
Abstract
Aim: Establish the minimal biochemical and radiological examinations necessary and their cost-effectiveness to accurately diagnose the etiology of Cushing's syndrome (CS).
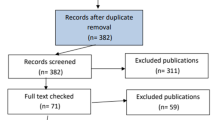
Material and Methods: In 71 patients with CS followed between 1982 and 1997 biochemical studies (basal ACTH, 8mg dexamethasone suppression test -HDST-, metyrapone stimulation test -MST-, or inferior petrosal sinus catheterization sinus catheterization -IPSC-) and radiological investigations (abdominal CT scan, pituitary CT scan or MRI) were performed. Once pathology confirmed the diagnosis (48 pituitary Cushing's disease-CD, 17 adrenal neoplasms, 2 bilateral macronodular hyperplasia -BMH-, and 4 ectopic ACTH syndrome -ES-), the sensitivity, specificity, positive and negative predictive value of the different studies was calculated to establish the most accurate and cost-effective diagnostic protocol.
Results: In ACTH-independent CS (ACTH ≤ 9 pg/ml; normal 9 to 54) a unilateral tumor was identified on abdominal CT scanning in 17, and BMH in 1; the other BMH had detectable ACTH (43.2 pg/ml). In ACTH-dependent CS, ACTH was > 9 pg/ml and IPSC (performed in 22) correctly identified 20 patients with CD and differentiated them from 2 with an ES (100 % specificity and sensitivity). Pituitary MRI or CT did not disclose an adenoma in 41.7% of patients with CD, and was reported to exhibit a microadenoma in 2 of the 4 patients with ES. HDST and MST were of no additional use in the differentiation between CD and ES.
Conclusions: Once CS is diagnosed low ACTH and an abdominal CT scan correctly identified all patients of adrenal origin. In ACTH-dependent CS IPSC was the best predictive test to differentiate CD from ES. BMH may behave as ACTH-dependent or independent. The other biochemical and radiological studies performed are not cost-effective and may even be misleading, and should not be routinely performed.
Similar content being viewed by others

References
Cushing H. The basophil adenomas of the pituitary body and their clinical manifestations. Bull Johns Hopkins Hosp 1932;1:137-195.
Orth DN. Cushing's syndrome. N Engl J Med 1995;332: 791-803.
Miller JW, Crapo L. The biochemical diagnoses of hypercortisolism. Endocrinologist 1994;4:7-16.
Aron DC, Finding JW, Tyrrell JB. Cushing's disease. Endocrinol Metab Clin North Am 1987;16:705-730.
Burke CW, Beardwell CG. Cushing's syndrome. An evaluation the clinical usefulness of urinary free cortisol and other steroid measurements in diagnosis. Q J Med 1973;42: 175-204.
Eddy R, Jones A, Lloyd G, Gilliland PF. Cushing's syndrome: a prospective study of diagnostic methods. Am J Med 1973;55:621-629.
Crapo L. Cushing's syndrome: a review of diagnostic tests. Metabolism 1979;28:955-977.
Liddle GW, Estep HL, Kendall JW, Williams WC, Townes AW. Clinical application of a new test of pituitary reserve. J Clin Endocrinol Metab 1959;19:875-894.
Kaye TB, Crapo L. The Cushing's syndrome: an update on diagnosis tests. Ann Intern Med 1990;112:434-444.
Sriussadaporn S, Ploybutr S, Peerapatdit T et al. Nocturnal 8mg DXM test: A practical and accurate test for identification of the cause of endogenous Cushing's syndrome. Br J Clin Pract 1996;50:9-13.
Carpenter PC. Diagnostic evaluation of Cushing syndrome. Endocrinol Metab Clin North Am 1988;17:445-472.
Flack MR, Oldfield EH, Cutler GB et al. Urine free cortisol in the high doses dexamethasone suppression test for the differential diagnosis of the Cushing syndrome. Ann Intern Med 1992;116:211-217.
Sindler BH, Griffing GT, Melby JC. The superiority of the metyrapone test versus the high-dose dexamethasone test in the differential diagnosis of Cushing's syndrome. Am J Med 1983;74:657-662.
Avgerinos PC, Yanovski JA, Oldfield EH, Nieman LK, Cutler GB. The metyrapone and dexamethasone suppression tests for the differential diagnosis of Cushing's syndrome: a comparison. Ann Intern Med 1994;121: 318-327.
Webb SM, Ruscalleda J, Schwarzstein et al. Computerized tomography versus magnetic resonance imaging: a comparative study in hypothalamic-pituitary and parasellar pathology. Clin Endocrinol 1992;36:459-465.
Miller DL, Doppman JL. Petrosal sinus sampling: Technique and rationale. Radiology 1991;178:37-47.
Oldfield EH, Doppman JL, Nieman LK et al. Petrosal sinus sampling with and without corticotropin-releasing hormone for the differential diagnosis of Cushing syndrome. N Eng J Med 1991;325:987-905.
Dickstein G, DeBold CR, Gaitan D et al. Plasma corticotropin and cortisol responses to ovine corticotropin releasing hormone (CRH), arginine vasopressin (AVP), CRH plus AVP, and CRH plus metyrapone in patients with Cushing's disease. J Clin Endocrinol Metab 1996;81:2934-2941.
Tsigos C, Papanicolaou DA, Chrousos CP. Advances in the diagnosis and treatment of Cushing's syndrome. Bailliere's Clin Endocrinol Metab 1995;9:315-336.
Weitzman DE, Fukishima DK, Nogeire C, Roffwarg H, Gallagher TF, Hellman L. Twenty-four hour pattern of the episodic secretion of cortisol in normal subjects. J Clin Endocrinol Metab 1971;33:14-22.
Veldhuis JD, Iranmanesh A, Johnson ML, Lizarralde G. Amplitude, but not frequency, modulation of adrenocorticotropin secretory bursts gives rise to the nyctohemeral rhythm of the corticotropic axis in man. J Clin Endocrinol Metab 1990;71:452-463.
Freda PU, Wardlaw SL, Bruce JN, Post KD, Goland RS. Differential diagnosis in Cushing's syndrome. Use of corticotropin-releasing hormone. Medicine 1995;74:74-82.
Shilo S, Rösler A. Single intravenous bolus of dexamethasone for the differential diagnosis of Cushing's syndrome. J Ped Endocrinol Metab 1995;8:27-33.
Shapiro MS, Shenkam L. Variable hormonogenesis in Cushing's syndrome. Quart J Med 1991;288:351-363.
Dunnick NR, Schaner EG, Doppman JL, Strott CA, Gill JR, Javadpour N. Computer tomography in adrenal tumors. Am J Roentgenol 1987;132:43-46.
Doppman JL, Nieman LK, Travis WD. CT and MRI of massive macronodular adrenocortical disease: a rare cause of autonomous primary adrenal hypercortisolism. J Comput Assist Tomogr 1991;15:773-779.
Findling JW, Aron DC, Tyrrell JB et al. Selective venous sampling for ACTH in Cushing's syndrome: differentiation between Cushing's disease and the ectopic ACTH syndrome. Ann Intern Med 1981;94:647-652.
Besser GM, Edwards CRW. Cushing's syndrome. Clin Endocrinol Metab 1972;1:451-490
Leinung MC, Young WF, Whitaker MD, Scheithauer BW, Trastek VF, Kvols LK. Diagnosis of corticotropin-producing bronchial carcinoid tumours causing Cushing's syndrome. Mayo Clin Proc 1990;65:1314-1321.
Flint LD, Jacobs EC. Belated recognition of adrenocorticotropic hormone-producing tumors post-adrenalectomized Cushing's syndrome. J Urol 1974;112:688-694.
Aron DC, Raff H, Findling JW. Effectiveness Versus Efficacy: The limited value in clinical practice of high dose dexamethasone suppression testing in the differential diagnosis of adrenocorticotropin dependent Cushing's syndrome. J Clin Endocrinol Metab 1997;82:1780-1785.
Tsigos C, Chrousos GP. Differential diagnosis and management of Cushing's Syndrome. Annu Rev Med 1996;47: 443-461.
Tyrrell JB, Findling JW, Aron DC, Fitzgerald PA, Forsham PH. An overnight high-dose dexamethasone suppression test for rapid differential diagnosis of Cushing's syndrome. Ann Intern Med 1986;104:180-186.
Urbanic RC, George JM. Cushing's disease: 18 years experience. Medicine 1981;60:14-24.
Nieman LK, Chrousos GP, Oldfield EH, Avgerinos PC, Cutler GB, Loriaux DL. The ovine corticotropin-releasing hormone stimulation and the dexamethasone suppression test in the differential diagnosis of Cushing's syndrome. Ann Intern Med 1986;105:862-867.
Carpenter PC. Cushing's syndrome: an update of diagnosis and management. Mayo Clin Proc 1986;61:49-58.
Strott CA, Nugent CA, Tyler FH. Cushing's syndrome caused by bronchial adenomas. Am J Med 1968;44:97-104.
Mason AMS, Ratcliffe JG, Buckle RM, Mason AS. ACTH secretion by bronchial carcinoid tumours. Clin Endocrinol 1972;1:3-25.
De Herder WW, Uitterlinden P, Pieterman H et al. Pituitary tumour localisation in patients with Cushing's disease by magnetic resonance imaging. Is there a place for petrosal sinus sampling? Clin Endocrinol 1994;40:87-92.
Parent AD, Bebin J, Smith RR. Incidental pituitary adenomas. J Neurosurg 1981;54:228-231.
Burrow GN, Wortzman G, Rewcastle NB, Holgate RC, Kovacs K. Microadenomas of the pituitary and abnormal sellar tomograms in an unselected autopsy series. N Eng J Med 1981;304:156-158.
Hall WA, Luciano MG, Doppman JL, Patronas NJ, Oldfield EH. Pituitary magnetic resonance imaging in normal human volunteers: occult adenomas in the general population. Ann Intern Med 1994;120:817-820.
Contreras P, Araya V. Sindrome de Cushing: Una revisión a propósito de una casuística nacional. Rev Med Chile 1995;123:350-362.
Miller DL, Doppman JL, Peterman SB, Nieman LK, Oldfield EH, Chang R. Neurologic complications of petrosal sinus sampling. Radiology 1992;185:143-147.
Sasaki A, Shinkawa O, Margioris AN. Immunoreactive corticotropin-releasing hormone in human plasma during pregnancy, labor and delivery. J Clin Endocrinol Metab 1987;64:224-229.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Puig, J., Wägner, A., Caballero, A. et al. Cost-effectiveness and accuracy of the tests used in the differential diagnosis of Cushing's syndrome.. Pituitary 1, 125–132 (1999). https://doi.org/10.1023/A:1009936622150
Issue Date:
DOI: https://doi.org/10.1023/A:1009936622150