
Abstract
Purpose
To report the contribution to carbon dioxide equivalent mass [CO2EM] of various types of VR surgery performed across three tertiary referral centres, according to their indication and fluorinated gas used. We secondarily reported on the difference in tamponade choice, and CO2EM between the different centres.
Materials
Retrospective, continuous, comparative multicentre study of all procedures using fluorinated gases between 01/01/17-31/12/20 at the Manchester Royal Eye Hospital and Birmingham and Midland Eye Centre, and between 01/01/19-31/12/2020 at the University Hospitals Coventry and Warwickshire.
Results
Across 4877 procedures, the use of fluorinated gases produced 284.2 tonnes (71.2 tonnes annually) CO2EM; an annual consumption of 30,330 l of gasoline. Rhegmatogenous-retinal-detachment (RRD) and macular hole repair had the highest CO2EM by indication, accounting for 191.4 tonnes CO2EM (67.3%) and 28.6 tonnes CO2EM (10.1%); a mean 60.0 kg and 32.0 kg of CO2EM produced per surgery respectively. The use of fluorinated gases and their respective CO2EM contributions were significantly different across all three centres (p < 0.001) for all indications. SF6, despite being used in 1883 procedures (38.6%), contributed to 195.5 tonnes CO2EM (68.8%). Relative to C2F6, procedures using C3F8 and SF6 produced 1.9 and 4.4 times more CO2EM.
Conclusion
We demonstrated that SF6 causes significantly higher carbon emissions relative to C2F6 and C3F8 with RRD and macular hole repair having the greatest environmental impact. We also reported large variations between different large VR centres in fluorinated gas use, and therefore in carbon emission contributions depending on indications for surgery. Evidence-based protocols might help in making VR surgery “greener”.
Similar content being viewed by others
Introduction
Sulphur hexafluoride (SF6), hexafluoroethane (C2F6) and octafluoropropane (C3F8) are the fluorinated gases commonly used in vitreoretinal (VR) surgery and they are among the most potent greenhouse gases. They have much longer atmospheric lifetimes than CO2 (Table 1, adapted from the Intergovernmental Panel on Climate Change (IPCC) second assessment report) with 1 kg of SF6 having a global warming potential (GWP) of 23,900 kg of CO2 (Table 1) over 100 years (GWP100) [1,2,3]. GWP represents the amount of heat absorbed by a greenhouse gas, as a multiple of the equivalent heat, that would be absorbed by the same mass of CO2 [1]. SF6 has also been identified in the Kyoto Protocol as one of six gases which require strict regulation in order to reduce global warming [4].
This research group has previously published that the fluorinated gas use in VR surgery is contributing to 0.11% of annual SF6 use in the United Kingdom (UK) across all industries [3].
The National Health Service (NHS) produces 5.4% of annual greenhouse gases in the UK, despite being committed to becoming carbon neutral by 2040 [5].
In this paper we aimed to investigate the contribution to carbon emissions of various types of VR surgery performed across three tertiary referral centres, according to their indication. We secondarily reported on the difference in tamponade choice, and therefore carbon emissions between the different centres and the surgeons involved.
Methods
This is a retrospective, continuous, comparative multicentre study of all fluorinated gas use in vitreoretinal surgery for different indications. This study was conducted at the Manchester Royal Eye Hospital (MREH), the Birmingham and Midland Eye Centre (BMEC) (the second and third largest eye hospitals in the UK), and the University Hospitals Coventry and Warwickshire (UHCW). We included all VR surgeries involving fluorinated gases at MREH and BMEC over four years, between 1st January 2017 to the 31st December 2020. For UHCW, data were available for consecutive cases of a single surgeon (DYP) over a two-year period, from the 1st of January 2019 to the 31st of December 2020.
Data acquisition
For MREH, data were extracted from a centralised database of all VR procedures performed, recorded on Microsoft Access. For BMEC, data were acquired from the electronic patient records (EPR, Medisoft Ophthalmology, Medisoft Limited, Leeds, UK). Finally, UHCW data were taken from DYP’s surgical logbook.
Surgeries were divided according to common VR surgical indications: rhegmatogenous retinal detachment (RRD), macular hole repair, diabetic retinopathy (including segmentation, delamination, and diabetic vitreous haemorrhage), haemorrhagic posterior vitreous detachment (PVD), other causes of vitreous haemorrhage, epiretinal membrane peel, sub-macular haemorrhage and other (any procedure that does not fit into any of the categories indicated).
All air tamponade cases were excluded, and this study looks exclusively at procedures that used fluorinated gases.
Environmental factor calculations
The environmental aspect of gas tamponade was performed by converting millilitre of gas to mass (g) using the modified ideal law gas formula at standard temperature and pressure (STP). Intraocular gas masses were then converted to their GWP100 [6]. The respective GWP100 values were used: SF6: 23,500, C2F6: 11,100 and C3F8: 8900, as per the fifth IPCC report [7]. The CO2 equivalent mass (CO2EM) was then calculated. For example, if a 75 ml canister of SF6 was used per surgery, 75 ml of SF6 was converted to the equivalent of 0.4887 g at STP [6], and multiplied by the GWP100 of 23,500 to be around 11,500 g (11.5 kg) of CO2EM.
Context was given to CO2 emissions using a greenhouse gas equivalencies calculator by the United States Environmental Protection Agency (EPA) [8]. This calculator converts CO2EM, which is an arbitrary value to most readers, to give context to the user, such as how many miles driven, mobile phone charges, or litres of gasoline used are a certain number of tonnes of CO2 equivalent to. While helpful in conceptualising the mass of CO2, this calculator will depend on the conversion factors used, which are not published. For example, cars in the US may have higher fuel consumption than the UK and so their calculations may not be fully reflective for certain populations.
Our full environmental factor methodology can be found in this prior publication that includes a calculator to allow accessibility to perform similar calculations [3, 6]. In summary, all three centres utilise different gas delivery systems. Total fluorinated gas use was calculated by accessing pharmaceutical orders and gas that was not used by expiry date (as was the case with cylinder delivery systems) was counted towards total fluorinated gas use.
Surgical method
This study encapsulates a wide range of surgical procedures across multiple surgeons, with 23 G, 25 G and 27 G Pars Plana Vitrectomy (PPV) used routinely in our study duration. Tamponade choice was at the discretion of the operator.
Statistical analysis
Statistical significance was defined as p < 0.05. Mann–Whitney U and Kruskal–Wallis Test were used to compare two and three independent continuous variables, respectively. Fisher exact test and Chi-Squared test were used for nominal variables. All statistical analysis was performed using IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp, Armonk NY).
Ethical approval/consent to participation
As this was a retrospective anonymized study, as per our local protocol from our Clinical Effectiveness Department, and as per national guidelines from the National Code of Clinical Research, and the Health Research Authority (HRA), this study has ethical approval exemption and no patient consent was required for participation [9, 10]. All procedures were completed prior to the design of this study. Patients were diagnosed and treated according to local guidelines and agreements and written consent from patients was acquired prior to all procedures as clinically indicated. This study does not report on the use of new or experimental protocols.
Results
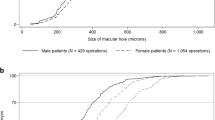
We included 4877 VR surgeries [3]. RRD, followed by macular hole repair were the most common indications for surgery (Fig. 1). Over the study period, the three centres contributed to 284.2 tonnes of CO2EM which equates to 71.2 tonnes of CO2EM annually due to the use of fluorinated gases. This corresponds to an annual consumption of 30,330 l of gasoline [8].

The total equivalent mass of CO2 over four years (A) show that SF6 contributes the highest proportion of the fluorinated gases in carbon emissions. This is evident by comparing against the number of procedures performed by each fluorinated gas (B). SF6 was used in 38.6% of procedures (B) but contributed to 68.8% of emissions (A).
The two major contributors of emissions were RRD and macular hole surgery. RRD was responsible for the highest fluorinated gas use accounting for 191.4 tonnes CO2EM (67.3%), followed by macular hole repair with 28.6 tonnes CO2EM (10.1%). This corresponds to 60.0 kg and 32.0 kg of CO2EM produced per surgery for RRD and macular hole, respectively. Figure 1A demonstrates the CO2EM contributed by each gas tamponade by surgical indication while Fig. 1B shows the number of procedures performed with each respective tamponade. SF6, despite being used in only 1883 procedures (38.6% of the total), contributed to 195.5 tonnes CO2EM (68.8% of the total). We found that SF6, C3F8 and C2F6 use resulted in 103.8 kg CO2EM, 44.1 kg CO2EM and 23.4 kg CO2EM per procedure, respectively. Relative to C2F6, procedures using C3F8 and SF6 produced 1.9 and 4.4 times more CO2EM.
We also explored the differences in fluorinated gas use between the three centres and their respective contributions to CO2EM (Fig. 2). For RRD repair, MREH used SF6 in 880 (55.3% of the total RDD cases) surgeries while UHCW utilised SF6 in only 24 (21.4%) of cases.

Chi-Squared test utilised between groups. Significant differences were found for every indication in tamponade contribution to equivalent CO2 emissions across the different institutions. UHCW did use any fluorinated gas for vitreous haemorrhage or ERM.
UHCW additionally did not use any fluorinated gas for ERM or haemorrhagic PVD surgery. The use of fluorinated gases and their respective CO2EM contributions were significantly different across all three centres (p < 0.001) for all indications.
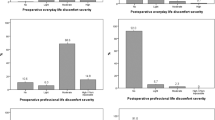
The total contributions of CO2EM from each centre and the fluorinated gases use are summarised in Table 2. MREH had the highest CO2EM production from SF6 accounting for 70.2% of total CO2EM compared to UHCW at 40.0%. C2F6 accounted for 52.3% of CO2EM for UHCW relative to MREH at 16.6%. At BMEC 25.2% of the total CO2EM originated from C3F8 compared to 7.7% at UHCW. Figure 3 compares the contribution to CO2EM according to indication for VR surgery by centre.

The relative contributions of each centre to CO2 emissions by indication.
Discussion
In this study we reported how different indications in VR surgery and tamponade preference affect CO2EM. While we found that RRD and macular hole are the two largest contributors to carbon emissions from fluorinated gas use, we also demonstrated the importance of type of tamponade choice on CO2EM (Fig. 1A, B) with SF6 having a 4.4 greater environmental impact than C2F6.
Our data showed significant differences in choice of tamponade between centres and among surgeons. This is multifactorial and complex decision. Local guidelines, and prior training have a significant impact on the surgeon’s choice of tamponade. In addition, concerning RRD, previous studies have shown that the training level of a VR surgeon [11], as well as the patients’ ethnicity and socioeconomic status, can play a role [12]. Therefore, different local populations, case complexity and the presence of VR fellows may have contributed to the differences observed between our centres. Ultimately, surgeons should use whichever gas they feel it achieves the best surgical outcome for their patient, but they should also be aware of their environmental impact. UHCW for example, used the least SF6 due to routine integration of air tamponade in RRD repair, without detriment to their outcomes [13]. By changing their practice, UHCW had the lowest carbon emissions from fluorinated gas use in RRD repair among the centres involved in our study.
SF6, as well as being the most potent greenhouse gas known [1], also has the shortest effect relative to C2F6 and C3F8. This provides several practical advantages for surgeons and patients over the longer acting alternatives. Air tamponade as an alternative for fluorinated gases (and especially SF6) has been described for RRD [13,14,15,16,17,18,19,20,21,22,23,24,25], and even in macular hole repair [26]. If air tamponade is not appropriate, surgeons could also consider diluting C2F6 or C3F8 as an alternative to SF6. However, although dilute concentrations of C2F6/C3F8 can be titrated to have the same duration gas bubble as SF6, the bubble volume will not be the same for all three gases and this will impact tamponade effect.
Although ophthalmology causes a relatively small contribution to CO2 emissions across the whole of medicine, this manuscript highlights a topic that is not often discussed. With climate change becoming an increasingly important issue, VR surgeons should be aware of the environmental impact of their surgery, and similar efforts are being made across other medical specialities [27,28,29]. Due to the wide variety in tamponade choice in VR surgery, evidence-based departmental protocols may provide environmentally friendlier surgery, without a detrimental effect on patients’ safety.
Study limitations and strengths
This is a retrospective study with no agreed protocol for gas tamponade choice for case indication and complexity. In addition, although fluorinated gases have significant CO2EM due to their high GWP100 values, they represent just a small part of the carbon emissions in VR surgery, with other hospital and patient factors such as the type of anaesthesia and the frequency of follow up visits, causing a significant environmental impact. Nevertheless, this large study reflects real-life environmental consequences of fluorinated gas use for different surgical indications at large VR centres in the UK.
Conclusions
In this study we demonstrated that SF6 causes significantly higher carbon emissions relative to C2F6 and C3F8 with RRD and macular hole repair having the greatest environmental impact. We also reported large variations between different large VR centres in fluorinated gas use, and therefore in carbon emission contributions depending on indications for surgery. Evidence-based protocols might help in making VR surgery “greener”.
Summary
What was known before
-
The fluorinated gases used in vitreoretinal (VR) surgery, are the most potent greenhouse gases in existence.
-
Large variability exists in the use of fluorinated gases across different clinicians.
What this study adds
-
A multicentre study to realise the environmental impact of fluorinated gases across different indications.
-
Variability in tamponade choice significantly affects the environmental carbon footprint of VR surgery.
Data availability
The raw data are available upon reasonable request
References
IPCC. IPCC Fourth Assessment Report (AR4), Working Group 1. Chapter 2, Changes in atmospheric constituents and in radiative forcing. Intergovernmental Panel on Climate Change (IPCC); 2007.
IPCC. Climate change 1995: The IPCC Second Assessment Report. Intergovernmental Panel on Climate Change (IPCC);1995.
Moussa G, Ch’ng SW, Park DY, Ziaei H, Jalil A, Patton N, et al. Environmental effect of fluorinated gases in vitreoretinal surgery: a multicenter study of 4,877 patients. Am J Ophthalmol. 2021. http://www.ajo.com/article/S0002939421004773/fulltext.
UNFCCC. What is the Kyoto Protocol? United Nations Climate Change. 2020. https://unfccc.int/kyoto_protocol. Accessed 5 January 2022.
England N NHS becomes the world’s first national health system to commit to become ‘carbon net zero’, backed by clear deliverables and milestones. 2020. https://www.england.nhs.uk/2020/10/nhs-becomes-the-worlds-national-health-system-to-commit-to-become-carbon-net-zero-backed-by-clear-deliverables-and-milestones/.
Moussa G, Ch’ng SW, Park DY, Ziaei H, Jalil A, Patton N, et al. Environmental effect of fluorinated gases in vitreoretinal surgery: a multicenter study of 4,877 patients. American Journal of Ophthalmology. 2021.
IPCC. Climate change 2014: synthesis report. Contribution of Working Groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. IPCC; 2014.
EPA - United States Environmental Protection Agency. Greenhouse Gas Equivalencies Calculator. 2021. https://www.epa.gov/energy/greenhouse-gas-equivalencies-calculator. Accessed 21 February 2021.
Kıraç FS. Is ethics approval necessary for all trials? A clear but not certain process. Malecular Imaging Radionucl Ther. 2013;22:73–75.
Health Research Authority. Do I need NHS Ethics approval? http://www.hra-decisiontools.org.uk/ethics/. Accessed 29 May 2021.
Moussa G, Kalogeropoulos D, Ch’ng SW, Lett KS, Mitra A, Tyagi AK, et al. The effect of supervision and out-of-hours surgery on the outcomes of primary macula-on retinal detachments operated by vitreoretinal fellows: a review of 435 surgeries. Ophthalmologica. 2021. https://pubmed.ncbi.nlm.nih.gov/34818241/.
Moussa G, Kalogeropoulos D, Ch’ng SW, Lett KS, Mitra A, Tyagi AK. et al. Effect of deprivation and ethnicity on primary macula-on retinal detachment repair success rate and clinical outcomes: a study of 568 patients Khetan V (ed). PLoS One. 2021;16:e0259714. https://pubmed.ncbi.nlm.nih.gov/34752493/.
Moussa G, Mathews N, Makhzoum O, Park DY. Vitrectomy with air tamponade and cryotherapy for retinal detachment repair without perfluorocarbon use: a UK 12-month prospective case series. Eur J Ophthalmol. 2020. http://journals.sagepub.com/doi/10.1177/1120672120978884.
Tan HS, Lesnik Oberstein SY, Mura M, Bijl HM. Air versus gas tamponade in retinal detachment surgery. Br J Ophthalmol. 2013;97:80–82.
Chen QY, Tang YX, He YQ, Lin HM, Gao RL, Li MY, et al. Air tamponade in retinal detachment surgery followed by ultra-widefield fundus imaging system. Int J Ophthalmol. 2018;11:1198–203.
Lin Z, Liang QH, Lin K, Hu ZX, Chen TY, Wu RH, et al. Air tamponade and without heavy liquid usage in pars plana vitrectomy for rhegmatogenous retinal detachment repair. Int J Ophthalmol. 2018;11:1779–83.
Zhang Z, Peng M, Wei Y, Jiang X, Zhang S. Pars plana vitrectomy with partial tamponade of filtered air in Rhegmatogenous retinal detachment caused by superior retinal breaks. BMC Ophthalmology. 2017;17:64.
Zhou C, Qiu Q, Zheng Z. Air versus gas tamponade in rhegmatogenous retinal detachment with inferior breaks after 23-gauge pars plana vitrectomy: a prospective, randomized comparative interventional study. Retina. 2015;35:886–91.
Tetsumoto A, Imai H, Hayashida M, Otsuka K, Matsumiya W, Miki A, et al. The comparison of the surgical outcome of 27-gauge pars plana vitrectomy for primary rhegmatogenous retinal detachment between air and SF6 gas tamponade. Eye. 2020;34:299–306.
Martínez-Castillo VJ, García-Arumí J, Boixadera A. Pars plana vitrectomy alone for the management of pseudophakic rhegmatogenous retinal detachment with only inferior breaks. Ophthalmology. 2016;123:1563–9.
Martínez-Castillo V, Boixadera A, Verdugo A, García-Arumí J. Pars Plana Vitrectomy Alone for the Management of Inferior Breaks in Pseudophakic Retinal Detachment without Facedown Position. Ophthalmology. 2005;112:1222–26.e1
Martínez-Castillo V, Verdugo A, Boixadera A, García-Arumí J, Corcóstegui B. Management of inferior breaks in pseudophakic rhegmatogenous retinal detachment with pars plana vitrectomy and air. Arch Ophthalmol. 2005;123:1078–81.
Li Y, Cheung N, Jia L, Zhang H, Liu N. Surgical outcomes of 25-Gauge pars plana vitrectomy using air as an internal tamponade for primary rhegmatogenous retinal detachment. Retina. 2020;40:2077–82.
Mateo-Montoya A, de Smet MD. Air as tamponade for retinal detachments. Eur J Ophthalmol. 2013;24:242–6.
Ruamviboonsuk P, Limwattanayingyong J, Tadarati M. Sutureless 25-gauge vitrectomy for rhegmatogenous retinal detachment caused by superior breaks using air tamponade. Asia-Pac J Ophthalmol. 2015;4:92–96.
Eckardt C, Eckert T, Eckardt U, Porkert U, Gesser C. Macular hole surgery with air tamponade and optical coherence tomography-based duration of face-down positioning. Retina. 2008;28:1087–96.
Starup‐Hansen J, Dunne H, Sadler J, Jones A, Okorie M. Climate change in healthcare: Exploring the potential role of inhaler prescribing. Pharmacology Research & Perspectives. 2020;8.
Bali T, Flesher W. BET 1: The clinical impact of policies aimed at reducing the carbon footprint of emergency departments. Emergency Medicine Journal. 2020;37:170.2-171.
Wilkinson AJK, Braggins R, Steinbach I, Smith J. Costs of switching to low global warming potential inhalers. An economic and carbon footprint analysis of NHS prescription data in England. BMJ Open. 2019;9:e028763.
Author information
Authors and Affiliations
Contributions
All authors have made substantial contributions to the following: (1) the conception and design of the study, or acquisition of data, or analysis and interpretation of data, (2) drafting the article or revising it critically for important intellectual content, (3) final approval of the version to be submitted.
Corresponding author
Ethics declarations
Competing interests
All authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Moussa, G., Ch’ng, S.W., Ziaei, H. et al. The use of fluorinated gases and quantification of carbon emission for common vitreoretinal procedures. Eye 37, 1405–1409 (2023). https://doi.org/10.1038/s41433-022-02145-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-02145-9
