
Abstract
Chemotherapy is a primary treatment for the metastatic lung cancer patients. To select the most effective combination of drugs, we need an efficient way of assessing tumor response. Here, we showed that differential scanning calorimetry (DSC) analysis of blood serum proteins could reveal the patient response to the treatment. If chemotherapy is effective, serum proteins DSC curve of non-small cellular lung cancer (NSCLC) case is similar to the those of the healthy individuals. If treatment fails, notable changes occur in the DSC profile of NSCLC patient’s blood serum. Our preliminary work illustrates how thermal analysis of changes in the heat capacity of blood serum proteins can provide an insight into patient response to chemotherapy – the essential information for any successive lung cancer treatment.
Similar content being viewed by others


Introduction
Lung cancer remains the leading cause of cancer-related death worldwide1,2. The high mortality is due to late cancer diagnosis, at a stage when the tumor has already spread to other organs (metastasis)3. At this metastatic stage, treatment options are usually limited to chemotherapy or targeted therapy.
Almost all chemotherapeutic drugs have been designed to inhibit DNA replication or cell division in rapidly dividing tumor cells. However, these drugs efficacy is difficult to assess during the treatment.
At present, we rely on a frequent radiological scanning (e.g., spiral computed tomography) to determine therapy effectiveness by monitoring changes in tumors distribution and size4. On the other hand, the abundance of the blood samples makes it attractive to assess chemotherapeutic efficacy based on, for instance, the blood serum proteins. Unfortunately, it remains a challenge, mostly due to a lack of established lung cancer biomarkers.
Nonetheless, the blood serum proteins contain multiple cancer- and treatment-related signatures. First, the epigenetic changes associated with cancer manifest themselves in altered type, sequence and structure of expressed proteins at the cellular level (e.g., overexpression of growth factors and their receptors)5,6. Second, an effective chemotherapy reduces the number of cancerous cells, thus reducing the number of abnormally expressed proteins. Because the alteration of proteins is the cellular/extracellular signature of both malignant DNA alteration and chemotherapeutic drugs action, physicochemical analysis of cellular proteins should in principle allow one to detect treatment efficacy.
Among recently introduced methods for diagnostics and monitoring of diseases, the differential scanning calorimetry (DSC) seems to be the most promising one, regarding serum protein-based diagnosis7,8,9,10,11,12,13,14,15,16,17,18,19,20,21. DSC serum profile shows the heat capacity changes corresponding to the process of proteins unfolding as a function of a temperature. DSC evidences the absence or failure of protein structure or slight changes in protein stability. The weakness or stabilization of intermolecular interactions allows tracking of the molecules conformational change under the influence of environmental factors. The obtained DSC curve contains information about the thermodynamic stability of the most abundant serum proteins (i.e., their melting temperatures Tm and enthalpies of denaturation ΔH), protein mixture composition and the compositional changes taking place in the disease state, intra- and intermolecular interactions, including those related to alteration of protein structure. However, these data usually need skillful analysis because some of them are not directly available thus difficult to interpret. In applying DSC to blood serum proteins, one typically compares the denaturation curves obtained for a sick patient with the profile expected for the healthy individuals7,8,9,10,11,12,13,14,15,16,17,20,21,22. The disease-related alterations of serum proteins provide a diagnostic information evident on the DSC curve. DSC was tested to show the effects on blood serum caused by different injurious factors that are unavoidable in particular cases, e.g. necessary for treatment (chemotherapy, oxidative stress or neutron radiation)18,19,20,21. For instance, Ferencz et al. 21 showed that serum proteins denaturation profile of recovering breast cancer patients could indicate the tumor relapse. Here, we present the preliminary, but promising, results of DSC study of serum proteins obtained from metastatic lung cancer patients that respond positively or negatively to the platinum-based chemotherapy.
Results and Discussion
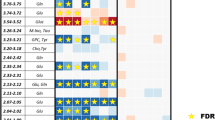
For our preliminary study, we selected eleven non-small cellular lung cancer (NSCLC) patients (nine adenocarcinomas and two squamous cell lung cancer) at stage IV after administered platinum-based chemotherapy. The reference group of healthy individuals consists of two men and three women (mean age ~61). All samples groups were matched with ethnicity (West-Slavic group), age and smoking status. The lung-cancer patients were between 57 and 77 years old (mean value of 65.1), and five of them were smokers (see Table 1). Among investigated cases there was a group of three patients with pronounced genomic alterations. EGFR (epidermal growth factors receptor) mutation was detected using real-time PCR (polymerase chain reaction). ALK (anaplastic lymphoma kinase) rearrangement was confirmed based on immunohistochemistry and FISH (fluorescent in situ hybridization). Our DSC analysis of plasma samples yielded a normalized, baseline-corrected denaturation curve for each blood sample (see Figs 1 and 2). The DSC profile for our healthy volunteers agree well with the similar literature data9, and is a reference to the DSC curves of lung cancer patients. It is typically decomposed into four protein groups (i.e., peaks)8,9. The two dominant and most relevant for our study are: peak corresponding to unligated albumin with a trace of haptoglobin centered at about 63 C (Tm1), and immunoglobulins peak located at about 70 C (Tm2), with intensities Cp1 ex, Cp2 ex respectively.

DSC curves obtained for blood serum samples from chemotherapy-treated LC patients with reduced progression (n = 8) and healthy individuals (n = 5).
The DSC profiles for all lung cancer patients (n = 11) differ from those of healthy ones (n = 5). The mean Tm1 for the control group (63.00 ± 0.54) is slightly higher than for NSCLC patients (62.37 ± 0.77) but the difference is not statistically significant. However, the mean Tm2 for NSCLC (69.85 ± 0.69) is higher than for the control group (68.86 ± 0.41) and the Student’s t-test shows statistically significant difference between these two groups (p = 0.01).
Eight out of eleven patients responded to chemotherapy, and they are referred as a stable metastatic lung cancer (smLC). Their DSC profiles resemble the one obtained for healthy individuals (see Fig. 1). It is not possible to show statistically significant differences between both subtypes of NSCLC, i.e., adenocarcinoma (mean age 65.6) and squamous cell lung cancer (mean age 62) due to the small sample size (only two patients with the second subtype). The smoking status doesn’t differentiate the shape of DSC curve.
In three patients the chemotherapy failed (referred as a progressive lung cancer, pLC*; mean age 65.3). The progressed patients had also EGFR mutation or ALK rearrangement. It is known that lung cancer patients with such abnormalities are more likely to respond to targeted treatment. Gross progression was the effect of ineffectual chemotherapy at moment of sampling. We observe that the serum DSC curve of chemotherapeutically non-responding patients (pLC*) differs significantly from those of the healthy or responding patients (Fig. 2). The results of a one – way ANOVA indicate statistically significant differences between these three groups in the Cp1 ex (p = 0.0003) as well as Cp2 ex intensities (p = 0.0006). The mean Cp1 ex value for pLC* patients (0.214 ± 0.077) is significantly lower than for smLC (0.387 ± 0.043; p = 0.001) and healthy (0.341 ± 0.023; p = 0.01) groups. The Cp2 ex value for pLC* patients (0.306 ± 0.031) is significantly higher than for smLC (0.230 ± 0.032; p = 0.02) and a little higher than for control group (0.270 ± 0.025). A similar change in a denaturation profile, i.e., a reduction of first denaturation peak and a significant increase in the high-temperature peak height, was reported by Garbett et al 9. for 30 lung cancer plasma samples. Another significant difference was found for Tm2 parameter. It is higher for smLC and pLC* than for healthy group (p = 0.025 in Kruskal-Wallis test), particularly for pLC* patients (Tm2 = 70.33 ± 0.22) in comparison with the healthy group (p = 0.02).

DSC curves obtained for blood serum samples from chemotherapy-treated LC with rapidly progressed adenocarcinoma patients (LCa7* without fluid in lungs; LCa8* and LCa3*- with massive fluid production); set with an average DSC profile for healthy individuals (n = 5).
By analyzing clinical data, we confirm that chemotherapy was ineffective in this patients and we observed a massive tumor progression. Moreover, the DSC curves reveal the intensification of observed clinical symptoms of the developing disease. In two of progressing patients (LC-a3* and LC-a8*) rapid production and retention of fluid in lungs occurred. One can try to correlate the change in the DSC profile with the presence of EGFR activating mutation or ALK rearrangement. However, a chemotherapy-induced decrease in the albumin contents or alteration of interactions between serum proteins might also influence DSC curves8,9. The albumin fraction in chemotherapy responded patients is 55.6–64.5% of total proteins while for progressed patients 57.2–60.1%. It suggests that reduction of the first denaturation peak over 50% is not an effect of the quantitative albumin changes. It appears that a main fraction of the albumin peak shifts towards higher temperatures (with a maximum above 70 C, see Fig. 2). This indicates an increase in the thermodynamic stability of albumins as a result of modification of interactions in pathologically affected serum (i.e., biomarkers interactions with the major plasma proteins)8,9. Though our results are in agreement with the literature data, the unambiguous identification of the origin of altered DSC curve requires further investigation.
Conclusions
We showed that the blood serum microcalorimetry is capable of differentiating metastatic lung cancer patients that respond well to chemotherapy from those who did not. If the selected chemotherapy drugs are effective, the DSC curve of serum proteins starts to resemble the DSC profile of the healthy individuals. What is more, a lack of tumor response to the treatment is also evident in the DSC curve. Even though serum protein DSC-based diagnosis is in its infancy and here we reported studies for a limited patient population, our results indicate that DSC can become a supportive method for monitoring lung cancer patient response to the chemotherapy.
Methods
The informed consent from lung cancer patients and healthy volunteers was obtained before the peripheral blood samples were taken. The study was approved by Bioethics Committee at Medical University in Lublin and followed all local laws and regulations. The total serum proteins were determined using biuret method. The total albumin level was detected by UV-Vis spectrometry with bromocresol green.
The protocols used for the serum preparation included centrifugation and aliquoting before freezing. 5 ml Vacutainer tubes containing clot activator were used for blood collection. Samples were centrifuged 30 min after collection for 10 min at 10000 rpm. The supernatant was transferred into 2 mL Eppendorf microcentrifuge tubes and immediately frozen at −80 C to avoid proteins changes until the measurement. Straightway before the DSC analysis, the sample was thawed out at room temperature for 15 minutes. Then the 20-fold diluted solution was prepared using 0.25 ml of sample and 4.75 ml of degassed phosphate saline buffer (PBS) with pH 7.4 (0.1 M). Serum samples and reference solutions were degassed adequately before careful load into the cells to avoid bubble formation. The cell volume was 0.5137 ml.
The differential scanning calorimetry profiles were recorded using a VP DSC MicroCal micro-calorimeter (Northampton, MA) in the temperature range from 20 to 100 °C. The scan rate was 1 °C min−1 with a pre-scan equilibration time 15 min. The buffer–buffer scan under the same conditions was used as an instrumental baseline. For each sample, the temperature programs were performed two times. Serum DSC curves were normalized for the gram mass of protein and next linear baseline was subtracted. DSC curves represent changes of excess heat capacity, Cp ex, (cal °C−1 g−1) in function of temperature.
The statistical analysis of parameters describing the thermal transition of serum (see data in the Table S1 in Supporting Information) was performed with Statistica 13. All results are given as mean values ± standard deviation. After checking for normal distribution (tested by Schapiro-Wilk test) and homogeneity of variance (Leven’s test), one-way analysis of variance (ANOVA) or independent- samples t-test for comparison of mean values were used. If ANOVA was statistically significant, Tukey’s post–hoc test for unequal sample sizes was applied. The Kruskal- Wallis H-test was used for non-normally distributed variables or in the case of non-homogenous variances. The level of statistical significance was set at p < 0.05.
Ethical statement
Authors confirm that the project was approved by Bioethics Committee at Medical University in Lublin and followed all local laws and regulations. The informed consent from all volunteers was obtained before the peripheral blood samples were taken.
References
Torre, L. A., Bray, F., Siegel, R. L., Ferlay, J. & Lortet-Tieulent, J. Cancer statistics, 2015. CA Cancer J. Clin. 65, 87–108 (2015).
Siegel, R., Ma, J., Zou, Z. & Jemal, A. Cancer statistics, 2014. CA Cancer J. Clin. 64, 9–29 (2014).
Mulshine, J. L. Screening for lung cancer: in pursuit of pre-metastatic disease. Nat. Rev. Cancer 3, 65–73 (2003).
Lung Cancer, Fourth Edition, (ed. Roth, J. A., Kong, W. H., Komaki, R. U.) John (Wiley&Sons, Inc. 2014).
Pelengaris, S., Khan, M. In The Molecular Biology of Cancer (eds. Pelengaris, S., Khan, M.) (Wiley-Blackwell, 2013).
Herbst, R. S., Heymach, J. V. & Lippman, S. M. Lung Cancer. N. Engl. J. Med. 359, 1367–1380 (2008).
Garbett, N. C., Miller, J. J., Jenson, A. B. & Chaires, J. B. Calorimetric Analysis of the Plasma Proteome. Semin Nephrol. 27, 621–6 (2007).
Garbett, N. C., Miller, J. J., Jenson, A. B. & Chaires, J. B. Calorimetry outside the box: a new window into the plasma proteome. Biophys. J. 94, 1377–1383 (2008).
Garbett, N. C., Mekmaysy, C. S., Helm, C. W., Jenson, A. B. & Chaires, J. B. Differential scanning calorimetry of blood plasma for clinical diagnosis and monitoring. Exp. Mol. Pathol. 86, 186–191 (2009).
Garbett, N. C., Mekmaysy, C. S., DeLeeuw, L. & Chaires, J. B. Clinical application of plasma thermograms. Utility, practical approaches and considerations. Methods 15, 41–50 (2015).
Todinova, S., Krumova, S., Radoeva, R., Gartcheva, L. & Taneva, S. G. Calorimetric markers of Bence Jones and nonsecretory multiple myeloma serum proteome. Anal. Chem. 86, 12355–12361 (2014).
Barcelo, F. et al. Characterization of Monoclonal Gammopathy of Undetermined Significance by Calorimetric Analysis of Blood Serum Proteome, PLoS ONE 10, doi:e0120316, 1–15 (2015).
Krumova, S. et al. Calorimetric monitoring of the serum proteome in schizophrenia patients. Thermochim Acta 572, 59–64 (2013).
Todinova, S., Krumova, S., Gartcheva, L., Robeerst, C. & Taneva, S. G. Microcalorimetry of blood serum proteome: a modified interaction network in the multiple myeloma case. Anal Chem. 83, 7992–8 (2011).
Góralski, P. et al. The differences in thermal profiles between normal and leukemic cells exposed to anticancer drug evaluated by differential scanning calorimetry. J Therm Anal Calorim 118, 1339–44 (2014).
Michnik, A. et al. Differential scanning calorimetry study of blood serum in chronic obstructive pulmonary disease. J Therm Anal Calorim. 102, 57–60 (2010).
Zapf, I. et al. DSC analysis of human plasma in breast cancer patients. Thermochim Acta 524, 88–91 (2011).
Michnik, A. et al. DSC serum profiles of sportsmen. J Therm Anal Calorim 113, 365–70 (2013).
Michnik, A. et al. Delayed effects of neutron radiation on human serum In vitro DSC study. J Therm Anal Calorim 126, 37–45 (2016).
Moezzi, M., Fekecs, T., Nedvig, K., Lőrinczy, D. & Ferencz, A. Differential scanning calorimetry (DSC) analysis of human plasma in different psoriasis stages. J Therm Anal Calorim 123, 2029–2035 (2016).
Ferencz, A., Zapf, I. & Lőrinczy, D. Harmful effect of neoadjuvant chemotherapy monitoring by DSC on breast cancer patients’ blood plasma. J Therm Anal Calorim 126, 55–59 (2016).
Vega, S., Garcia-Gonzalez, M. A., Lanas, A., Velazquez-Campoy, A. & Abian, O. Deconvolution Analysis for Classifying Gastric Adenocarcinoma Patients Based on Differential Scanning Calorimetry Serum Thermograms. Sci. Rep. 5, 7988, https://doi.org/10.1038/srep07988 (2015).
Acknowledgements
This work was supported by National Science Center (grant Sonata Bis 6 DEC-2016/22/E/ST4/00446).
Author information
Authors and Affiliations
Contributions
I.C. monitored the lung cancer patients and provided the blood samples. A.M. and K.K. carried out the DSC experiments. A.M. performed statistical analysis. K.K. and P.Z. wrote the manuscript. All authors contributed to the research design, data analysis and approved the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kędra-Królik, K., Chmielewska, I., Michnik, A. et al. Blood Serum Calorimetry Indicates the Chemotherapeutic Efficacy in Lung Cancer Treatment. Sci Rep 7, 16796 (2017). https://doi.org/10.1038/s41598-017-17004-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-17004-x
This article is cited by
-
Investigation the efficacy of antipsoriatic drugs by blood plasma thermoanalysis
Journal of Thermal Analysis and Calorimetry (2023)
-
Comparison of human blood serum DSC profiles in aqueous and PBS buffer solutions
Journal of Thermal Analysis and Calorimetry (2022)
-
Comparison of deconvoluted plasma DSC curves on patients with solid tumors
Journal of Thermal Analysis and Calorimetry (2020)
-
Modification of blood serum DSC profiles by sauna treatments in cross-country skiers during the exercise cycle
Journal of Thermal Analysis and Calorimetry (2020)
-
Whole-body cryostimulation impact on blood serum thermal denaturation profiles of cross-country skiers
Journal of Thermal Analysis and Calorimetry (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
