
Abstract
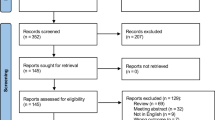
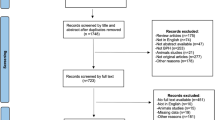
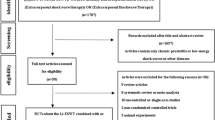
The aim of this study is to present a summary of current evidence concerning the various treatments in the management of penile rehabilitation after radical prostatectomy (RP) and provide recommendations for future research. Randomized controlled trials (RCTs) were identified from electronic databases including PubMed, the Cochrane Library, Embase, and Web of Science from inception through March 2020 with no limitation to language. Comparable data from each study were combined in a meta-analysis where possible, otherwise data were synthesized narratively. The data analysis was completed by Review Manager version 5.3. A total of 39 RCTs were included in this study. At present, phosphodiesterase type 5 inhibitors (PDE5is) remain the first-line treatment for patients with erectile dysfunction (ED) after RP. Compared with the placebo group, patients in regular PDE5is group (mean difference (MD): 0.76; 95% confidence interval (CI): 1.69–4.44; p < 0.0001) and on demand group (MD: 3.92; 95% CI: 2.95–4.88; p < 0.00001) had a significantly higher mean Erectile Function domain of the International Index of Erectile Function (IIEF-EF) scores within 3 months after RP. As for the proportion of IIEF-EF ≥ 22, patients in regular PDE5is group and on demand PDE5is group had significantly higher proportion than those in placebo group 6 months after RP, and the odds ratios were 1.87 (95% CI: 1.32–2.66; p = 0.0005) and 2.17 (95% CI: 1.20–3.93; p = 0.01), respectively. No significant difference was observed between regular PDE5is group and on demand group regardless of mean IIEF-EF score or the proportion of IIEF-EF ≥ 22. Intracorporeal injection therapy seemed to have similar efficacy to PDE5is. The International Index of Erectile Function—5 items (IIEF-5) scores were significantly higher in vacuum constriction devices group than control group at 6–9 months after RP (MD: 6.70, 95% CI: 2.30–11.10, p = 0.003) with great between-study heterogeneity (p = 0.06, I2 = 72%). The other therapeutics including low-intensity extracorporeal shockwave therapy, statin therapy, psychotherapy interventions, and pelvic floor muscle training plus electrical stimulation showed certain improvement on erectile function. We found that the combination therapy showed certain advantages over monotherapy. Currently, PDE5is-based combination therapy remains the mainstream treatment for ED after RP. Intracorporeal injection therapy and vacuum therapy could be served as alternative treatments if PDE5is are ineffective and contraindicated.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 8 print issues and online access
$259.00 per year
only $32.38 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout






Similar content being viewed by others
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Hamdy FC, Donovan JL, Lane JA, Mason M, Metcalfe C, Holding P, et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl J Med. 2016;375:1415–24.
Mottet N, Cornford P, van den Bergh RCN, Briers E, De Santis M, Fanti S, et al. EAU guidelines on prostate cancer. https://uroweb.org/guideline/prostate-cancer/#note_353. Accessed date 2020.
Ficarra V, Novara G, Ahlering TE, Costello A, Eastham JA, Graefen M, et al. Systematic review and meta-analysis of studies reporting potency rates after robot-assisted radical prostatectomy. Eur Urol. 2012;62:418–30.
Sivarajan G, Prabhu V, Taksler GB, Laze J, Lepor H. Ten-year outcomes of sexual function after radical prostatectomy: results of a prospective longitudinal study. Eur Urol. 2014;65:58–65.
Nelson CJ, Scardino PT, Eastham JA, Mulhall JP. Back to baseline: erectile function recovery after radical prostatectomy from the patients’ perspective. J Sex Med. 2013;10:1636–43.
Montorsi F, Guazzoni G, Strambi LF, Da Pozzo LF, Nava L, Barbieri L, et al. Recovery of spontaneous erectile function after nerve-sparing radical retropubic prostatectomy with and without early intracavernous injections of alprostadil: results of a prospective, randomized trial. J Urol. 1997;158:1408–10.
Laurienzo CE, Magnabosco WJ, Jabur F, Faria EF, Gameiro MO, Sarri AJ, et al. Pelvic floor muscle training and electrical stimulation as rehabilitation after radical prostatectomy: a randomized controlled trial. J Phys Ther Sci. 2018;30:825–31.
Geraerts I, Van Poppel H, Devoogdt N, De Groef A, Fieuws S, Van Kampen M. Pelvic floor muscle training for erectile dysfunction and climacturia 1 year after nerve sparing radical prostatectomy: a randomized controlled trial. Int J Impot Res. 2016;28:9–13.
de Lira GHS, Fornari A, Cardoso LF, Aranchipe M, Kretiska C, Rhoden EL. Effects of perioperative pelvic floor muscle training on early recovery of urinary continence and erectile function in men undergoing radical prostatectomy: a randomized clinical trial. Int Braz J Urol. 2019;45:1196–203.
Oh JJ, Kim JK, Lee H, Lee S, Jin Jeong S, Kyu, Hong S, et al. Effect of personalized extracorporeal biofeedback device for pelvic floor muscle training on urinary incontinence after robot-assisted radical prostatectomy: a randomized controlled trial. Neurourol Urodyn. 2020;39:674–81.
Karlsen RV, E Bidstrup P, Hvarness H, Bagi P, Friis Lippert E, Permild R, et al. Feasibility and acceptability of couple counselling and pelvic floor muscle training after operation for prostate cancer. Acta Oncol. 2017;56:270–7.
Aydogdu O, Gokce MI, Burgu B, Baltacı S, Yaman O. Tadalafil rehabilitation therapy preserves penile size after bilateral nerve sparing radical retropubic prostatectomy. Int Braz J Urol. 2011;37:336–44.
Kim DJ, Hawksworth DJ, Hurwitz LM, Cullen J, Rosner IL, Lue TF, et al. A prospective, randomized, placebo-controlled trial of on-demand vs. nightly sildenafil citrate as assessed by Rigiscan and the International Index of Erectile Function. Andrology. 2016;4:27–32.
Montorsi F, Brock G, Lee J, Shapiro J, Van Poppel H, Graefen M, et al. Effect of nightly versus on-demand vardenafil on recovery of erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol. 2008;54:924–31.
Brock G, Nehra A, Lipshultz LI, Karlin GS, Gleave M, Seger M, et al. Safety and efficacy of vardenafil for the treatment of men with erectile dysfunction after radical retropubic prostatectomy. J Urol. 2003;170:1278–83.
Montorsi F, Brock G, Stolzenburg JU, Mulhall J, Moncada I, Patel HR, et al. Effects of tadalafil treatment on erectile function recovery following bilateral nerve-sparing radical prostatectomy: a randomised placebo-controlled study (REACTT). Eur Urol. 2014;65:587–96.
Padma-Nathan H, McCullough AR, Levine LA, Lipshultz LI, Siegel R, Montorsi F, et al. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res. 2008;20:479–86.
Pavlovich CP, Levinson AW, Su LM, Mettee LZ, Feng Z, Bivalacqua TJ, et al. Nightly vs on-demand sildenafil for penile rehabilitation after minimally invasive nerve-sparing radical prostatectomy: results of a randomized double-blind trial with placebo. BJU Int. 2013;112:844–51.
Bannowsky A, van Ahlen H, Loch T. Increasing the dose of vardenafil on a daily basis does not improve erectile function after unilateral nerve-sparing radical prostatectomy. J Sex Med. 2012;9:1448–53.
Canat L, Güner B, Gürbüz C, Atış G, Çaşkurlu T. Effects of three-times-per-week versus on-demand tadalafil treatment on erectile function and continence recovery following bilateral nerve sparing radical prostatectomy: results of a prospective, randomized, and single-center study. Kaohsiung J Med Sci. 2015;31:90–95.
Montorsi F, Nathan HP, McCullough A, Brock GB, Broderick G, Ahuja S, et al. Tadalafil in the treatment of erectile dysfunction following bilateral nerve sparing radical retropubic prostatectomy: a randomized, double-blind, placebo controlled trial. J Urol. 2004;172:1036–41.
Mulhall JP, Burnett AL, Wang R, McVary KT, Moul JW, Bowden CH, et al. A phase 3, placebo controlled study of the safety and efficacy of avanafil for the treatment of erectile dysfunction after nerve sparing radical prostatectomy. J Urol. 2013;189:2229–2236.
Pace G, Del Rosso A, Vicentini C. Penile rehabilitation therapy following radical prostatectomy. Disabil Rehabil. 2010;32:1204–8.
Raina R, Agarwal A, Ausmundson S, Lakin M, Nandipati KC, Montague DK, et al. Early use of vacuum constriction device following radical prostatectomy facilitates early sexual activity and potentially earlier return of erectile function. Int J Impot Res. 2006;18:77–81.
Köhler TS, Pedro R, Hendlin K, Utz W, Ugarte R, Reddy P, et al. A pilot study on the early use of the vacuum erection device after radical retropubic prostatectomy. BJU Int. 2007;100:858–62.
Engel JD. Effect on sexual function of a vacuum erection device post-prostatectomy. Can J Urol. 2011;18:5721–5.
Hu Dingan, Hu Mengzhong, Zhao Juping, Shen Zhoujun. Efficacy and safety of vacuum erection device in the treatment of erectile dysfunction after radical prostatectomy. Chin J Hum Sexuality. 2014;23:14–16.
Liu T, Chen XG. Clinical diagnosis and treatment of erectile dysfunction after radical prostatectomy. Chin J Hum Sexuality. 2016;25:10–3.
Molton IR, Siegel SD, Penedo FJ, Dahn JR, Kinsinger D, Traeger LN, et al. Promoting recovery of sexual functioning after radical prostatectomy with group-based stress management: the role of interpersonal sensitivity. J Psychosom Res. 2008;64:527–36.
Siddons HM, Wootten AC, Costello AJ. A randomised, wait-list controlled trial: evaluation of a cognitive-behavioural group intervention on psycho-sexual adjustment for men with localised prostate cancer. Psychooncology. 2013;22:2186–92.
Haahr MK, Harken Jensen C, Toyserkani NM, Andersen DC, Damkier P, Sørensen JA, et al. A 12-month follow-up after a single intracavernous injection of autologous adipose-derived regenerative cells in patients with erectile dysfunction following radical prostatectomy: an open-label phase I clinical trial. Urology. 2018;121:203.e6–203.e13.
Yiou R, Hamidou L, Birebent B, Bitari D, Le Corvoisier P, Contremoulins I, et al. Intracavernous injections of bone marrow mononucleated cells for postradical prostatectomy erectile dysfunction: final results of the INSTIN clinical trial. Eur Urol Focus. 2017;3:643–5.
Yiou R, Hamidou L, Birebent B, Bitari D, Lecorvoisier P, Contremoulins I, et al. Safety of intracavernous bone marrow-mononuclear cells for postradical prostatectomy erectile dysfunction: an open dose-escalation pilot study. Eur Urol. 2016;69:988–91.
Baccaglini W, Pazeto CL, Corrêa Barros EA, Timóteo F, Monteiro L, Saad Rached RY, et al. The role of the low-intensity extracorporeal shockwave therapy on penile rehabilitation after radical prostatectomy: a randomized clinical trial. J Sex Med. 2020;17:688–94.
Mulhall JP, Klein EA, Slawin K, Henning AK, Scardino PT. A randomized, double-blind, placebo-controlled trial to assess the utility of tacrolimus (FK506) for the prevention of erectile dysfunction following bilateral nerve-sparing radical prostatectomy. J Sex Med. 2018;15:1293–9.
Chiles KA, Staff I, Johnson-Arbor K, Champagne A, McLaughlin T, Graydon RJ. A double-blind, randomized trial on the efficacy and safety of hyperbaric oxygenation therapy in the preservation of erectile function after radical prostatectomy. J Urol. 2018;199:805–11.
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. 2015;4:1.
Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A. The international index of erectile function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology. 1997;49:822–30.
Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Pena BM. Development and evaluation of an Abridged 5-Item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11:319–26.
Evidence-Based Cf. Oxford Centre for evidence-based medicine: levels of evidence, 2009. http://www.cebm.net/oxford-centreevidence-based-medicine-levels-evidence-march-2009/.
Glazener C, Boachie C, Buckley B, Cochran C, Dorey G, Grant A, et al. Urinary incontinence in men after formal one-to-one pelvic-floor muscle training following radical prostatectomy or transurethral resection of the prostate (MAPS): two parallel randomized controlled trials. Lancet. 2011a;378:328–37.
Lin YH, Yu TJ, Lin VC, Wang HP, Lu K. Effects of early pelvic-floor muscle exercise for sexual dysfunction in radical prostatectomy recipients. Cancer Nurs. 2012;35:106–14.
Prota C, Gomes CM, Ribeiro LH, de Bessa J Jr, Nakano E, Dall’Oglio M, et al. Early postoperative pelvic-floor biofeedback improves erectile function in men undergoing radical prostatectomy: a prospective, randomized, controlled trial. Int J Impot Res. 2012;24:174–8.
Fode M, Borre M, Ohl DA, Lichtbach J, Sønksen J. Penile vibratory stimulation in the recovery of urinary continence and erectile function after nerve-sparing radical prostatectomy: arandomized, controlled trial. BJU Int. 2014;114:111–7.
Frey A, Sonksen J, Fode M. Low-intensity extracorporeal shockwave therapy in the treatment of postprostatectomy erectile dysfunction: a pilot study. Scand J Urol. 2016;50:123–7.
Huber J, Ihrig A, Yass M, Bruckner T, Peters T, Huber CG, et al. Multimedia support for improving preoperative patient education: a randomized controlled trial using the example of radical prostatectomy. Ann Surg Oncol. 2013;20:15–23.
Robertson J, McNamee P, Molloy G, Hubbard G, McNeill A, Bollina P, et al. Couple-based psychosexual support following prostate cancer surgery: results of a feasibility pilot randomized control trial. J Sex Med. 2016;13:1233–42.
Naccarato AM, Reis LO, Ferreira U, Denardi F. Psychotherapy and phosphodiesterase-5 inhibitor in early rehabilitation after radical prostatectomy: a prospective randomised controlled trial. Andrologia. 2016;48:1183–7.
McCullough AR, Hellstrom WG, Wang R, Lepor H, Wagner KR, Engel JD. Recovery of erectile function after nerve sparing radical prostatectomy and penile rehabilitation with nightly intraurethral alprostadil versus sildenafil citrate. J Urol. 2010;183:2451–6.
Kostis JB, Dobrzynski JM. The effect of statins on erectile dysfunction: a meta-analysis of randomized trials. J Sex Med. 2014;11:1626–35.
Cui Y, Zong H, Yan H, Zhang Y. The effect of statins on erectile dysfunction: a systematic review and meta-analysis. J Sex Med. 2014;11:1367–75.
Siltari A, Riikonen J, Fode M, Murtola TJ. Effects of preoperative atorvastatin treatment on erectile function after radical prostatectomy: results from a subgroup of ESTO1, a randomized, double-blind, placebo-controlled study. J Sex Med. 2019;16:1597–605.
Liao JK, Laufs U. Pleiotropic effects of statins. Annu Rev Pharm Toxicol. 2005;45:89–118.
Hong SK, Han BK, Jeong SJ, Byun SS, Lee SE. Effect of statin therapy on early return of potency after nerve sparing radical retropubic prostatectomy. J Urol. 2007;178:613–6.
McCorkle R, Seifert ML, Dowd MF, Robinson JP, Pickett M. Effects of advanced practice nursing on patient and spouse depressive symptoms, sexual function, and marital interaction after radical prostatectomy. Urol Nurs. 2007;27:65–77.
Nelson CJ, Saracino RM, Napolitano S, Pessin H, Narus JB, Mulhall JP. Acceptance and commitment therapy to increase adherence to penile injection therapy-based rehabilitation after radical prostatectomy: pilot randomized controlled trial. J Sex Med. 2019;16:1398–408.
Kim N, Vardi Y, Padma-Nathan H, Daley J, Goldstein I, Saenz de Tejada I. Oxygen tension regulates the nitric oxide pathway physiological role penile erection. J Clin Invest. 1993;91:437–42.
Blecher G, Almekaty K, Kalejaiye O, Minhas S. Does penile rehabilitation have a role in the treatment of erectile dysfunction following radical prostatectomy? F1000Res. 2017;6:1923.
Walz J, Graefen M, Huland H. Surgical anatomy of the prostate in the era of radical robotic prostatectomy. Curr Opin Urol. 2011;21:173–8.
Mulhall J, Bivalacqua T, Becher E. Standard operating procedure for the preservation of erectile function outcomes after radical prostatectomy. J Sex Med. 2013;10:195–203.
Champion H, Abdel-Mageed A, Hellstrom W. Cavernous neurotomy causes hypoxia and fibrosis in rat corpus cavernosum. J Androl. 2003;24:239–45.
Clavell-Hernandez J, Ermeç B, Kadıoğlu A, Wang R. Perplexity of penile rehabilitation following radical prostatectomy. Turk J Urol. 2019;45:77–82.
Wang R. Penile rehabilitation after radical prostatectomy: where do we stand and where are we going? J Sex Med. 2007;4:1085–97.
Salonia A, Burnett AL, Graefen M, Hatzimouratidis K, Montorsi F, Mulhall JP, et al. Prevention and management of postprostatectomy sexual dysfunctions. Part 1: Choosing the right patient at the right time for the right surgery. Eur Urol. 2012;62:261–72.
Nguyen LN, Head L, Witiuk K, Punjani N, Mallick R, Cnossen S, et al. The risks and benefits of cavernous neurovascular bundle sparing during radical prostatectomy: a systematic review and meta-analysis. J Urol. 2017;198:760–9.
Du Y, Long Q, Guan B, Mu L, Tian J, Jiang Y, et al. Robot-assisted radical prostatectomy is more beneficial for prostate cancer patients: a system review and meta-analysis. Med Sci Monit. 2018;24:272–87.
Lafaye A, Petit S, Richaud P, Houédé N, Baguet F, Cousson-Gélie F. Dyadic effects of coping strategies on emotional state and quality of life in prostate cancer patients and their spouses. Psychooncology. 2014;23:797–803.
Zisman A, Leibovici D, Kleinmann J, Siegel YI, Lindner A. The impact of prostate biopsy on patient well-being: a prospective study of pain, anxiety and erectile dysfunction. J Urol. 2001;166:2242–6.
Xu P, Wang Y-H. Prevention and treatment of erectile dysfunction after prostatectomy: an update. Zhonghua Nan Ke Xue Za Zhi. 2017;23:656–62.
Mulhall JP, Parker M, Waters BW, Flanigan R. The timing of penile rehabilitation after bilateral nerve-sparing radical prostatectomy affects the recovery of erectile function. BJU Int. 2010;105:37–41.
Author information
Authors and Affiliations
Contributions
Conception and design: DCF. Administrative support: WRW. Provision of study materials or patients, collection and assembly of data, data analysis and interpretation: DCF and CT. Manuscript writing and final approval of manuscript: all authors.
Corresponding author
Ethics declarations
Conflict of interest
The study was supported by the 1.3.5 project for disciplines of excellence, West China Hospital, Sichuan University (ZY2016104) and Pillar Program from Department of Science and Technology of Sichuan Province (2018SZ0219). The funders had no role in study design, data collection or analysis, preparation of the manuscript, or the decision to publish. The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Feng, D., Tang, C., Liu, S. et al. Current management strategy of treating patients with erectile dysfunction after radical prostatectomy: a systematic review and meta-analysis. Int J Impot Res 34, 18–36 (2022). https://doi.org/10.1038/s41443-020-00364-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41443-020-00364-w
This article is cited by
-
Vacuum erection device for erectile function rehabilitation after radical prostatectomy: which is the correct schedule? Results from a systematic, scoping review
International Journal of Impotence Research (2024)
-
Comment on: Comparison of the efficacy of the early LI-SWT plus daily tadalafil with daily tadalafil only as penile rehabilitation for postprostatectomy erectile dysfunction
International Journal of Impotence Research (2023)
-
Indocyanine green fluorescence is an innovative and practical intra-operative identification tool: latest updates from the 38th annual European association of urology congress (EAU2023)
World Journal of Urology (2023)
-
The use of combination regenerative therapies for erectile dysfunction: rationale and current status
International Journal of Impotence Research (2022)
