
Abstract
Background
The numerous restrictive measures implemented during the recent COVID-19 pandemic have reduced the levels of physical activity (PA) carried out by elderly people and telecoaching (TC) could be a training method to maintain the recommended levels of PA. In fact, TC uses information and digital communications technologies, such as computers and mobile devices, to access training services remotely. Thus, this study aimed to systematically review the scientific literature to verify the application, efficacy, and safety of TC training programs.
Methods
PubMed, Scopus, and Web of Sciences databases were used for this review, and randomized controlled trials analyzing TC training programs for elderly people were included. Only articles written in English and published in the last decade were considered.
Results
3 articles were included in the qualitative synthesis including 194 elderly people. The sample size ranged from 12 to 117 and the TC training program from 8 to 12 weeks. The TC training programs were applied to elderly people with metabolic diseases and respiratory diseases. TC training program was effective in elderly people with metabolic diseases while the benefits for respiratory diseases have yet to be clarified.
Conclusion
TC seems to be a safe, effective, and injury-free training method, despite its limited application in elderly population. Future studies should better investigate this training method in elderly people in order to evaluate the effectiveness in a wider range of diseases.
Similar content being viewed by others


Introduction
The world aging process is indisputable, 125 million people are 80 years of age or older [1], altering the social, economic, and health systems of most countries [2]. Population aging is a problem for the present and especially for the future, and the United Nations estimates that the elderly population will reach 2 billion by 2050. This aging process results from the increase in life expectancy, the decrease in birth rates, and the advances in medical care and technology [1]. The European Commission has recently expressed the need to increase scientific research to ensure healthy aging [1]. Indeed, after the age of 40, it is possible to detect a first involution of the physiological systems, involution that develop at a peak near 65 years of age [3, 4]. Aging is a process associated with structural and functional changes in both the physical and mental domains [5]. The mental component is altered due to neurological mechanisms related to aging [6], such as vestibulocochlear degeneration [7], the reduction of cognitive functions [8], and the development of dementia and depression [8], while the physical component is associated with a decreased muscle strength, muscle flexibility, and body balance [7, 9, 10]. All these impairments, associated with a sedentary lifestyle, accelerate the decline of bodily functions [11] and increase the risk of falls [12, 13]. Consequently, to ensure a healthy aging, it is important to develop appropriate health habits such as sleep management, stress management, balanced nutrition, and physical activity (PA) practice [14].
PA has been shown to be effective in encouraging a healthy aging [15]. For example, a regular outdoor walk seems to generate benefits on body balance ability in elderly people and consequently prevent the risk of falls [16]. The benefits of PA in elderly have also been demonstrated in sarcopenia [13] and osteoporosis diseases [17], as well as to improve physical performance such as the range of motion (ROM) of joints. For example, a flexibility training program has been shown to improve spinal ROM in a population of older women [18].
In consideration of the recent COVID-19 pandemic and the relative restrictive measures, it would be useful to increase the duration of the weekly time of PA practice in elderly people [19, 20]. Indeed, the recent COVID-19 pandemic, due to the numerous restrictive measures implemented, has reduced the levels of PA practiced by this population [21, 22]. As a consequence, different strategies have been developed and, among these, telecoaching (TC) seems to result as an effective training setting for maintaining the recommended levels of PA [23, 24]. TC provides the use of information technologies and digital communications, such as computers and mobile devices, to access training services remotely [25]. It is a useful training method for all patients with travel difficulties, who live in different cities, or who prefer to train in a familiar environment such as their own home [26].
Therefore, this systematic review aimed to analyze the application, efficacy, and safety of TC training programs in elderly people.
Methods
Search strategy
For conducting this systematic review the PRISMA guidelines were adopted [27]. The studies were searched in electronic databases such as PubMed, Scopus, and Web of Science. To find studies, the following keywords were used in different combinations: telecoaching, exercise, elderly, training protocol, and training program.
All the articles found were transferred into Endnote software (vers. X9 for Windows 11, © Thomson Reuters).
Eligibility Criteria
All studies that have the following criteria were included in this systematic review: (1) studies with TC as training program for elderly people; (2) original research with full text written in English language; (3) studies published in the last decade; (4) study designs other than reviews, meta-analysis, letter to editors, and theses. No gender differences between males and females were considered for this study.
Study selection
The search of the studies was performed by one author of the research group (I.L.). After removing duplicates, two authors (F.F. and V.G.) independently analyzed the titles and abstracts of all studies. Other two authors (J.B. and M.B.) later analyzed the full text for study inclusion according to the inclusion and exclusion criteria. In case of disagreement of the latter two authors, a negotiation process was carried out and, if necessary, a third author (V.N.) was consulted.
A Microsoft Excel spreadsheet (Microsoft Corp, Redmond, Washington) was used to record the following information related to the included studies: year of publication, sample age, gender, aim of the study, and TC program.
Results
Study Identification
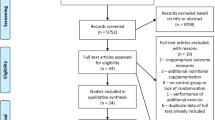
From the search conducted on these databases, a total of 113 studies analyzing the use of TC in elderly were found. 77 were doubled and 33 were eliminated because they did not include elderly subjects, or they analyzed a different topic. Only 3 articles were finally included. In detail, 2 studies aimed to evaluate the effects of TC in elderly suffering from respiratory diseases, while 1 study aimed to evaluate the effects of TC in elderly suffering from metabolic disease. The PRISMA flowchart shows the entire selection process (Fig. 1).

Flow Diagram representing the entire selection process
A total of 194 elderly participants were included and the sample size varied from 12 to 117 while the TC training program lasted from 8 to 12 weeks. Detailed information is provided in Table 1.
Table 2 shows details of the training program and the results found in the articles included.
Respiratory diseases
The first study included in this review was conducted by Cameron-Tucker and colleagues [28] who applied the TC method to patients with chronic obstructive pulmonary disease (COPD) which is a chronic inflammatory disease with non-reversible obstruction of airways [30]. The researchers investigated telephone health mentoring aimed at home-based free walking (TC or experimental group) compared to the usual waiting time (usual care or control group) followed by a training program for each group. Participants were randomized between the two groups (i.e., TC and usual care). TC provided by trained nurse healthcare supported participants’ home-based free walking for 8 weeks, to accumulate 30 min of training per day, preferably every day of the week. Data collection was performed at the baseline (T1), after the TC program (T2), and at the end of the training program of both groups (T3). The primary outcome was a change in physical capacity measured by a 6-min walk test, resulting in highly indicative disease status in patients suffering from respiratory diseases [31]. The results demonstrated no significant changes between time points in the TC group. It follows that in patients with COPD, telephone mentoring for home-based walking has not demonstrated any benefit on exercise capacity.
The second study included in this review was conducted by Hume and colleagues [29]. The researchers evaluated the feasibility and acceptability of a TC training program for lung transplant recipients (LTx). The program included 12 weeks of TC training program. In detail, patients were recruited and randomized into two groups (i.e., TC and usual care). TC involved the use of a pedometer and a smartphone app, with the latter the researchers established periodic PA goals, monitored the activity performed by patients, and dialogued with them if necessary. 86% of participants rated the TC training program positively. The pedometer was used excellently, being used by the patients for 90% of the study period without any negative events. After 12 weeks, only the TC group showed significant improvements in daily steps and movement intensity, while both groups showed significant changes in quality of life (SF-36). In conclusion, TC in patients with LTx appears to be safe, feasible, and well-accepted.
Metabolic diseases
The third study included in this review was the only one that applied TC in elderly patients suffering from metabolic diseases. In detail, Storch and colleagues [32] applied TC in patients with type 2 diabetes mellitus (T2DM). Participants were recruited and randomized into two groups (i.e., the intervention group with the TC training program and the control group with usual care). The TC training program lasted 12 weeks and, through a tablet, a glucometer, and a pedometer, different measures relating to diet, PA, and stress management were recorded. In each phone-based meeting, the participant and the coach individually decided on the patient’s periodic goals to manage the disease. The number of daily steps was monitored continuously through the pedometer and automatically reported each day through Bluetooth. The results showed a greater reduction in glycated hemoglobin (HbA) values in the experimental group compared to the control group. In addition, the analysis conducted on PA demonstrated, although not significant, an increase in terms of average daily steps for the intervention group compared to the control group. However, this increase allowed a significant improvement in the management of the body mass index. It follows that a TC training program could be a new approach to manage disease progression in patients with T2DM.
Discussion
This systematic review aimed to analyze the use of TC training programs in elderly people. Indeed, the average age of the world population is constantly growing and epidemiological studies showed that the number of people aged 60 or more exceeds 11% and is expected to increase reaching 22% in 2050 [33].
This aging process causes an increase in the development of age-related diseases and respiratory and metabolic diseases. One of the major respiratory diseases is COPD. This disease is characterized by bronchial obstruction with a progressive increase in dyspnea generating large physical limitations. For this reason, one of the main objectives to contrast this disease is to limit the sedentary lifestyle. This is demonstrated by the fact that physically active people with COPD have a lower risk of hospitalization and death than sedentary ones. Despite the demonstrated benefits of PA, these patients are still largely sedentary [34]. It follows that exercise professionals should counter the misconceptions related to the practice of PA or exercise in order to motivate individuals to train [35]. In this way, Cameron-Tucker and colleagues applied TC to these patients. Although their results demonstrate that the use of a diary with weekly walking plans and 1 h of weekly exercise does not induce benefits, TC can still be considered a useful method to increase daily PA time. The non-significant results found could depend on the reduced duration of the program, the small sample size, and the small number of tests carried out to evaluate physical efficiency. The 8 weeks of duration with 7 calls for single individual does not seem to be sufficient. Indeed, a systematic review of elderly patients with various chronic diseases demonstrated that 12 or more calls in 6–12 months are effective in increasing PA and improving eating behaviour [36]. Moreover, this study agrees with the scientific literature that 1 h of supervised exercise is insufficient to generate improvements in exercise capacity, supporting that at least two weekly sessions are necessary to improve exercise capacity in these patients [37, 38].
A further disease analyzed in this review refers to elderly with LTx, i.e., patients with end-stage lung disease who require surgery. In recent years, the disease survival rate has improved significantly and the International Society for Heart and Lung Transplantation Registry reports a 5-year survival rate of 59% [39]. It follows that one of the main objectives is to improve physical functions and the related quality of life in this population [40]. The study by Hume and colleagues demonstrated the effectiveness of TC in these patients. In detail, 86% of the participants evaluated this intervention positively stating that this allowed them to increase PA time. On the contrary one study in COPD patients, with the same intervention program, had a 59% satisfaction level [41]. 47.8% of participants with COPD rated goal progression as “high” or “much too high” compared to only 14% of participants with LTx. [41]. These results seem to suggest a greater ambition in choosing physical goals in LTx patients than in COPD patients. This condition could be due to a greater consideration of the role of PA [42] and the clear progress that the practice of PA generates in the symptoms of these patients [43].
The effectiveness of TC in elderly patients was also analyzed in subjects with T2DM. Diabetes is a metabolic disease characterized by chronic hyperglycemia with impairment of carbohydrate metabolism caused by partial or non-secretion of insulin. T2DM is the most common form of diabetes mellitus reaching 90/95% of all patients with diabetes [44]. It is also predicted that patients with this disease could become 439 million by 2030 [45]. The main objective for these patients is to prevent the onset of complications to maintain a high quality of life index [46]. In order to reach this goal, blood sugar levels need to be checked periodically and the American Diabetes Association (ADA) recommends HbA values < 7% [46]. TC program applied by Storch and colleagues allowed a reduction in HbA values from 7% to 6.6%, demonstrating the success of this training method in these patients. In detail, TC intervention has made it possible to increase daily activity with a consequent reduction in a sedentary lifestyle. A further benefit is the prevention of cardiovascular disease and all other complications that lead to death, especially in males with T2DM. It should be noted that high levels of physical fitness are associated with greater insulin sensitivity favouring better management and control of diabetes [47, 48].
Although 30% of elderly people suffer at least one fall per year [49], no literature supporting the application of TC as primary method for preventing falls in the elderly was identified. As reported by Lord and colleagues, one-third of older people experience at least one episode of falling each year [50]. The prevention of falls, due to the constant aging of the world population, is one of the main public health problems. Falls, after road accidents, are the main cause of death related to injuries among elderly subjects in the world [51], resulting in one of the main causes of death for people over 65 years of age [52]. In detail, high levels of PA reduce mortality and fall risk in the range of 30–50% [53–56].
Conclusion
This systematic review highlighted that few studies have been conducted for evaluating the efficacy of TC training programs in elderly people. Despite this, the few studies included in this systematic review demonstrated that this training method seems to be safe, effective, and injury-free. In detail, the findings suggest that TC can be effective in subjects with metabolic diseases while partial results have been recorded in subjects with respiratory diseases.
Considering these results, further studies are needed to analyze the effectiveness of this intervention program. Moreover, future studies should investigate the efficacy of this training method also on different physical performance such as balance ability to evaluate its effects on falls prevention because TC program could increase adherence to the training, thanks to the possibility of overcoming barriers such as costs, time, travel, and facilities.
Data availability
Data are available upon reasonable request to the corresponding author.
References
Directorate-General for Economic and Financial Affairs (2018) The 2018 ageing report: economic and budgetary projections for the EU member states (2016–2070). Institutional Paper 079, Brussels. https://doi.org/10.2765/615631
World-Health-Organization (2017) Depression and other common mental disorders: global health estimates. https://apps.who.int/iris/handle/10665/254610
Boss GR, Seegmiller JE (1981) Age-related physiological changes and their clinical significance. West J Med 135:434–440
Kendrick D, Kumar A, Carpenter H et al (2014) Exercise for reducing fear of falling in older people living in the community. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD009848.pub2
Moher D, Liberati A, Tetzlaff J et al (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 6:e1000097. https://doi.org/10.1371/journal.pmed.1000097
Bishop NA, Lu T, Yankner BA (2010) Neural mechanisms of ageing and cognitive decline. Nature 464:529–535. https://doi.org/10.1038/nature08983
Benavent-Caballer V, Rosado-Calatayud P, Segura-Ortí E et al (2014) Effects of three different low-intensity exercise interventions on physical performance, muscle CSA and activities of daily living: a randomized controlled trial. Exp Gerontol 58:159–165. https://doi.org/10.1016/j.exger.2014.08.004
Zecevic AA, Salmoni AW, Speechley M et al (2006) Defining a fall and reasons for falling: comparisons among the views of seniors, health care providers, and the research literature. Gerontologist 46:367–376. https://doi.org/10.1093/geront/46.3.367
Daley MJ, Spinks WL (2000) Exercise, mobility and aging. Sports Med 29:1–12. https://doi.org/10.2165/00007256-200029010-00001
Pêgo-Fernandes PM, Abrão FC, Fernandes FL et al (2009) Spirometric assessment of lung transplant patients: one year follow-up. Clinics (Sao Paulo) 64:519–525. https://doi.org/10.1590/s1807-59322009000600006
Inouye SK, Studenski S, Tinetti ME et al (2007) Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc 55:780–791. https://doi.org/10.1111/j.1532-5415.2007.01156.x
Kramarow E, Chen LH, Hedegaard H et al (2015) Deaths from unintentional injury among adults aged 65 and over: United States, 2000–2013. NCHS Data Brief 199:199
Zhao H, Cheng R, Song G et al (2022) The effect of resistance training on the rehabilitation of elderly patients with sarcopenia: a meta-analysis. Int J Environ Res Public Health. https://doi.org/10.3390/ijerph192315491
Friedman SM (2020) Lifestyle (Medicine) and healthy aging. Clin Geriatr Med 36:645–653. https://doi.org/10.1016/j.cger.2020.06.007
Spruit MA, Singh SJ, Garvey C et al (2013) An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med 188:e13-64. https://doi.org/10.1164/rccm.201309-1634ST
Battaglia G, Giustino V, Messina G et al (2020) Walking in natural environments as geriatrician’s recommendation for fall prevention: preliminary outcomes from the “Passiata Day” Model. Sustainability 12:2684
Wietlisbach M, Benden C, Koutsokera A et al (2020) Perceptions towards physical activity in adult lung transplant recipients with cystic fibrosis. PLoS ONE 15:e0229296. https://doi.org/10.1371/journal.pone.0229296
Battaglia G, Bellafiore M, Caramazza G et al (2014) Changes in spinal range of motion after a flexibility training program in elderly women. Clin Interv Aging 9:653–660. https://doi.org/10.2147/cia.S59548
Chambonniere C, Lambert C, Tardieu M et al (2021) Physical Activity and Sedentary Behavior of Elderly Populations during Confinement: Results from the FRENCH COVID-19 ONAPS Survey. Exp Aging Res 47:401–413. https://doi.org/10.1080/0361073x.2021.1908750
Genin PM, Lambert C, Larras B et al (2021) How did the COVID-19 confinement period affect our physical activity level and sedentary behaviors? Methodology and first results from the French National ONAPS Survey. J Phys Act Health 18:296–303. https://doi.org/10.1123/jpah.2020-0449
Giustino V, Parroco AM, Gennaro A et al (2020) Physical activity levels and related energy expenditure during COVID-19 quarantine among the sicilian active population: a cross-sectional online survey study. Sustainability. https://doi.org/10.3390/su12114356
Gjaka M, Feka K, Bianco A et al (2021) The Effect of COVID-19 Lockdown Measures on Physical Activity Levels and Sedentary Behaviour in a Relatively Young Population Living in Kosovo. J Clin Med. https://doi.org/10.3390/jcm10040763
de Vasconcelos HCA, Lira Neto JCG, de Araújo MFM et al (2018) Telecoaching programme for type 2 diabetes control: a randomised clinical trial. Br J Nurs 27:1115–1120. https://doi.org/10.12968/bjon.2018.27.19.1115
Owino V, Yang SY, Goldspink G (2001) Age-related loss of skeletal muscle function and the inability to express the autocrine form of insulin-like growth factor-1 (MGF) in response to mechanical overload. FEBS Lett 505:259–263. https://doi.org/10.1016/s0014-5793(01)02825-3
Institute of Medicine Committee on Evaluating Clinical Applications T (1996) The National Academies Collection: Reports funded by National Institutes of Health. In: Field MJ (ed) Telemedicine: a guide to assessing telecommunications in health care. National Academies Press, National Academy of Sciences, Washington (DC)
Colorado-State-University (2016) Telecoaching emerges as tool in nutrition and medicine. Retrieved from https://source.colostate.edu/telecoaching-emerges-as-tool-in-nutrition-and-medicine/. Accessed 5 Jul 2016
Odnoletkova I, Goderis G, Nobels F et al (2016) Optimizing diabetes control in people with Type 2 diabetes through nurse-led telecoaching. Diabet Med 33:777–785. https://doi.org/10.1111/dme.13092
Cameron-Tucker HL, Wood-Baker R, Joseph L et al (2016) A randomized controlled trial of telephone-mentoring with home-based walking preceding rehabilitation in COPD. Int J Chron Obstruct Pulmon Dis 11:1991–2000. https://doi.org/10.2147/copd.S109820
Hume E, Muse H, Wallace K et al (2022) Feasibility and acceptability of a physical activity behavioural modification tele-coaching intervention in lung transplant recipients. Chron Respir Dis 19:14799731221116588. https://doi.org/10.1177/14799731221116588
von Storch K, Graaf E, Wunderlich M et al (2019) Telemedicine-assisted self-management program for type 2 diabetes patients. Diabetes Technol Ther 21:514–521. https://doi.org/10.1089/dia.2019.0056
Guyatt GH, Sullivan MJ, Thompson PJ et al (1985) The 6-minute walk: a new measure of exercise capacity in patients with chronic heart failure. Can Med Assoc J 132:919–923
Watson SL, Weeks BK, Weis LJ et al (2015) Heavy resistance training is safe and improves bone, function, and stature in postmenopausal women with low to very low bone mass: novel early findings from the LIFTMOR trial. Osteoporos Int 26:2889–2894. https://doi.org/10.1007/s00198-015-3263-2
Keller K, Engelhardt M (2013) Strength and muscle mass loss with aging process. Age and strength loss. Muscles Ligaments Tendons J 3:346–350
Bernard P, Hains-Monfette G, Atoui S et al (2018) Daily objective physical activity and sedentary time in adults with COPD using spirometry data from Canadian Measures Health Survey. Can Respir J 2018:9107435. https://doi.org/10.1155/2018/9107435
Costello E, Kafchinski M, Vrazel J et al (2011) Motivators, barriers, and beliefs regarding physical activity in an older adult population. J Geriatr Phys Ther 34:138–147. https://doi.org/10.1519/JPT.0b013e31820e0e71
Eakin EG, Lawler SP, Vandelanotte C et al (2007) Telephone interventions for physical activity and dietary behavior change: a systematic review. Am J Prev Med 32:419–434. https://doi.org/10.1016/j.amepre.2007.01.004
Bolton CE, Bevan-Smith EF, Blakey JD et al (2013) British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax 68 Suppl 2:i1-30. https://doi.org/10.1136/thoraxjnl-2013-203808
Tripathi BK, Srivastava AK (2006) Diabetes mellitus: complications and therapeutics. Med Sci Monit 12:Ra130-147
Bos S, Vos R, Van Raemdonck DE et al (2020) Survival in adult lung transplantation: where are we in 2020? Curr Opin Organ Transplant 25:268–273. https://doi.org/10.1097/mot.0000000000000753
Loeckx M, Rabinovich RA, Demeyer H et al (2018) Smartphone-based physical activity telecoaching in chronic obstructive pulmonary disease: mixed-methods study on patient experiences and lessons for implementation. JMIR Mhealth Uhealth 6:e200. https://doi.org/10.2196/mhealth.9774
Lord SR, Ward JA, Williams P et al (1993) An epidemiological study of falls in older community-dwelling women: the Randwick falls and fractures study. Austral J Public Health 17:240–245
World-Health-Organization (2015) Ageing and health report
Sherrington C, Whitney JC, Lord SR et al (2008) Effective exercise for the prevention of falls: a systematic review and meta-analysis. J Am Geriatr Soc 56:2234–2243. https://doi.org/10.1111/j.1532-5415.2008.02014.x
Vestbo J, Hurd SS, Agustí AG et al (2013) Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med 187:347–365. https://doi.org/10.1164/rccm.201204-0596PP
Chen L, Magliano DJ, Zimmet PZ (2011) The worldwide epidemiology of type 2 diabetes mellitus–present and future perspectives. Nat Rev Endocrinol 8:228–236. https://doi.org/10.1038/nrendo.2011.183
Davies MJ, D’Alessio DA, Fradkin J et al (2018) A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetes Care 41:2669–2701. https://doi.org/10.2337/dci18-0033
Balkau B, Mhamdi L, Oppert JM et al (2008) Physical activity and insulin sensitivity: the RISC study. Diabetes 57:2613–2618. https://doi.org/10.2337/db07-1605
Helmrich SP, Ragland DR, Leung RW et al (1991) Physical activity and reduced occurrence of non-insulin-dependent diabetes mellitus. N Engl J Med 325:147–152. https://doi.org/10.1056/nejm199107183250302
Gillespie LD, Gillespie WJ, Robertson MC et al (2003) Interventions for preventing falls in elderly people. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.Cd000340
Merchant RA, Morley JE, Izquierdo M (2021) Editorial: exercise, aging and frailty: guidelines for increasing function. J Nutr Health Aging 25:405–409. https://doi.org/10.1007/s12603-021-1590-x
Langer D (2021) Addressing the changing rehabilitation needs of patients undergoing thoracic surgery. Chron Respir Dis 18:1479973121994783. https://doi.org/10.1177/1479973121994783
CDCCfDCaP (2006) Fatalities and injuries from falls among older adults–United States, 1993–2003 and 2001–2005. MMWR Morb Mortal Wkly Rep 55:1221–1224
Battaglia G, Bellafiore M, Bianco A et al (2010) Effects of a dynamic balance training protocol on podalic support in older women. Pilot Study Aging Clin Exp Res 22:406–411. https://doi.org/10.1007/bf03337736
Bellafiore M, Battaglia G, Bianco A et al (2011) Improved postural control after dynamic balance training in older overweight women. Aging Clin Exp Res 23:378–385. https://doi.org/10.1007/bf03337762
Bembom O, van der Laan M, Haight T et al (2009) Leisure-time physical activity and all-cause mortality in an elderly cohort. Epidemiology 20:424–430. https://doi.org/10.1097/EDE.0b013e31819e3f28
Gillespie LD, Robertson MC, Gillespie WJ et al (2012) Interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD007146.pub3
Funding
Open access funding provided by Università degli Studi di Palermo within the CRUI-CARE Agreement. No funding was received for conducting this study. The authors declare they have no financial interests.
Author information
Authors and Affiliations
Contributions
Conceptualization: Giuseppe Battaglia, Ligia J. Dominguez, Giuseppe Messina; Methodology: Ignazio Leale, Flavia Figlioli, Valerio Giustino, Jessica Brusa, Antonino Patti; Formal analysis and investigation: Ignazio Leale, Flavia Figlioli, Valerio Giustino, Jessica Brusa, Matteo Barcellona, Valerio Nocera; Writing-original draft preparation: Ignazio Leale, Flavia Figlioli; Writing-review and editing: Valerio Giustino, Jessica Brusa; Supervision: Giuseppe Battaglia, Ligia J. Dominguez, Mario Barbagallo, Antonio Palma.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no competing interests to declare that are relevant to the content of this article.
Statement of human and animal rights
This article does not contain any studies with human participants or animals performed by any of the authors.
Informed consent
For this type of study, formal consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Leale, I., Figlioli, F., Giustino, V. et al. Telecoaching as a new training method for elderly people: a systematic review. Aging Clin Exp Res 36, 18 (2024). https://doi.org/10.1007/s40520-023-02648-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s40520-023-02648-9