematology and Oncology, in the day hospital or observation unit. Random equidistant sampling method was used for sampling. A sample of 50 patients was randomly selected from standard patients monthly, which began in January 2013, with a total of 1800 patients.
Triggers
The trigger items of CHCMU were developed based on 51 kinds of triggers recommended in ‘IHI GTT for Measuring Adverse Events’ and previous trigger tool studies by using triggers. Through the preliminary experiment and consultation, the experts determined the trigger list.
Records Review
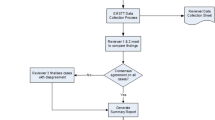
We employed a three-stage review process for medical records. In the first stage, one pharmacist reviewed each medical record for the presence of any of the triggers with a limit of no more than 20 min per chart. The medical records were reviewed in the following order: diagnoses and treatment procedures, discharge summaries, medication charts, laboratory results, operation notes, nurse notes, physician notes and admission note. The basic information of patients was recorded with the identified trigger, which led to a further review to determine the occurrence of ADEs.
In the second stage, two pediatricians reviewed all the medical records with identified triggers from the first stage to determine the presence of ADEs, its category and severity. If there was a disagreement, the final decision was made on the basis of a consensus at the research team meetings.
In the third stage, the pharmacist entered the data of the medical record review. All reviewers were required to read the white paper of the ‘IHI GTT for Measuring Adverse Events’ and trained in records review methods before the review.
We focused on ADEs that cause actual patient harm, but not medical errors that has potentials for patient harm. Harm was defined as an unintended physical injury resulting from or contributing to medical care that requires additional monitoring, treatment or hospitalization, or that results in death. Once harm was identified, its severity was evaluated by using the classification from the NCC MERP Index for Categorizing Errors6. It included temporary harm to the patient and required intervention (category E), temporary harm to the patient and required initial or prolonged hospitalization (category F), permanent patient harm (category G), required intervention to sustain life (category H), and the patient’s death (category I).
Statistical Analysis
Data were analyzed by using Microsoft Excel 2011 and SPSS 23.0 software. We calculated ADEs per 100 patients admissions, ADEs per 1000 patient days, ADEs per 1000 doses and ADEs per 1000 drugs. Comparisons between groups were made by using the χ2 test for categorical variables and t test for continuous variables. P Values lower than 0.05 were considered significant. Stepwise logistic regression was used to investigate risk factors associated with ADEs. Multiple collinearity diagnosis was performed by variance decomposition proportion.
Ethics Statement
This study was exempt from ethical review by the Institutional Review of the Children’s Hospital of Chongqing Medical University. Its compliance with the Ministry of Health’s 2007 Chinese Regulation on Ethical Review of Biomedical Research Involving Human Subjects. The methods were carried out in accordance with the relevant guidelines and regulations.
References
Marcum, Z. A. et al. Utility of an adverse drug event trigger tool in Veterans Affairs nursing facilities. J.Consult Pharm. 28, 99–109 (2013).
Malladi, P. A study of adverse drug reactions reported to the adverse drug reaction monitoring centre at a tertiary care teaching hospital, kuppam. J. Pharmacy and Pharmaceutial Sciences. 5, 804–12 (2016).
Resar, R. K., Rozich, R. K. & Classen, D. Methodology and rationale for the measurement of harm with trigger tools. J.Quality and Safety in Health Care. 12, 39–45 (2003).
Sakuma, M. et al. Adverse drug events and medication errors in Japanese paediatric inpatients: a retrospective cohort study. J.BMJ Qual Saf. 23, 830–7 (2014).
Smyth, R. M. D. et al. Adverse drug reactions in children–a systematic review. J.PLoS One. 7, e24061 (2012).
Griffin, F. A. & Resear, R.K. IHIGlobal Trigger Tool for Measuring Adverse Events(Second Edition). Cambridge, Massachusetts: Institute for Healthcare Improvement (2009).
Steven, M. H. & Joesph, T. H. Detecting Adverse Drug Events Using a Nursing Home Specific Trigger Tool. J.Ann Longterm Care. 18, 17–22 (2010).
Classen, D. C. et al. ‘Global trigger tool’ shows that adverse events in hospitals may be ten times greater than previously measured. J.Health Aff (Millwood). 30, 581–9 (2011).
Takata, G. S., Mason, W., Taketomo, C., Logsdon, T. & Sharek, P. J. Development, testing, and findings of a pediatric-focused trigger tool to identify medication-related harm in US children’s hospitals. J.Pediatrics. 121, e927–35 (2008).
Kirkendall, E. S. et al. Measuring adverse events and levels of harm in pediatric inpatients with the Global Trigger Tool. J.Pediatrics. 130, e1206–14 (2012).
Chapman, S. M., Fitzsimons, J., Davey, J. & Lachman, P. Prevalence and severity of patient harm in a sample of UK-hospitalised children detected by the Paediatric Trigger Tool. J. BMJ Open. 4 e005066 (2014).
Solevag, A. L. & Nakstad, B. Utility of a Paediatric Trigger Tool in a Norwegian department of paediatric and adolescent medicine. J.BMJ Open. 4, e005011 (2014).
Hibbert, P. D. et al. CareTrack Kids-part 3. Adverse events in children’s healthcare in Australia: study protocol for a retrospective medical record review. J.BMJ Open. 5, e007750 (2015).
Saedder, E. A., Lisby, M., Nielsen, L. P., Bonnerup, D. K. & Brock, B. Number of drugs most frequently found to be independent risk factors for serious adverse reactions: a systematic literature review. J.Br J Clin Pharmacol. 80, 808–17 (2015).
Andrade, P. H. S., Santos, A. D. S., Souza, C. A. S., Lobo, I. M. F. & Silva, W. B. D. Risk factors for adverse drug reactions in pediatric inpatients: a systematic review. J.Ther Adv Drug Saf. 8, 199–210 (2017).
Thiesen, S. et al. Incidence, characteristics and risk factors of adverse drug reactions in hospitalized children – a prospective observational cohort study of 6,601 admissions. J.BMC Medicine. 7, 10 (2013).
Rashed, A. N. et al. Risk factors associated with adverse drug reactions in hospitalised children: international multicentre study. J.Eur J Clin Pharmacol. 68, 801–10 (2012).
Star, K., Norén, G. N., Nordin, K. & Edwards, R. Suspected Adverse Drug Reactions Reported For Children Worldwide:An Exploratory Study Using VigiBase. J.Drug-Safety. 34, 415–28 (2011).
Hwang, J. I., Chin, H. J. & Chang, H. J. Characteristics associated with the occurrence of adverse events: a retrospective medical record review using the Global Trigger Tool in a fully digitalized tertiary teaching hospital in Korea.J. J Eval Clin Pract. 20, 27–35 (2014).
Stockwell, D. C. et al. A Trigger Tool to Detect Harm in Pediatric Inpatient Settings. J.Pediatrics. 135, 1036–42 (2015).
Unbeck, M. et al. Validation of triggers and development of a pediatric trigger tool to identify adverse events. J.BMC Health Serv Res. 14, 655 (2014).
Munoz-Torrero, J. F. S. et al. Adverse drug reactions in internal medicine units and associated risk factors[J]. Eur J Clin Pharmacol. 66, 1257–64 (2010).
Rozich, J. D., Haraden, C. R. & Resar, R. K. Adverse drug event trigger tool:a practical methodology for measuring medication related harm. J.Qual Saf Health Care. 12, 194–200 (2003).
Rozenfeld, S., Giordani, F. & Coelho, S. Adverse drug events in hospital: pilot study with trigger tool. J. Rev Saude Publica. 47, 1102–11 (2013).
Acknowledgements
This work was supported by the Health and Family Planning Commission of Chongqing grants (2016ZDXM017), Chongqing Science and Technology Commission grants (cstc2016shmszx130048).
Author information
Authors and Affiliations
Contributions
All the authors were involved in the study. Study design: Lin Song, Jian-wen Xiao, Huan-huan Ji and Yun-tao Jia. Sampling: Ting-ting Tang, Huan-huan Ji. Record review: Huan-huan Ji, Yu-xia Guo, Ping Wei. Analysis and interpretation of data: Huan-huan Ji, Xue-wen Tang, Xiao-jiang Tian and Yun-tao Jia. All the authors took part in the discussions of the results and contributed to the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ji, Hh., Song, L., Xiao, Jw. et al. Adverse drug events in Chinese pediatric inpatients and associated risk factors: a retrospective review using the Global Trigger Tool. Sci Rep 8, 2573 (2018). https://doi.org/10.1038/s41598-018-20868-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-20868-2
This article is cited by
-
Adverse drug events and contributing factors among pediatric cancer patients at Jimma University medical center, Southwest Ethiopia
BMC Pediatrics (2023)
-
Impact of suspected adverse drug reactions on mortality and length of hospital stay in the hospitalised patients: a meta-analysis
European Journal of Clinical Pharmacology (2023)
-
Causality and preventability assessment of adverse drug events of antibiotics among inpatients having different lengths of hospital stay: a multicenter, cross-sectional study in Lahore, Pakistan
BMC Pharmacology and Toxicology (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
