
Abstract
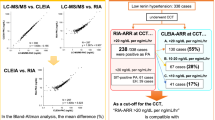
Aldosterone and renin measurement is a cornerstone for primary aldosteronism (PA) diagnosis, but different thresholds are used according to different assays. A fully automated chemiluminescence (CL) immunoassay for renin and aldosterone was recently proposed, showing good performance for PA screening by aldosterone to renin ratio (ARR). This study aimed to define the accuracy of this assay in the screening and in the most popular confirmatory test of autonomous aldosterone production, the intravenous saline loading test (ivSLT). We compared aldosterone results obtained by CL vs radioimmunoassay (RIA) in hypertensive patients investigated for PA (102 baseline and 85 after ivSLT). An excellent correlation was observed between RIA and CL in the entire population for aldosterone (r=0.922) and ARR (r=0.977). For ARR, Deming regression proved a good accordance between methods and, consistent with the fit model, our previous institutional ARR cut-off of 32 (pg ml−1)/(pg ml−1) corresponded to 20 pg ml−1 mU−1 l−1 in CL assay. However, the correlation was weaker in the low end of aldosterone concentrations (r=0.676 for aldosterone <100 pg ml−1), with a concordance of ivSLT results in only 68% of patients. CL assay displays a diagnostic performance very similar to RIA for ARR screening, but it is substantially inferior in the setting of confirmatory tests of autonomous aldosterone secretion, that is, ivSLT.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


References
Gordon RD, Stowasser M, Tunny TJ, Klemm SA, Rutherford JC . High incidence of primary aldosteronism in 199 patients referred with hypertension. Clin Exp Pharmacol Physiol 1994; 21 (4): 315–318.
Mulatero P, Stowasser M, Loh KC, Fardella CE, Gordon RD, Mosso L et al. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab 2004; 89 (3): 1045–1050.
Rossi GP, Bernini G, Caliumi C, Desideri G, Fabris B, Ferri C et al. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol 2006; 48 (11): 2293–2300.
Funder JW, Carey RM, Mantero F, Murad MH, Reincke M, Shibata H et al. The management of primary aldosteronism: case detection, diagnosis, and treatment: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2016; 101 (5): 1889–1916.
Rossi GP, Di Bello V, Ganzaroli C, Sacchetto A, Cesari M, Bertini A et al. Excess aldosterone is associated with alterations of myocardial texture in primary aldosteronism. Hypertension 2002; 40 (1): 23–27.
Milliez P, Girerd X, Plouin PF, Blacher J, Safar ME, Mourad JJ . Evidence for an increased rate of cardiovascular events in patients with primary aldosteronism. J Am Coll Cardiol 2005; 45 (8): 1243–1248.
Mulatero P, Monticone S, Bertello C, Viola A, Tizzani D, Iannaccone A et al. Long-term cardio- and cerebrovascular events in patients with primary aldosteronism. J Clin Endocrinol Metab 2013; 98 (12): 4826–4833.
Savard S, Amar L, Plouin PF, Steichen O . Cardiovascular complications associated with primary aldosteronism: a controlled cross-sectional study. Hypertension 2013; 62 (2): 331–336.
Catena C, Colussi G, Nadalini E, Chiuch A, Baroselli S, Lapenna R et al. Cardiovascular outcomes in patients with primary aldosteronism after treatment. Arch Intern Med 2008; 168 (1): 80–85.
Funder JW . Primary aldosteronism: are we missing the wood for the trees? Horm Metab Res 2012; 44 (3): 251–253.
Tiu SC, Choi CH, Shek CC, Ng YW, Chan FK, Ng CM et al. The use of aldosterone-renin ratio as a diagnostic test for primary hyperaldosteronism and its test characteristics under different conditions of blood sampling. J Clin Endocrinol Metab 2005; 90 (1): 72–78.
Stowasser M, Ahmed AH, Pimenta E, Taylor PJ, Gordon RD . Factors affecting the aldosterone/renin ratio. Horm Metab Res 2012; 44 (3): 170–176.
Stowasser M, Gordon RD . Aldosterone assays: an urgent need for improvement. Clin Chem 2006; 52 (9): 1640–1642.
Taylor PJ, Cooper DP, Gordon RD, Stowasser M . Measurement of aldosterone in human plasma by semiautomated HPLC-tandem mass spectrometry. Clin Chem 2009; 55 (6): 1155–1162.
Ray JA, Kushnir MM, Palmer J, Sadjadi S, Rockwood AL, Meikle AW . Enhancement of specificity of aldosterone measurement in human serum and plasma using 2D-LC-MS/MS and comparison with commercial immunoassays. J Chromatogr B Analyt Technol Biomed Life Sci 2014; 970: 102–107.
Rossi GP, Ceolotto G, Rossitto G, Seccia TM, Maiolino G, Berton C et al. Prospective validation of an automated chemiluminescence-based assay of renin and aldosterone for the work-up of arterial hypertension. Clin Chem Lab Med 2016; 54 (9): 1441–1450.
Burrello J, Monticone S, Buffolo F, Lucchiari M, Tetti M, Rabbia F et al. Diagnostic accuracy of aldosterone and renin measurement by chemiluminescent immunoassay and radioimmunoassay in primary aldosteronism. J Hypertens 2016; 34 (5): 920–927.
Pizzolo F, Zorzi F, Chiecchi L, Consoli L, Aprili I, Guarini P et al. NT-proBNP, a useful tool in hypertensive patients undergoing a diagnostic evaluation for primary aldosteronism. Endocrine 2014; 45 (3): 479–486.
Olivieri O, Ciacciarelli A, Signorelli D, Pizzolo F, Guarini P, Pavan C et al. Aldosterone to renin ratio in a primary care setting: the Bussolengo study. J Clin Endocrinol Metab 2004; 89 (9): 4221–4226.
Mulatero P, Milan A, Fallo F, Regolisti G, Pizzolo F, Fardella C et al. Comparison of confirmatory tests for the diagnosis of primary aldosteronism. J Clin Endocrinol Metab 2006; 91 (7): 2618–2623.
Linnet K . Necessary sample size for method comparison studies based on regression analysis. Clin Chem 1999; 45 (6 Pt 1): 882–894.
Pizzolo F, Corgnati A, Guarini P, Pavan C, Bassi A, Corrocher R et al. Plasma aldosterone assays: comparison between chemiluminescence-based and RIA methods. Clin Chem 2006; 52 (7): 1431–1432.
Schirpenbach C, Seiler L, Maser-Gluth C, Beuschlein F, Reincke M, Bidlingmaier M . Automated chemiluminescence-immunoassay for aldosterone during dynamic testing: comparison to radioimmunoassays with and without extraction steps. Clin Chem 2006; 52 (9): 1749–1755.
Mulatero P, Bertello C, Garrone C, Rossato D, Mengozzi G, Verhovez A et al. Captopril test can give misleading results in patients with suspect primary aldosteronism. Hypertension 2007; 50 (2): e26–e27.
Rossi GP, Belfiore A, Bernini G, Desideri G, Fabris B, Ferri C et al. Comparison of the captopril and the saline infusion test for excluding aldosterone-producing adenoma. Hypertension 2007; 50 (2): 424–431.
Nanba K, Tamanaha T, Nakao K, Kawashima ST, Usui T, Tagami T et al. Confirmatory testing in primary aldosteronism. J Clin Endocrinol Metab 2012; 97 (5): 1688–1694.
Manolopoulou J, Fischer E, Dietz A, Diederich S, Holmes D, Junnila R et al. Clinical validation for the aldosterone-to-renin ratio and aldosterone suppression testing using simultaneous fully automated chemiluminescence immunoassays. J Hypertens 2015; 33 (12): 2500–2511.
Acknowledgements
The work was performed in part in the LURM (Laboratorio Universitario di Ricerca Medica) Research Center, University of Verona. This study was supported by research grants from the Ministero dell’Istruzione dell’Università e della Ricerca (MIUR) and Fondazione Cariverona.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Pizzolo, F., Salvagno, G., Caruso, B. et al. Fully automated chemiluminescence vs RIA aldosterone assay in primary aldosteronism work-up. J Hum Hypertens 31, 826–830 (2017). https://doi.org/10.1038/jhh.2017.62
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhh.2017.62
This article is cited by
-
Urinary extracellular vesicle mRNA analysis of sodium chloride cotransporter in hypertensive patients under different conditions
Journal of Human Hypertension (2022)
-
An isotope dilution liquid chromatography-tandem mass spectrometry candidate reference measurement procedure for aldosterone measurement in human plasma
Analytical and Bioanalytical Chemistry (2021)
-
High efficiency of the aldosterone-to-renin ratio in precisely detecting primary aldosteronism
Journal of Human Hypertension (2019)
