
Abstract
Background
Patients with advanced heart failure (AHF) are extensively evaluated before heart transplantation or left ventricular assist device (LVAD) eligibility. Patients are assessed for medical need and psychosocial or economic factors that may affect success post-treatment. For patients to be evaluated, however, they first must be referred. This study investigated social and economic factors affecting AHF referral, specialist visits, or treatment.
Methods
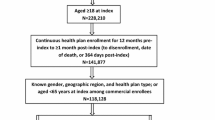
Patients with heart failure (n = 24,258) were reviewed at one large hospital system over 4 years. Independent variables age, sex, marital status, race/ethnicity, preferred language, smoking, and insurance status were assessed for the outcomes of referral, clinic visit, and treatment by Chi-square and ANOVA. In-house and 1-year mortality were evaluated by logistic regression, and time-to-event was assessed by the Cox proportional hazards model.
Results
Younger (HR 0.934, 95% CI 0.925–0.943), male (HR 2.216, 95% CI 1.544–3.181), and publicly insured (HR 1.298 [95% CI 1.038, 1.623]) patients were more likely to be referred, while unmarried (HR 0.665, 95% CI 0.488–0.905) and smoking (HR 0.549, 95% CI 0.389–0.776) patients had fewer referrals. Younger, married, and nonsmoking patients were more likely to have a clinic visit. Younger age, White race, and Hispanic/Latino ethnicity were associated with receiving a heart transplant, and LVAD recipients were more likely Hispanic/Latino ethnicity. Advanced age, Hispanic/Latino ethnicity, and smoking were associated with 1-year mortality after heart failure diagnosis.
Conclusions
Disparities in access exist before evaluation for AHF therapies. Improving access at the levels of referral and evaluation is a necessary step toward achieving equity in organ allocation.

Similar content being viewed by others


Data Availability
The data that support the findings of this study are not publicly available. Data may be requested for research purposes to investigators with approved data use agreements with Corewell Health.
References
Bozkurt B, et al. Universal definition and classification of heart failure. J Cardiac Fail. 2021;27(4):387–413.
Mayo Clinic. Ventricular Assist Device (VAD). 2022 August 29, 2022]; Available from: https://www.mayoclinic.org/tests-procedures/ventricular-assist-device/about/pac-20384529.
Hsich EM. Sex differences in advanced heart failure therapies. Circulation. 2019;139(8):1080–93.
Chouairi F, et al. Evaluation of racial and ethnic disparities in cardiac transplantation. J Am Heart Assoc. 2021;10(17):e021067.
National Organ Transplant Act, in Public Law. 1984.
Cogburn CD. Culture, race, and health: implications for racial inequities and population health. Milbank Q. 2019;97(3):736–61.
Spectrum health heart, lung and vascular locations. June 13, 2019]; Available from: https://www.spectrumhealth.org/patient-care/cardiovascular/heart-and-vascular-locations.
Epic Systems Corporation, Epic hyperspace. Verona, Wisconsin. 2021: Verona, Wisconsin.
Office for Human Research Protections. Attachment D: FAQ’s terms and recommendations on informed consent. 2011 August 29, 2022]; Available from: https://www.hhs.gov/ohrp/sachrp-committee/recommendations/2011-october-13-letter-attachment-d/index.html.
IBM SPSS Statistics for Windows. IBM Corp.: Armonk, NY.
Thabane L, et al. A tutorial on sensitivity analyses in clinical trials: the what, why, when and how. BMC Med Res Methodol. 2013;13:92.
Tsao CW, et al. Heart disease and stroke statistics—2023 update: a report from the American Heart Association. Circulation. 2023;147(8):e93–621.
Abouezzeddine OF, Redfield MM. Who has advanced heart failure?: definition and epidemiology. Congest Heart Fail. 2011;17(4):160–8.
Mehra MR, et al. Listing criteria for heart transplantation: International Society for Heart and Lung Transplantation guidelines for the care of cardiac transplant candidates–2006. J Heart Lung Transplant. 2006;25(9):1024–42.
Stehlik J, et al. The Registry of the International Society for Heart and Lung Transplantation: 29th official adult heart transplant report–2012. J Heart Lung Transplant. 2012;31(10):1052–64.
Guglin M, et al. Evaluation for heart transplantation and LVAD implantation: JACC Council Perspectives. J Am Coll Cardiol. 2020;75(12):1471–87.
Thorvaldsen T, Lund LH. Focusing on referral rather than selection for advanced heart failure therapies. Card Fail Rev. 2019;5(1):24–6.
Bairey Merz CN, et al. Insights from the NHLBI-Sponsored Women’s Ischemia Syndrome Evaluation (WISE) Study: Part II: gender differences in presentation, diagnosis, and outcome with regard to gender-based pathophysiology of atherosclerosis and macrovascular and microvascular coronary disease. J Am Coll Cardiol. 2006;47(3 Suppl):S21–9.
Habal MV, Axsom K, Farr M. Advanced therapies for advanced heart failure in women. Heart Fail Clin. 2019;15(1):97–107.
Morris AA, et al. Guidance for timely and appropriate referral of patients with advanced heart failure: a scientific statement from the American Heart Association. Circulation. 2021;144(15):e238–50.
Schulman K, et al. The effect of race and sex on physicians’ recommendations for cardiac catheterization. N Engl J Med. 1999;340:618–26.
Einbinder LC, Schulman KA. The effect of race on the referral process for invasive cardiac procedures. Med Care Res Rev. 2000;57:162–80.
Todd KH, et al. Ethnicity and analgesic practice. Ann Emerg Med. 2000;35(1):11–6.
Waldman SV, et al. Ethnic differences in the treatment of depression in patients with ischemic heart disease. Am Heart J. 2009;157(1):77–83.
Bliss EB, et al. Variation in participation in health care settings associated with race and ethnicity. J Gen Intern Med. 2004;19(9):931–6.
Clark-Hitt R, et al. Doctors’ and nurses’ explanations for racial disparities in medical treatment. J Health Care Poor Underserved. 2010;21(1):386–400.
Benjamin EJ, et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–528.
Nayak A, Hicks AJ, Morris AA. Understanding the complexity of heart failure risk and treatment in Black patients. Circ Heart Fail. 2020;13(8):e007264.
Colvin M, et al. Heart failure in non-Caucasians, women, and older adults: a white paper on special populations from the Heart Failure Society of America Guideline Committee. J Card Fail. 2015;21(8):674–93.
Hadley J. Insurance coverage, medical care use, and short-term health changes following an unintentional injury or the onset of a chronic condition. JAMA. 2007;297(10):1073–84.
Pandey KR, et al. The impact of marital status on health care utilization among Medicare beneficiaries. Medicine (Baltimore). 2019;98(12):e14871.
Clemons AM, et al. Effect of socioeconomic status on patients supported with contemporary left ventricular assist devices. ASAIO J. 2020;66(4):373–80.
Espinosa J, Evans WN. Heightened mortality after the death of a spouse: marriage protection or marriage selection? J Health Econ. 2008;27(5):1326–42.
Robards J, et al. Marital status, health and mortality. Maturitas. 2012;73(4):295–9.
Dunlay SM, et al. Patient and spousal health and outcomes in heart failure. Circ Heart Fail. 2017;10:10.
Kahende JW, et al. Disparities in health care utilization by smoking status–NHANES 1999–2004. Int J Environ Res Public Health. 2009;6(3):1095–106.
Patzer RE, et al. Dialysis facility referral and start of evaluation for kidney transplantation among patients treated with dialysis in the Southeastern United States. Am J Transplant. 2020;20(8):2113–25.
Goff DC Jr, et al. Knowledge of heart attack symptoms in a population survey in the United States: the REACT trial. Rapid early action for coronary treatment. Arch Intern Med. 1998;158(21):2329–38.
Breathett K, et al. Factors related to physician clinical decision-making for African-American and Hispanic patients: a qualitative meta-synthesis. J Racial Ethn Health Disparities. 2018;5(6):1215–29.
Cascino TM, et al. Racial inequities in access to ventricular assist device and transplant persist after consideration for preferences for care: a report from the REVIVAL study. Circ Heart Fail. 2023;16(1):e009745.
Thibodeau JT, et al. Health insurance as a requirement to undergo cardiac transplantation: a national survey of transplant program practices. Transplant Proc. 2013;45(1):360–3.
Hutcheson SS, et al. Impact of insurance type on eligibility for advanced heart failure therapies and survival. Clin Transplant. 2018;32(8):e13328.
King LP, et al. Health insurance and cardiac transplantation: a call for reform. J Am Coll Cardiol. 2005;45(9):1388–91.
Baumwol J. “I Need Help”-a mnemonic to aid timely referral in advanced heart failure. J Heart Lung Transplant. 2017;36(5):593–4.
Raphael C, et al. Limitations of the New York Heart Association functional classification system and self-reported walking distances in chronic heart failure. Heart. 2007;93(4):476–82.
Thorvaldsen T, et al. Triage of patients with moderate to severe heart failure: who should be referred to a heart failure center? J Am Coll Cardiol. 2014;63(7):661–71.
Hauptman PJ, et al. Physician attitudes toward end-stage heart failure: a national survey. Am J Med. 2008;121(2):127–35.
Vivo RP, et al. Heart failure in Hispanics. J Am Coll Cardiol. 2009;53(14):1167–75.
Institute of Medicine (US), Committee on understanding and eliminating racial and ethnic disparities in health care; Smedley BD, Stith AY, Nelson AR, editors. Unequal treatment: confronting racial and ethnic disparities in health care. Washington (DC): National Academies Press (US); 2003. Available from: https://www.ncbi.nlm.nih.gov/books/NBK220358/https://doi.org/10.17226/12875
Blair IV, Steiner JF, Havranek EP. Unconscious (implicit) bias and health disparities: where do we go from here? Permanente J. 2011;15(2):71–8.
Chapman EN, Kaatz A, Carnes M. Physicians and implicit bias: how doctors may unwittingly perpetuate health care disparities. J Gen Intern Med. 2013;28(11):1504–10.
Mayberry RM, et al. Improving quality and reducing inequities: a challenge in achieving best care. Proc (Bayl Univ Med Cent). 2006;19(2):103–18.
Breathett K, et al. Does race influence decision making for advanced heart failure therapies? J Am Heart Assoc. 2019;8(22):e013592.
Wadhwani SI, Lai JC, Gottlieb LM. Medical need, financial resources, and transplant accessibility. JAMA. 2022;327(15):1445–6.
Acknowledgements
We thank Western Michigan University for the Graduate College Research Opportunity. Thank you to Indiana University and the NIH for the T32 Postdoctoral Fellowship (5T32DK120524-05) support. The contents of this paper are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. Many thanks to Ruth Kurtycz, PhD, for their statistical expertise and consultation.
Funding
The research was funded in part by a competitive research award toward dissertation research completion (Graduate College Research Opportunity) from Western Michigan University (Catherine Kelty). This publication was also made possible by an NIH-funded postdoctoral fellowship for Catherine Kelty (T32 5T32DK120524-05) within the Indiana University Kidney Training Program.
Author information
Authors and Affiliations
Contributions
All authors contributed to study conception and design. Data collection and analysis were performed by Catherine Kelty. All authors contributed to the interpretation of results. The first draft was written by Catherine Kelty, and all authors critically reviewed previous manuscript versions. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval
This research was approved separately by the Corewell Health Institutional Review Board and Western Michigan University Institutional Review Board. Both boards issued non-human subjects research determinations for this study.
Informed Consent
N/A for non-human subjects research.
Consent for Publication
N/A for non-human subjects research.
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Kelty, C.E., Dickinson, M.G., Lyerla, R. et al. Non-Medical Characteristics Affect Referral for Advanced Heart Failure Services: a Retrospective Review. J. Racial and Ethnic Health Disparities (2023). https://doi.org/10.1007/s40615-023-01879-w
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40615-023-01879-w