
Abstract
Purpose of Review
Long COVID, or post-COVID Condition, is increasingly recognized in children and adolescents, despite being less studied compared with the adult population. Recent studies are documenting that inappropriate sinus tachycardia (IST) or postural orthostatic tachycardia syndrome (POTS) may be key clinical problems in patients with long COVID, and preliminary findings have shown that these may be important features also in children. However, POTS and IST are poorly known among non-specialized pediatricians, and this gap may limit access to appropriate care for children and adolescents with long COVID or other post-viral fatigue syndromes. In this review, we critically evaluate the available literature investigating the burden of post-COVID-19 IST and POTS in children and young people, their pathogenesis, and available evidence for their management in the pediatric population.
Recent Findings
In line with adult studies, there is increasing evidence that also children with long COVID may suffer from IST and POTS. Case reports and case series, as well as pediatric experience from other conditions, suggest that IST and POTS can be treated also in the pediatric population
Summary
IST and POTS are under-recognized conditions in children. Clinical findings as well as diagnostics like 24-h ECG and heart rate variability are non-invasive tests to diagnose IST and POTS. If properly recognized, these conditions are treatable.
Similar content being viewed by others

Introduction
Long COVID, or post-COVID condition, refers to the long-term persistence of symptoms in children with a history of confirmed or probable SARS-CoV-2 infection. Fatigue, headaches, tachycardia, palpitations, post-exertional malaise, and brain fog are among the most commonly reported problems by patients, parents, and family associations. Presentations overlap with other post-viral syndromes such as myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). In both these clinical syndromes, there is growing evidence that some of these symptoms can be due to inappropriate sinus tachycardia (IST) or postural orthostatic tachycardia syndrome (POTS). However, these conditions are poorly characterized in the pediatric populations and, as a consequence, poorly understood by pediatricians, with subsequent reduction in clinical recognition of these issues and negative impact on access to appropriate care experienced by patients and families.
In this review, we critically evaluate the available literature investigating the burden of post-COVID-19 IST and POTS in children and young people, their pathogenesis, and available evidence for their management in the pediatric population.
POTS and IST Introduction: Epidemiology and Definition
Inappropriate sinus tachycardia (IST) and postural orthostatic tachycardia syndrome (POTS) are syndromes with overlapping clinical features of excessive sinus tachycardia. While the elevated heart rate (HR) in POTS is predominantly triggered by orthostatic stress, IST is defined as a fast sinus rhythm (> 100 bpm) at rest or during minimal activity that is out of proportion with the level of physical, emotional, pathological, or pharmacological stress [1].
IST is usually persistent and mainly affects young women, with an incidence ratio of 4:1 compared to men and an average age between 15 and 45 years [2]. Its prevalence is unclear because several confounding variables, including different definitions, appear to influence its estimates. A 24-h Holter ECG with an average HR > 90 bpm and an exaggerated HR response > 100 bpm during daylight hours is diagnostic. The HR pattern (rapid, but not abrupt, warming up and slow cooling down) is useful, as it can be diagnostic of sinus tachycardia and allows exclusion of supraventricular tachycardias, which are most often characterized by an abrupt onset and end (“on-off” pattern) [3]. Symptoms are variable and range from asymptomatic or mildly symptomatic forms to patients presenting with dyspnoea, dizziness, and light-headedness.
POTS is defined as a clinical syndrome usually characterized in adults by an increase in HR of > 30 bpm when standing for > 30 s, in the absence of orthostatic hypotension (> 20 mmHg drop in systolic blood pressure during the position change) [4]. The prevalence of POTS is 0.2%, and it represents the most common cause of orthostatic intolerance in the young, with most patients aged between 15 and 25 years, more than 75% being female. POTS is diagnosed during a 10-min active or passive stand test or head-up tilt test with non-invasive hemodynamic monitoring [5,6,7]. Although the exact relationship between IST and POTS is unknown, the overlapping multisystemic and autonomic abnormalities seen in selected IST patients suggest that these two syndromes may share some common pathophysiologic mechanisms [8]. The mechanism is still not clear, but it is likely to be multifactorial. Also, viral infections like COVID-19 may lead to an autonomic imbalance that could manifest with POTS or IST [9]. Specifically, Sandroni et al. have reported that up to 50% of patients with POTS reported a history of infection closely preceding the onset of their POTS symptoms [10].
IST and POTS as Sequelae of COVID-19 Infection
Coronavirus disease 19 (COVID-19) is a viral illness caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Declared a global pandemic in March 2020, it has infected over 500 million individuals and caused more than 6 million deaths [11]. While severe respiratory manifestations and multi-organ failure may occur in as many as 15% and 5% of cases, 80% present as paucisymptomatic and self-limiting [12]. Increasing evidence suggests that long-term multi-organ manifestations, together with its associated symptoms, may persist after the acute phase of the infection [13,14,15] in the form of “long COVID” [16, 17]. Despite no universally accepted definition, long COVID is generally defined as the persistence of symptoms after 8–12 weeks from the SARS-CoV-2 infection [18]. It may be divided into two phases based on symptom duration: an ongoing symptomatic phase if symptoms last between 4 and 12 weeks and a post-COVID-19 syndrome if symptoms persist more than 12 weeks. The World Health Organization (WHO) has recently defined post-COVID-19 as the persistence of symptoms at 3 months from the initial infection and that last for > 2 months, in the absence of other possible causes [19]. In literature, post-acute COVID-19 syndrome, post-acute sequelae of COVID-19 (PASC), and long-haul COVID have also been used interchangeably to describe long COVID-19 [20,21,22].
Its prevalence is unclear, as numerous confounding variables, including varying definitions, seem to influence estimates. In adults, a UK survey from November 2020 suggests that approximately 20% of patients reported persistence of symptoms after 5 weeks from the acute infections and 10% reported symptoms after 12 weeks [22]. On the contrary, research clearly links the risk of long COVID with several risk factors, including female sex, increasing age, and obesity [23].
Its heterogeneous clinical manifestations are multisystemic and include fatigue; pain and headaches; cardiopulmonary symptoms such as chest pain, dyspnea, arrhythmias, hypertension, postural hypotension, and exercise intolerance; gastrointestinal symptoms; neuropsychiatric symptoms (olfactory and gustatory dysfunction, anxiety and depression, cognitive impairment or brain fog, memory deficits, difficulty concentrating, sleep disturbances, Guillain-Barré syndrome, seizures); and skin rashes [24].
Among its clinical manifestations, dysautonomia appears to be an under-recognized and multi-faceted pathophysiologic event with potential implications on various organ systems, including the cardiovascular system. Recent evidence has unveiled a link between COVID-19 and the appearance of dysautonomic conditions, such as POTS and IST, which may be characterizing signs and symptoms of long COVID [25].
There are several non-mutually exclusive pathophysiological mechanisms that might be associated with post-COVID POTS. One is hypovolemia: fever, nausea, anorexia, weight loss, and nocturnal sweating might operate together to decrease blood volume. Moreover, prolonged bed rest and deconditioning can be part of a vicious cycle involving low stroke volume, high sympathetic adrenergic and noradrenergic system outflows, exercise intolerance, and fatigue. Second, SARS-CoV-2 may infect and destroy extracardiac postganglionic neurons of the sympathetic noradrenergic system (SNS), thus increasing cardiac SNS outflow in a manner analogous to neuropathic POTS. This may cause splanchnic venous pooling or a failure of reflexive mesenteric vasoconstriction during orthostasis. Although myocardiocytes express the ACE2 receptor that allows viral access to the cell, autopsy studies do not suggest direct myocardial lesions in COVID-19. Third, the virus could invade the brainstem and alter the functions of medullary centers, resulting in increased central sympathetic outflows and psychiatric comorbidities, such as anxiety and depression. Fourth, autoimmunity after the infection, in the form of autoimmune markers and autoantibodies, has been widely described in the literature [26, 27] (Fig. 1).

Potential pathophysiological mechanisms that might be associated with long COVID POTS and IST (created with Biorender.com)
Dysautonomia, together with other pathophysiological mechanisms, appears to be a shared trait in both IST and POTS. COVID-19 may damage the cardiovascular system by other mechanisms, such as hyper-inflammation, hypercoagulability, and dysfunction of the renin-angiotensin-aldosterone system, and may also provoke pulmonary injury or exacerbate underlying lung disease to cause desaturation and reflex tachycardia. Decreased parasympathetic activity due to M2 receptor autoantibody or hyposensitivity may lead to decreased vagal inhibitory activity on the sinus node. A 2022 study by Aranyó et al. [28] investigated the pathophysiological mechanisms of IST in patients after COVID-19 infection. The study revealed a decrease in HR variability parameters, mostly related to cardiovascular tone in patients with IST, in the absence of underlying structural heart disease, myocyte injury, hypoxia, or an inflammatory state. For this reason, it has been hypothesized that cardiac autonomic imbalance with a decrease in parasympathetic activity in favor of increased compensatory sympathetic tone is the causative mechanism of the IST in patients after COVID-19. The hypoactivity of the parasympathetic tone could explain not only the tachycardia, but also all the prevalent symptoms that often are present in the post-COVID-19 syndrome such as fatigue, gastrointestinal discomfort, headache, sore throat, neuro-cognitive disorder, and altered sleep structure.
Management in General Population and Post-COVID-19 Syndrome
The management of these arrhythmias (POTS and IST) involves a pharmacological and non-pharmacological approach [29, 30]. The management of post-COVID-19 tachycardia syndromes is similar to that of non-COVID-19-related POTS and IST.
Physicians should collect the patient’s past medical history, asking about symptoms that suggest possible signs of autonomic dysfunction, such as gastrointestinal or urinary dysfunction, abnormal sweating, acrocyanosis, dry mouth, and unexplained fever [31]. The clinical history should focus on the problematic symptoms such as fatigue, dizziness, and syncope, defining the chronicity of the condition, possible causes/triggers of orthostatic tachycardia such as weight loss or underweight, dehydration, modifying factors, impact on daily activities, potential triggers, and family history. Particular attention should be focused on the patient’s diet and activity history [32]. Selected patients might benefit from a thyroid function test and hematocrit, 24-h Holter, transthoracic echocardiogram, and exercise stress testing.
Non-pharmacological management of IST involves lifestyle modification, firstly by avoiding triggers or stimulants such as caffeine, nicotine, and alcohol. Symptom-driven physical inactivity often leads to significant physical debilitation and consequent psychosocial effects such as withdrawal from activities and low mood or anxiety.
Non-pharmacological treatments for POTS include increasing blood volume with more salt and > 2 L/day fluid intake, reducing venous retention with compression clothing, and limiting deconditioning. In addition, patients should cautiously engage in a regular, gradual, and supervised exercise program (where tolerated) that includes aerobic reconditioning and resistance training for the thighs, initially started supine.
Pharmacological treatments should be considered if individuals present with debilitating or persistent symptoms despite the use of non-pharmacological management techniques, but medical treatment of IST or POTS is not universally effective [33].
Non-selective ß1 selective therapy is the most common initial therapy; however, these medications are poorly tolerated, even if their titration is not limited by hypotension or side effects [4, 34]. Non-selective beta-blockers are also preferable by blocking epinephrine-mediated beta-2 vasodilation. Low-dose oral propranolol acutely lowers the standing HR and improves symptoms [35]. Similarly, calcium channel blockers have had limited use [36]. If ß-blockers and calcium channel blockers are ineffective, ivabradine, a funny current I(f) inhibitor, has shown significant promise in the treatment of IST, with studies demonstrating its superiority in terms of both effectiveness and tolerability, when compared to beta-blockers and other available therapies [37, 38]. In a prospective observational study involving a total of 55 patients with COVID-19-associated POTS, started on ivabradine 5 mg twice daily, 43 of 55 (78%) patients reported significant improvement of the symptoms within 7 days of ivabradine therapy. The 24-h HR (minimum, average, and maximum) was significantly lower, with a significant difference in HR variability time-domain parameters after ivabradine therapy [39]. These results are in line with those of another study that compared ivabradine (5 mg twice daily) and carvedilol (3.125 mg twice daily) in 24 patients who developed sinus tachycardia after COVID-19 infection. Although both were effective in controlling HR in post-COVID-19 patients without any comorbidities, ivabradine is more effective in controlling HR than carvedilol. Furthermore, the ivabradine group scores very high in “patient satisfaction” with regard to symptom relief (palpitation). Possible mechanisms behind these findings are the possible action of ivabradine on the sinus node, which appears to be more effective than atrio-ventricular blockers [40].
With regard to POTS, midodrine administered three times a day may be considered to improve symptoms related to tachycardia [20].
Pyridostigmine, a cholinergic agonist that inhibits acetylcholinesterase, may also increase parasympathetic activity, with a low risk of hypertension. However, the drug can cause abdominal pain, diarrhea, and muscle cramps [41].
Current guidelines recommend the administration of ivabradine with a beta-blocker whenever possible; this combination may be more beneficial than each drug alone for IST and POTS. Radiofrequency sinus node (SN) modification is not recommended [4]. For these interventions, caution is needed in young women and adolescents of childbearing age, with pregnancy status to be assessed.
POTS and IST in Children and Young People
For children and adolescents, the diagnostic criteria of POTS include symptoms of orthostatic intolerance together with a normal supine HR and an HR increase of at least 40 bpm during position change or a maximum HR over 130 bpm for children aged 6–12 years and > 125 bpm for adolescents aged 13–18 years in the first 10 min of an active standing test or during the passive head-up tilt test, in the absence of orthostatic hypotension characterized by a reduction in systolic blood pressure (SBP) of more than 20 mmHg or a reduction in diastolic blood pressure (DBP) by more than 10 mmHg. POTS is an underdiagnosed and undertreated disease, so it is difficult to estimate its incidence. A Chinese study that enrolled 600 patients aged between 7 and 18 years revealed an incidence of 6.8%. Unlike the disease in adults, which has a female prevalence, no significant difference between the two sexes was found in this study [42]. To date, although the precise pathophysiology underlying pediatric POTS remains unclear, some literature data suggest a multifactorial pathogenesis even in the pediatric form.
The main causes investigated include hypovolemia in the context of volume dysregulation, hyperadrenergic states, autoimmunity, peripheral autonomic neuropathy, and excessive venous pooling [43]. From the study cited above, low fluid intake and consequent low blood volume were associated with a higher incidence of POTS. Indeed, children who consumed less than 800 mL/day had a 3.8 times higher incidence than those who consumed more. Autonomic nerve dysfunction also plays a central role in children. Studies have shown increased baroreflex sensitivity (BRS) and elevated plasma noradrenaline levels in orthostatism in children with POTS [44, 45]. In a trial that included 46 children aged 12 +/− 3 years with POTS and twenty healthy children aged 12 +/− 4 years, flow-mediated vasodilation (FMD) and plasma concentrations of nitric oxide (NO) and NO synthase (NOS) activity were investigated. The FMD of each participant’s brachial artery was measured by color Doppler vascular ultrasound. Patients in the POTS group had a higher FMD (10.8 +/− 4.4%) than children in the control group (5.7 +/− 2.2%, P < 0.01). Furthermore, plasma levels of NO and NOS were significantly higher in the POTS group. Hence, vasodilation and vascular endothelium dysfunction may play an important role in this population [46]. Autoimmunity would also seem to play a causal role [47]. POTS patients appear to have higher autoimmune marker levels (e.g., antinuclear antibody (25 vs. 16%) and antiphospholipid antibody), as well as an increased incidence of comorbid autoimmune diseases such as Hashimoto thyroiditis, rheumatoid arthritis, systemic lupus erythematosus, and common variable immunodeficiency [48]. Although the causative role of infections, including COVID-19, in the adult form suggests a similar role in pediatric POTS, data is scarce.
Petracek et al. describe a case of a 19-year-old male with confirmed COVID-19, who developed orthostatic symptoms within 2 weeks of diagnosis [49•]. An orthostatic standing testing revealed a striking 70 bpm increase in HR from supine to standing, consistent with a diagnosis of POTS. Another case report documented the onset of POTS in a 16-year-old boy 6 weeks after infection with COVID-19. In fact, after undergoing a 10-min passive standing test, there was an increase in HR of 64 bpm, from 49 bpm supine to a peak of 113 bpm standing, associated with a worsening of orthostatic symptoms, and in the absence of orthostatic hypotension [50•].
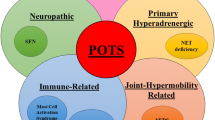
After diagnosis, health education remains the fundamental strategy, followed by non-pharmacological and pharmacological interventions. First of all, children and parents must be educated on the possible triggers, such as long periods of standing, sudden head-up postural changes, and high ambient temperatures, and on strategies to avoid them. Most of these factors, mediate their effect through vasodilation with consequent blood pooling and decreased effective circulatory volume. Infection, sympathetic activation, and lack of sleep may aggravate symptoms [51] (Fig. 2).

Potential pathogenetic mechanisms involved in POTS and IST in children and adolescents. POTS, postural orthostatic tachycardia syndrome; IST, inappropriate sinus tachycardia
Non-pharmacological management of POTS aims at increasing fluid intake by improving effective circulatory volume and venous return [52••]. Notably, the intake of at least 2–3 L of water per day and increased sodium intake is recommended [52••]. An indicator of the effectiveness of salt supplementation in children with POTS may be the 24-h urinary sodium excretion. Zhang et al. [53] compared 24-h urinary sodium levels before treatment between POTS children and healthy controls. The results showed that, compared to the control group, the 24-h urinary sodium level at baseline was low in the POTS group (117.09 ± 58.63 mmol/24 h versus 193.88 ± 91.12 mmol/24 h, P = 0.004). Furthermore, symptom severity was negatively correlated with 24-h urinary sodium excretion. Children with POTS are advised to appropriate initial supine physical exercises to improve the pumping function of the limb muscles and autonomic nervous system exercises to improve autonomic tone. Indeed, some investigators have found that a regular and progressive short-term exercise program leads to an improvement in symptoms in patients with POTS [54]. However, caution should be taken to start slowly in those with post-COVID condition/syndrome where post-exertional malaise (PEM) is present to ensure that any exercises do not cause exacerbation of the condition. In fact, when POTS is present in the context of PEM, several experts suggest that pushing patients to train beyond their tolerance threshold can cause severe malaise for the following days, and a recent rigorous study in adults, based on muscle biopsies and metabolic studies, demonstrated that muscle abnormalities worsen after post-exertional malaise in long COVID [55]. As a consequence, gradual exercise should always be balanced with pacing strategies teaching the patient to train arriving to the tolerated threshold of heart rate and fatigue.
If these interventions are ineffective, pharmacological therapies should be applied to solve specific issues. β-adrenoreceptor blockers, which are considered first-line drugs, can reduce the effect of catecholamines by acting on β1 receptors to reduce the increase in HR and alleviate symptoms. However, not all children responded to beta-blocker therapy. In the study by Zhang et al., 27 children with POTS received metoprolol treatment, and their orthostatic plasma norepinephrine levels were measured by the high-performance liquid chromatography method. Only patients who had an elevated norepinephrine level (> 3.59 pg/mL) responded to metoprolol therapy [41]. Another marker for predicting the effect of metoprolol in children and adolescents with POTS is the plasma copeptin assay. A trial showed that the plasma copeptin level, as measured by a sandwich immunoluminometric test, was higher in children with POTS than in controls and was lower for responders than for non-responders to metoprolol (9.377 ± 1.411 vs. 12.054 ± 1.662 pmol/L, P = 0.003). Baseline plasma copeptin level could be used as a biomarker to predict the therapeutic efficacy of metoprolol in children with POTS [56].
Metoprolol has been proposed as a possible drug to use, with an initial dose of 0.5 mg/kg/day in treating pediatric POTS (108) and a maximum dose of 2 mg/kg/day in severe cases, based on symptoms [57].
Oral midodrine hydrochloride, which is enzymatically hydrolyzed into the selective 1-adrenoceptor agonist desglymidodrine, theoretically helps treat POTS by constricting veins and arteries to increase venous return. Treatment with midodrine was compared with beta-blockers in a retrospective study of 121 adolescents with POTS who had undergone autonomic reflex screening at the Mayo Clinic from 2002 to 2005. In this study, beta-blockers were more effective in improving symptoms than those treated with midodrine. In contrast, another study compared midodrine hydrochloride (2.5 mg/day) plus conventional therapy (that included increased water and salt intake, avoidance of predisposing situations, maneuvers to prevent blood pooling in the limbs and lower extremities such as leg crossing) (group I) with metoprolol plus conventional therapy (group II) and with conventional therapy alone (group III). The symptom score and the symptom recurrence rate in group I were significantly lower than in group II and group III, respectively [58]. Several trials have been conducted to evaluate markers predictive of response to this drug; the ones that have shown some usefulness and correlation with response to therapy are measurement of plasma mid-regional pro-adrenomedullin (MR-proADM) [59], erythrocyte production of H2S [60], and flow-mediated vasodilation (FMD) [43]. Additionally, copeptin plasma levels (> 10.5 pmol/L) and SBP drops in changing from a supine to an upright position can well predict the long-term asymptomatic survival rate of pediatric POTS patients given oral midodrine hydrochloride [51, 56]. For those who have drug allergies or a blood pressure reading that is higher than 95% of the average for people their age and sex, midodrine is contraindicated. The daily dose of midodrine hydrochloride is advised to be split into several administrations, as it has immediate and fleeting effects (the duration of action of midodrine is approximately 4 h). Due to the possibility of developing hypertension while lying flat, the medication should only be taken during the day and no earlier than 4 h before bed (106); as a result, blood pressure should be monitored while under treatment [61]. This side effect is more common in adults; it is rarely seen in adolescents and the pediatric population.
Some forms of POTS have been shown to be associated with high levels of antibodies against acetylcholine receptors. Pyridostigmine may be useful in this group of patients. Acetylcholinesterase inhibition has been shown to increase aortic and carotid baroreceptor sensitivity and may increase peripheral vascular resistance and reduce symptoms of orthostatic intolerance [62]. A single-center retrospective study including 300 patients aged 26 ± 12 years and POTS demonstrated an improvement in symptoms (fatigue, palpitations, presyncope, and syncope) in patients who received and tolerated pyridostigmine. The reduction in symptoms was correlated with a statistically significant improvement in upright HR and diastolic blood pressure after treatment with pyridostigmine compared to baseline hemodynamic parameters. The overall efficacy of pyridostigmine was seen in 42% of total patients or 52% of patients who could tolerate taking the drug. Gastrointestinal problems were the most common adverse effects reported [63, 64]. Ivabradine is a selective and specific inhibitor of the I(f) current blocker that acts at the level of the sinoatrial node to cause a decrease in HR in patients with sinus rhythm and heart failure (HF) or angina. Ivabradine has shown favorable results in adult patients with POTS and IST. Donne et al. retrospectively evaluated the efficacy of ivabradine in the treatment of POTS in the pediatric population (n = 22) with a median age of 14.5 years. During the median follow-up period of 4.6 months, most participants (68%) reported an improvement in symptoms [65].
Little is known about the long-term prognoses for pediatric patients with POTS. Heterogeneous pathophysiology leads to a common phenotype, but prognosis depends on the underlying etiology [66]. A survey from a single tertiary center conducted by using a mailed questionnaire suggests a good overall prognosis among adolescent patients with POTS, with 86% reporting symptom improvement or resolution at 5. Four years after diagnosis [67]. Another center showed improvements among young adult patients with POTS (aged 20–33 years) over a mean follow-up period of 92 ± 41 months [68].
With regard to the pediatric IST, evidence is very scarce. The only study published to date found that 15.4% of the 479 adolescents enrolled suffered from IST with a 24-h heart rate ≥ 95 bpm. They also found that the risk of IST was higher in adolescents suffering from attention deficit disorder and hypertension [69]. In the case series reported by Atik et al., two children with IST were treated: in the first case, beta-blocker therapy resulted in regression of the patients’ symptoms, whereas in the second case, despite previous treatment with beta-blockers and then with ivabradine, the patients’ symptoms did not improve, and therefore, treatment with midodrine was initiated [67]. A recent analysis comparing 28 adolescents who developed IST (n = 13) and POTS (n = 15) after COVID-19 and/or vaccination versus 64 adolescents who had developed dysautonomia due to psychosomatic diseases prior to the COVID-19 pandemic showed that low-dose propanol and to a lesser extent ivabradine followed by omega-3 significantly reduce elevated HR in patients with IST and increases in HR in patients with POTS and may be useful in these children with dysautonomia regardless of whether it is related to COVID-19 infection or not [70]. Romeo et al. described the case of a 16-year-old adolescent with IST-induced cardiomyopathy. The patient was resistant to treatment with conventional rate-reducing drugs and was therefore started on ivabradine. After 3 months of therapy, an improvement in ejection fraction and an effective reduction in HR was observed in the absence of side effects [71••]. A study evaluated the efficacious and safe dose of ivabradine in children with dilated cardiomyopathy and symptomatic chronic heart failure from ages 6 months to 18 years.
Ivabradine was administered as an oral liquid at an initial dose of 0.02 mg/kg twice daily for children aged 6 to 12 months and 0.05 mg/kg twice daily for children older than 1 year and younger than 3 years or 3 to 18 years and weighing < 40 kg. Liquid ivabradine was specially formulated for this pediatric study and was administered in 10 mL single-dose units containing 1, 5, or 13.3 mg ivabradine (stored at room temperature). The tablet form (adult formulation) was administered to children older than 3 years and weighing ≥ 40 kg with an initial dose of 2.5 mg twice daily. Doses could be adjusted every 2 weeks. The duration of the titration period was governed by the extent of HR reduction and could last up to 8 weeks or until the patient reached the primary endpoint (heart rate reduction ≥ 20% without bradycardia or symptoms of bradycardia). Titration could comprise a maximum of 4 phases so patients weighing ≥ 40 kg who started with 2.5 mg twice daily (tablet form) could be increased to 5, 7.5, 10, and 15 mg twice daily, but each titration was followed by a 2-week maintenance. Ivabradine safely reduced the resting HR of children with chronic heart failure and dilated cardiomyopathy. Adverse events were reported at a similar frequency in both treatment groups (ivabradine and placebo group) [72, 73] (Table 1). Cardiopulmonary testing could be used to assess the efficacy and tolerability of ivabradine in this population (https://www.ema.europa.eu/en/documents/product-information/procoralan-epar-product-information_en.pdf). Although the pathogenetic mechanisms of IST are not yet understood, it has many aspects in common with POTS, so the same pharmacological and non-pharmacological measures are applied in clinical practice as for POTS. Small case series suggest the possibility of using other therapies such as fludrocortisone, phenobarbital, clonidine, and erythropoietin, but there is a lack of randomized trials in this regard [75, 76].
Conclusion
The identification and management of patients with POTS and IST are a growing problem, especially in children and those with long COVID. Although they cause chronic impairment of quality of life, these two diseases are often underdiagnosed and under-recognized. The exact pathogenesis of these two syndromes has not yet been fully elucidated, but it is likely that POTS and IST have many aspects in common. A better understanding of the causal mechanisms would lead to an improvement in therapeutic management, which to date is still unsatisfactory.
The various studies conducted are often monocentric and with a small sample size. In children, the evidence is even poorer. Several biomarkers that can guide the response to drug therapy have been identified but are little used.
To date, the most important thing is interdisciplinary management that assesses case by case and aims firstly at lifestyle modifications, such as diet, fluid intake, and physical activity, and secondly at a targeted pharmacological approach.
Data Availability
Not applicable for this paper.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Olshansky B, Sullivan RM. Inappropriate sinus tachycardia. Europace. 2019;21(2):194–207. https://doi.org/10.1093/europace/euy128.
Ahmed A, Pothineni NVK, Charate R, Garg J, Elbey M, de Asmundis C, LaMeir M, Romeya A, Shivamurthy P, Olshansky B, Russo A, Gopinathannair R, Lakkireddy D. Inappropriate sinus tachycardia: etiology, pathophysiology, and management: JACC review topic of the week. J Am Coll Cardiol. 2022;79(24):2450–62.
Still AM, Raatikainen P, Ylitalo A, Kauma H, Ikäheimo M, Antero Kesäniemi Y, Huikuri HV. Prevalence, characteristics and natural course of inappropriate sinus tachycardia. Europace. 2005;7(2):104–12.
Calkins H. The 2019 ESC guidelines for the management of patients with supraventricular tachycardia. Eur Heart J. 2019;40(47):3812–3. https://doi.org/10.1093/eurheartj/ehz837.
Bryarly M, Phillips LT, Fu Q, Vernino S, Levine BD. Postural orthostatic tachycardia syndrome: JACC focus seminar. J Am Coll Cardiol. 2019;73(10):1207–28. https://doi.org/10.1016/j.jacc.2018.11.059.
• Fedorowski A. Postural orthostatic tachycardia syndrome: clinical presentation, aetiology and management. J Intern Med. 2019;285(4):352–66. https://doi.org/10.1111/joim.12852. Epub 2018 Nov 23. An important guidance on the topic to guide patient management.
Shen WK. How to manage patients with inappropriate sinus tachycardia. Heart Rhythm. 2005;2(9):1015–9. https://doi.org/10.1016/j.hrthm.2005.05.002.
Watari M, Nakane S, Mukaino A, Nakajima M, Mori Y, Maeda Y, Masuda T, Takamatsu K, Kouzaki Y, Higuchi O, Matsuo H, Ando Y. Autoimmune postural orthostatic tachycardia syndrome. Ann Clin Transl Neurol. 2018;5(4):486–92. https://doi.org/10.1002/acn3.524.
Hira R, Baker JR, Siddiqui T, Ranada SI, Soroush A, Karalasingham K, Ahmad H, Mavai V, Ayala Valani LM, Ambreen S, Bourne KM, Lloyd MG, Morillo CA, Sheldon RS, Raj SR. on behalf of the Canadian Long COVID Autonomic Network (CanLoCAN), Objective hemodynamic cardiovascular autonomic abnormalities in post-acute sequelae of COVID-19. Can J Cardiol. 2023; https://doi.org/10.1016/j.cjca.2022.12.002.
Sandroni P, Opfer-Gehrking TL, McPhee BR, Low PA. Postural tachycardia syndrome: clinical features and follow-up study. Mayo Clin Proc. 1999;74(11):1106–10.
Johns Hopkins Coronavirus Resource Center, Cited 2021 Jun 30. 2021 Internet, Available from: https://coronavirus.jhu.edu/data/hubei-timeline
Moghimi N, Di Napoli M, Biller J, Siegler JE, Shekhar R, McCullough LD, Harkins MS, Hong E, Alaouieh DA, Mansueto G, Divani AA. The neurological manifestations of post-acute sequelae of SARS-CoV-2 infection. Curr Neurol Neurosci Rep. 2021;21(9):44.
Venkatesan P. NICE guideline on long COVID. Lancet Respir Med. 2021;9(2):129.
Carfì A, Bernabei R, Landi F. Gemelli Against COVID-19 post-acute care study group. Persistent symptoms in patients after acute COVID-19. JAMA. 2020;324(6):603–5.
Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, Cook JR, Nordvig AS, Shalev D, Sehrawat TS, Ahluwalia N, Bikdeli B, Dietz D, Der-Nigoghossian C, Liyanage-Don N, Rosner GF, Bernstein EJ, Mohan S, Beckley AA, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–15.
NIH launches new initiative to study“LongCOVID”|NationalInstitutesofHealth (NIH), Cited 2021 Apr 22, Internet. 2021 Available from: https://www.nih.gov/about-nih/who-we-are/nih-director/statements/nih-launches-new-initiative-study-long-covid.
Hope AA, Evering TH. Postacute sequelae of severe acute respiratory syndrome coronavirus 2 infection. Infect Dis Clin N Am. 2022;36(2):379–95.
COVID-19 rapid guideline: managing the long-term effects of COVID-19. London: National Institute for Health and Care Excellence (NICE); 2020.
Fedorowski A, Fanciulli A, Raj SR, Sheldon R, Shibao CA, Sutton R. Cardiovascular autonomic dysfunction in post-COVID-19 syndrome: a major health-care burden. Nat Rev Cardiol. 2024; https://doi.org/10.1038/s41569-023-00962-3.
Nalbandian A, Sehgal K, Gupta A, Madhavan MV, McGroder C, Stevens JS, Cook JR, Nordvig AS, Shalev D, Sehrawat TS, Ahluwalia N, Bikdeli B, Dietz D, Der-Nigoghossian C, Liyanage-Don N, Rosner GF, Bernstein EJ, Mohan S, Beckley AA, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–15.
Al-Aly Z, Xie Y, Bowe B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature. 2021;594(7862):259–64.
Phillips S, Williams MA. Confronting our next national health disaster - long-haul COVID. N Engl J Med. 2021;385(7):577–9.
Sudre CH, Murray B, Varsavsky T, Graham MS, Penfold RS, Bowyer RC, Pujol JC, Klaser K, Antonelli M, Canas LS, Molteni E, Modat M, Jorge Cardoso M, May A, Ganesh S, Davies R, Nguyen LH, Drew DA, Astley CM, et al. Attributes and predictors of long COVID. Nat Med. 2021;27(4):626–31.
Huang C, Huang L, Wang Y, Li X, Ren L, Gu X, Kang L, Guo L, Liu M, Zhou X, Luo J, Huang Z, Tu S, Zhao Y, Chen L, Xu D, Li Y, Li C, Peng L, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–32.
Lopez-Leon S, Wegman-Ostrosky T, Perelman C, Sepulveda R, Rebolledo PA, Cuapio A, Villapol S. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. 2021;11(1):16144.
Raman B, Bluemke DA, Luscher TF, Neubauer S. Long COVID: post-acute sequelae of COVID-19 with a cardiovascular focus. Eur Heart J. 2022;43:1157–17.
Visco V, Vitale C, Rispoli A, Izzo C, Virtuoso N, Ferruzzi GJ, Santopietro M, Melfi A, Rusciano MR, Maglio A, Di Pietro P, Carrizzo A, Galasso G, Vatrella A, Vecchione C, Ciccarelli M. Post-COVID-19 syndrome: involvement and interactions between respiratory, Cardiovascular and Nervous Systems. J Clin Med. 2022;11(3):524.
Aranyó J, Bazan V, Lladós G, Dominguez MJ, Bisbal F, Massanella M, Sarrias A, Adeliño R, Riverola A, Paredes R, Clotet B, Bayés-Genís A, Mateu L, Villuendas R. Inappropriate sinus tachycardia in post-COVID-19 syndrome. Sci Rep. 2022;12(1):298.
Low PA, Sandroni P, Joyner M, Shen WK. Postural tachycardia syndrome (POTS). J Cardiovasc Electrophysiol. 2009;20(3):352–8. https://doi.org/10.1111/j.1540-8167.2008.01407.
Tomichi Y, Kawano H, Mukaino A, Chiba A, Doi Y, Arakawa S, Ishimatsu T, Fukae S, Abiru N, Maemura K. Postural orthostatic tachycardia in a patient with type 2 diabetes with diabetic neuropathy. Int Heart J. 2018;59(6):1488–90.
Raj SR, Fedorowski A, Sheldon RS. Diagnosis and management of postural orthostatic tachycardia syndrome. CMAJ. 2022;194(10):E378–85.
Sheldon RS, Grubb BP 2nd, Olshansky B, Shen WK, Calkins H, Brignole M, Raj SR, Krahn AD, Morillo CA, Stewart JM, Sutton R, Sandroni P, Friday KJ, Hachul DT, Cohen MI, Lau DH, Mayuga KA, Moak JP, Sandhu RK, Kanjwal K. 2015 Heart Rhythm Society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015;12(6):e41–63.
Raj SR, Guzman JC, Harvey P, Richer L, Schondorf R, Seifer C, Thibodeau-Jarry N, Sheldon RS. Canadian Cardiovascular Society position statement on postural orthostatic tachycardia syndrome (POTS) and related disorders of chronic orthostatic intolerance. Can J Cardiol. 2020;36(3):357–72.
Foster MC, Levine PA. Use of verapamil to control an inappropriate chronic sinus tachycardia. Chest. 1984;85(5):697–9.
Raj SR, Black BK, Biaggioni I, Paranjape SY, Ramirez M, Dupont WD, Robertson D. Propranolol decreases tachycardia and improves symptoms in the postural tachycardia syndrome: less is more. Circulation. 2009;120(9):725–34.
Cappato R, Castelvecchio S, Ricci C, Bianco E, Vitali-Serdoz L, Gnecchi-Ruscone T, Pittalis M, De Ambroggi L, Baruscotti M, Gaeta M, Furlanello F, Di Francesco D, Lupo PP. Clinical efficacy of ivabradine in patients with inappropriate sinus tachycardia: a prospective, randomized, placebo-controlled, double-blind, crossover evaluation. J Am Coll Cardiol. 2012;60(15):1323–9.
McDonald C, Frith J, Newton JL. Single centre experience of ivabradine in postural orthostatic tachycardia syndrome. Europace. 2011;13(3):427–30.
Kanjwal K, Karabin B, Sheikh M, Elmer L, Kanjwal Y, Saeed B, Grubb BP. Pyridostigmine in the treatment of postural orthostatic tachycardia: a single-center experience. Pacing Clin Electrophysiol. 2011;34(6):750–5.
Abdelnabi M, Saleh Y, Ahmed A, Benjanuwattra J, Leelaviwat N, Almaghraby A. Ivabradine effects on COVID-19-associated postural orthostatic tachycardia syndrome: a single center prospective study. Am J Cardiovasc Dis. 2023;13(3):162–7.
Jadhav K, Jariwala P. ‘Ivabradin’ versus ‘carvedilol’ in the management of post-COVID-19 palpitation with sinus tachycardia. Indian Heart J. 2020;72:S33.
Jacob G, Shannon JR, Black B, Biaggioni I, Mosqueda-Garcia R, Robertson RM, Robertson D. Effects of volume loading and pressor agents in idiopathic orthostatic tachycardia. Circulation. 1997;96(2):575–80.
Lin J, Han Z, Li X, Ochs T, Zhao J, Zhang X, Yang J, Liu P, Xiong Z, Gai Y, Tang C, Du J, Jin H. Risk factors for postural tachycardia syndrome in children and adolescents. PLoS One. 2014;9(12):e113625.
Bryarly M, Phillips LT, Fu Q, Vernino S, Levine BD. Postural orthostatic tachycardia syndrome: JACC focus seminar. J Am Coll Cardiol. 2019;73(10):1207–28.
Zhang Q, Chen X, Li J, Du J. Orthostatic plasma norepinephrine level as a predictor for therapeutic response to metoprolol in children with postural tachycardia syndrome. J Transl Med. 2014;12:249.
Kimpinski K, Figueroa JJ, Singer W, Sletten DM, Iodice V, Sandroni P, Fischer PR, Opfer-Gehrking TL, Gehrking JA, Low PA. A prospective, 1-year follow-up study of postural tachycardia syndrome. Mayo Clin Proc. 2012;87(8):746–52.
Liao Y, Chen S, Liu X, Zhang Q, Ai Y, Wang Y, Jin H, Tang C, Du J. Flow-mediated vasodilation and endothelium function in children with postural orthostatic tachycardia syndrome. Am J Cardiol. 2010;106(3):378–82.
Li J, Zhang Q, Liao Y, Zhang C, Hao H, Du J. The value of acetylcholine receptor antibody in children with postural tachycardia syndrome. Pediatr Cardiol. 2015;36(1):165–70. https://doi.org/10.1007/s00246-014-0981-8. Epub 2014 Aug 3
Blitshteyn S. Autoimmune markers and autoimmune disorders in patients with postural tachycardia syndrome (POTS). Lupus. 2015;24(13):1364–9.
• Petracek LS, Suskauer SJ, Vickers RF, Patel NR, Violand RL, Swope RL, Rowe PC. Adolescent and young adult ME/CFS after confirmed or probable COVID-19. Front Med (Lausanne). 2021;8:668944. An important paper on evidence of POTS in children with ME/CFS and long COVID.
• Kokorelis C, Malone L, Byrne K, Morrow A, Rowe PC. Onset of postural orthostatic tachycardia syndrome (POTS) following COVID-19 infection: a pediatric case report. Clin Pediatr (Phila). 2023;62(2):92–5. An important paper on evidence of POTS in children with ME/CFS and long COVID.
Chen G, Du J, Jin H, Huang Y. Postural tachycardia syndrome in children and adolescents: pathophysiology and clinical management. Front Pediatr. 2020;8:474.
•• Vernino S, Bourne KM, Stiles LE, Grubb BP, Fedorowski A, Stewart JM, Arnold AC, Pace LA, Axelsson J, Boris JR, Moak JP, Goodman BP, Chémali KR, Chung TH, Goldstein DS, Diedrich A, Miglis MG, Cortez MM, Miller AJ, et al. Postural orthostatic tachycardia syndrome (POTS): state of the science and clinical care from a 2019 National Institutes of Health expert consensus meeting - part 1. Auton Neurosci. 2021;235:102828. An important guidance to manage ITS and POTS.
Zhang Q, Chen X, Li J, Du J. Clinical features of hyperadrenergic postural tachycardia syndrome in children. Pediatr Int. 2014;56(6):813–6.
Zhang Q, Xu B, Du J. Update of individualized treatment strategies for postural orthostatic tachycardia syndrome in children. Front Neurol. 2020;11:525. https://doi.org/10.3389/fneur.2020.00525.
Appelman B, Charlton BT, Goulding RP, Kerkhoff TJ, Breedveld EA, Noort W, Offringa C, Bloemers FW, van Weeghel M, Schomakers BV, Coelho P, Posthuma JJ, Aronica E, Joost Wiersinga W, van Vugt M, Wüst RCI. Muscle abnormalities worsen after post-exertional malaise in long COVID. Nat Commun. 2024;15(1):17. https://doi.org/10.1038/s41467-023-44432-3.
Zhao J, Du S, Yang J, Lin J, Tang C, Du J, Jin H. Usefulness of plasma copeptin as a biomarker to predict the therapeutic effectiveness of metoprolol for postural tachycardia syndrome in children. Am J Cardiol. 2014;114(4):601–5.
Writing Committee Members:; panelists:. 2018 Chinese Pediatric Cardiology Society (CPCS) guideline for diagnosis and treatment of syncope in children and adolescents. Sci Bull (Beijing) 2018; 63(23):1558-1564.
Chen L, Wang L, Sun J, Qin J, Tang C, Jin H, Du J. Midodrine hydrochloride is effective in the treatment of children with postural orthostatic tachycardia syndrome. Circ J. 2011;75(4):927–31.
Zhang F, Li X, Ochs T, Chen L, Liao Y, Tang C, Jin H, Du J. Midregional pro-adrenomedullin as a predictor for therapeutic response to midodrine hydrochloride in children with postural orthostatic tachycardia syndrome. J Am Coll Cardiol. 2012;60(4):315–20.
Yang J, Zhao J, Du S, Liu D, Fu C, Li X, Chen S, Tang C, Du J, Jin H. Postural orthostatic tachycardia syndrome with increased erythrocytic hydrogen sulfide and response to midodrine hydrochloride. J Pediatr. 2013;163(4):1169–73.e2.
Deng W, Liu Y, Liu AD, Holmberg L, Ochs T, Li X, Yang J, Tang C, Du J, Jin H. Difference between supine and upright blood pressure associates to the efficacy of midodrine on postural orthostatic tachycardia syndrome (POTS) in children. Pediatr Cardiol. 2014;35(4):719–25. https://doi.org/10.1007/s00246-013-0843-9.
Chen G, Du J, Jin H, Huang Y. Postural tachycardia syndrome in children and adolescents: pathophysiology and clinical management. Front Pediatr. 2020;8:474. https://doi.org/10.3389/fped.2020.00474.
Gales BJ, Gales MA. Pyridostigmine in the treatment of orthostatic intolerance. Ann Pharmacother. 2007;41(2):314–8. https://doi.org/10.1345/aph.1H458.
Kanjwal K, Karabin B, Sheikh M, Elmer L, Kanjwal Y, Saeed B, Grubb BP. Pyridostigmine in the treatment of postural orthostatic tachycardia: a single-center experience. Pacing Clin Electrophysiol. 2011;34(6):750–5. https://doi.org/10.1111/j.1540-8159.2011.03047.x.
Delle Donne G, Rosés Noguer F, Till J, Salukhe T, Prasad SK, Daubeney PEF. Ivabradine in postural orthostatic tachycardia syndrome: preliminary experience in children. Am J Cardiovasc Drugs. 2018;18(1):59–63. https://doi.org/10.1007/s40256-017-0248-x.
Stewart JM, Boris JR, Chelimsky G, Fischer PR, Fortunato JE, Grubb BP, Heyer GL, Jarjour IT, Medow MS, Numan MT, Pianosi PT, Singer W, Tarbell S, Chelimsky TC, Pediatric writing group of the American Autonomic Society, et al. Pediatrics. 2018;141(1):e20171673.
Bhatia R, Kizilbash SJ, Ahrens SP, Killian JM, Kimmes SA, Knoebel EE, Muppa P, Weaver AL, Fischer PR. Outcomes of adolescent-onset postural orthostatic tachycardia syndrome. J Pediatr. 2016;173:149–53.
Sousa A, Lebreiro A, Freitas J, Maciel MJ. Long-term follow-up of patients with postural tachycardia syndrome. Clin Auton Res. 2012;22(3):151–3.
Buchhorn R, Baumann C, Gündogdu S, Rakowski U, Willaschek C. Diagnosis and management of an inappropriate sinus tachycardia in adolescence based upon a Holter ECG: a retrospective analysis of 479 patients. PLoS One. 2020;15(8):e0238139.
Ugan Atik S, Dedeoğlu R, Koka A, Öztunç F. Çocuklarda postüral ortostatik taşikardi sendromu, uygunsuz sinüs taşikardisi ve vazovagal senkop tanı ve tedavisindeki deneyimlerimiz [Our experience in the diagnosis and treatment of postural orthostatic tachycardia syndrome, vasovagal syncope, and inappropriate sinus tachycardia in children]. Turk Kardiyol Dern Ars. 2017;45(3):227–34. Turkish
•• Buchhorn R. Therapeutic approaches to dysautonomia in childhood, with a special focus on long COVID. Children (Basel). 2023;10(2):316. An important guidance on the management of long COVID in children with a focus on dysautonomia.
Romeo E, Grimaldi N, Sarubbi B, D'Alto M, Santarpia G, Scognamiglio G, Russo MG, Calabrò R. A pediatric case of cardiomyopathy induced by inappropriate sinus tachycardia: efficacy of ivabradine. Pediatr Cardiol. 2011;32(6):842–5.
Bonnet D, Berger F, Jokinen E, Kantor PF, Daubeney PEF. Ivabradine in children with dilated cardiomyopathy and symptomatic chronic heart failure. J Am Coll Cardiol. 2017;70(10):1262–72.
Filler G, Gow RM, Nadarajah R, Jacob P, Johnson G, Zhang YL, Christians U. Pharmacokinetics of pyridostigmine in a child with postural tachycardia syndrome. Pediatrics. 2006;118(5):e1563–8.
• Buonsenso D, Morello R, De Rose C, Spera F, Baldi F. Long-term outcome of a child with postcovid condition: role of cardiopulmonary exercise testing and 24-h Holter ECG to monitor treatment response and recovery. Pediatr Pulmonol 2023. An important case report demonstrating how POTS can be diagnosed and monitored during treatment.
Olshansky B, Sullivan RM. Inappropriate sinus tachycardia. J Am Coll Cardiol. 2013;61(8):793–801.
Acknowledgements
We are grateful to Dr. Peter Row, from the Department of Pediatrics, Johns Hopkins University School of Medicine, Baltimore, MD, USA, for his support and mentorship in finalizing this review. Dr. Francesco Raffaele Spera and Dr. Raffaella Mistrulli have been supported by a research grant provided by the DigiCardiopaTh PhD program.
Funding
Open access funding provided by Università Cattolica del Sacro Cuore within the CRUI-CARE Agreement.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Not applicable.
Conflict of Interest
DB has received grants to study Long Covid from Pfizer and Roche. The other authors have no conflicts of interest to declare.
Human and Animal Rights and Informed Consent
Not applicable.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Spera, F.R., Mistrulli, R., Salerno, L. et al. Post-COVID Postural Orthostatic Tachycardia Syndrome and Inappropriate Sinus Tachycardia in the Pediatric Population. Curr Clin Micro Rpt (2024). https://doi.org/10.1007/s40588-024-00217-w
Accepted:
Published:
DOI: https://doi.org/10.1007/s40588-024-00217-w