
Abstract
Introduction
Surveillance programs after hepatitis B surface antigen (HBsAg) loss are not yet well established, and the role of hepatitis B surface antibodies (anti-HBs) remains controversial. We aimed to evaluate the risk factors for increased mortality and the association between anti-HBs and all-cause and cause-specific mortality in a representative US (United States) population of patients with resolved HBV (Hepatitis B virus) infections.
Methods
Data were taken from the US National Health and Nutrition Examination Survey (NHANES) 1999–2018. A total of 3455 US adults with resolved HBV infection [defined as hepatitis B surface antigen (HBsAg) negative/anti-hepatitis B core antigen (anti-HBc) positive] were enrolled in this study. The primary outcome measures were all-cause and cause-specific mortality from baseline until 31 December 2019.
Results
During a mean follow-up of 10.3 years, 741 deaths occurred. Age, race, marital status, smoking status, physical activity level, and presence of cirrhosis, diabetes, cardiovascular diseases, chronic obstructive pulmonary diseases, cancer, and anti-HBs were significant factors for increased mortality, and a nomogram tool was developed and validated for the risk stratification of mortality. Compared with participants who were anti-HBs positive, those who were anti-HBs negative had a 23% (hazard ratio 1.23, 95% CI 1.02–1.46) higher risk of all-cause mortality in NHANES 1999–2018. For cause-specific mortality, the fully adjusted hazard ratios of participants who were anti-HBs negative were 0.71 (95% CI 0.48–1.06) for heart disease, 1.44 (95% CI 1.01–2.05) for cancer, and 1.44 (95% CI 1.13–1.83) for other conditions, compared to those of participants who were anti-HBs positive.
Conclusions
Among US adults with resolved HBV infections, anti-HBs-negative status was associated with an increased risk of death from all causes and cancer, implying that the role of anti-HBs in resolved HBV infection should not be ignored. On the public health level, more rigorous surveillance was needed for populations of individuals who were isolated anti-HBc positive.
Similar content being viewed by others

Why carry out this study? |
Surveillance programs after HBsAg loss are not yet well established, and the role of anti-HBs remains controversial. |
What was learned from this study? |
By investigating 3455 patients with resolved HBV infection with an average of 10.3 years of follow-up, we observed that anti-HBs-negative status was associated with an increased risk of death from all causes and cancer, implying that more rigorous surveillance was needed for populations of individuals who were isolated anti-HBc positive. |
In addition, a nomogram tool was developed and validated for the risk stratification of mortality among patients with resolved HBV infections, which may be a valuable reference for surveillance-related decision-making. |
Introduction
With high morbidity and mortality, hepatitis B virus (HBV) infection remains a significant global public health problem [1]. Loss of hepatitis B surface antigen (HBsAg) is recognized as the optimal therapeutic endpoint of HBV infection and also a safe endpoint for stopping acute or chronic hepatitis B treatment, known as “resolved hepatitis B” or “functional cure” [2, 3].
However, even if HBsAg loss is achieved, in some cases, HBV cannot be eradicated because of the persistence of covalently closed circular DNA (cccDNA) and HBV DNA integration. Thus, there is still a risk of HBsAg seroreversion, HBV reactivation, cirrhosis, and hepatocellular carcinoma [4,5,6]. Patients with resolved hepatitis B still have a significantly increased mortality compared with those without chronic liver disease [7]. Thus, surveillance should be continued after HBsAg loss [4,5,6]. Rigorous surveillance of the entire population of resolved HBV infections is neither necessary nor likely to be cost-effective. Risk stratification and targeted surveillance strategies may be necessary. Nevertheless, surveillance programs after HBsAg loss are not yet well established, and the role of anti-HBs (hepatitis B surface antibodies) remains controversial.
There is ongoing controversy over the guidelines for whether anti-HBs seroconversion should be included in the definition of “resolved hepatitis B” or “functional cure”. As stated in the AASLD Guidelines, “loss of HBsAg with acquisition of anti-HBs has been termed functional cure” [3]. In the EASL 2017 Clinical Practice Guidelines, the functional cure or resolved hepatitis B was described as the loss of HBsAg (with or without anti-HBs seroconversion) [1], which seems to imply that isolated anti-HBc (HBsAg negative/anti-HBs negative/anti-HBc positive) is also included in resolved hepatitis B. Such a difference in terminological definition leads to confusion in clinical practice. Previous studies have reported that anti-HBs could provide long-term protection for people who are vaccinated and healthy by clearing circulating HBsAg [8, 9]. However, the role of anti-HBs for populations who achieved HBsAg loss in acute or chronic hepatitis B remains unclear, especially in the long-term prognosis of this population. Elucidating the role of anti-HBs on the long-term prognosis after HBsAg loss could provide evidence for a reasonable definition of HBV “functional cure” or “resolved hepatitis B” and for the choice of primary efficacy endpoints in clinical practice [10].
Therefore, by using the data from the updated NHANES (1999–2018) with long-term follow-up, we intend to investigate which factors are associated with a higher risk of death after HBsAg loss, with a particular focus on the association of anti-HBs with all-cause and cause-specific mortality among US adults with resolved HBV infection.
Methods
Data Source and Study Population
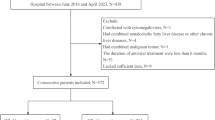
The National Health and Nutrition Examination Survey (NHANES), conducted by the National Center for Health Statistics (NCHS), is a program to assess the health and nutritional status of adults and children in the USA over time [11]. The NHANES used a complex, multistage, probability sampling method to collect nationally representative health-related data on the US population [11]. The NHANES 1999–2018 survey included an interview, physical examination, and laboratory measurements in 55,081 adults (aged 20 or over). In the current analysis, we included participants with resolved HBV infection (defined as serum HBsAg negative and anti-HBc positive) from the continuous NHANES 1999–2018. Those with missing information on anti-HBs (n = 5) and mortality (n = 9) were excluded from the analysis. Therefore, a total number of 3455 participants were included in our cohort for analysis. Among them, 2645 participants were anti-HBs positive, and 810 participants were anti-HBs negative (isolated anti-HBc). The mortality follow-up was a prospective study of the vital status of all participants aged 20 and older to December 2019 (Fig. 1).

Flowchart of inclusion and exclusion of participants
All data used in this study were published free of charge by NCHS. The study was conducted according to the principles of the Helsinki Declaration. The approval of the study from the NCHS ethics review board was waived because the research relied upon publicly available, deidentified secondary data. All participants signed informed consent forms.
Hepatitis B Surface Antibody and Covariates
Qualitative results of hepatitis B surface antibody, hepatitis B surface antigen, and hepatitis B core antibody were available through baseline laboratory data for continuous NHANES (1999–2018) data sets. All HBV tests were performed once at baseline. Definitions of anti-HBs positivity and descriptions of laboratory methodology and eligible samples were available through NHANES laboratory method manuals [12]. Briefly, the AUSAB EIA for anti-HBs uses the “sandwich principle”, a solid-phase enzyme-linked immunoassay technique to detect anti-HBs levels in serum or plasma. Polystyrene beads coated with human HBsAg are incubated with either the patient specimen or the appropriate controls [12]. An initial result of < 5.00 mIU/mL indicates a “negative” sample for anti-HBs. An initial of ≥ 12.0 mIU/mL indicates a “positive” sample for anti-HBs. An initial result of ≥ 5.00 and < 12.0 mIU/mL (“indeterminate”) indicates a sample that requires duplicate repeat testing for anti-HBs (Supplementary Material Fig. S1) [12].
Information on covariates was available through baseline questionnaires, including age, sex, race/ethnicity, education level, marital status, smoking status, drinking status, body mass index, leisure time physical activity level (0, 1–2, or ≥ 3 times/week) [13], healthy eating index scores (HEI-2015) [14], and self-reported baseline history of diabetes, hypertension, cardiovascular diseases, chronic obstructive pulmonary diseases (COPD), liver condition, and cancers. Chronic hepatitis C (CHC) was defined as being hepatitis C virus RNA positive. Low to moderate drinkers were defined as drinking < 1 drink/day in women and < 2 drinks/day in men and heavy drinkers were defined as ≥ 1 drink/day in women and ≥ 2 drinks/day in men. Detailed definitions of covariates are provided in Supplementary Material Table S1.
We employed APRI (AST to platelet ratio index) and FIB-4 (fibrosis-4) scores to assess the severity of liver fibrosis. The scores were calculated for participants with available aspartate aminotransferase (AST), alanine aminotransferase (ALT), and platelet count data from baseline laboratory data. The details of the calculation formula has been described elsewhere [15, 16]. Cirrhosis/ advanced fibrosis was defined by an FIB-4 score > 3.25 or an APRI score > 2.0 in the current study [15, 16].
Ascertainment of Deaths
The baseline was defined as the time the participants underwent physical examination, and the primary outcomes for our study were all-cause mortality from baseline to 31 December 2019. Here, the 10th revision of the International Classification of Diseases was used to classify causes of death. Our secondary outcomes were mortality from heart disease (codes I00–I09, I11, I13, and I20–I51) and cancer (codes C00–C97). Using a unique study identifier, we determined death status by matching it with the National Death Index. Further details of the matching method are available from the NCHS [17].
Statistical Analysis
We accounted for the complex survey design and sampling weights for continuous NHANES (1999–2018) data sets. Less than 10% of values of covariates were missing, except for drinking status, healthy eating index score, and vaccination status. We performed multiple imputations for all missing values. The characteristics of the participants were compared using the Rao-Scott χ2 test, and the analysis of variance was adjusted for sampling weights when appropriate.
Univariate and multivariate Cox regressions (stepwise) were used to confirm which factors were associated with a higher risk of death. To establish and validate a nomogram tool for mortality risk stratification among resolved HBV infection, we divided the study cohort (complete case removed participants with missing values; n = 2403) into a training cohort (NHANES cycles 1, 3, 5, 7, and 9; n = 1237) and a validation cohort (NHANES cycles 2, 4, 6, 8 and 10; n = 1166). The training cohort fitted the penalized Cox model using an adaptive elastic net regularization method. Bootstrap-based validation and calibration were used in both the training and validation cohorts.
Multivariate Cox regression was used to calculate the hazard ratios (HRs) and 95% confidence intervals for mortality with hepatitis B surface antibody. Covariates that may affect mortality were considered in the analysis. We adjusted for baseline age, sex, and race/ethnicity in model 1. We further adjusted for education level, marital status, body mass index, alcohol intake/consumption, and smoking status in model 2. Finally, we further adjusted for healthy eating index scores, leisure time physical activity level, diabetes, hypertension, cardiovascular diseases, emphysema or chronic bronchitis, cancer, cirrhosis, HCV, and liver condition in model 3.
To balance the confounding factors, we performed propensity score matching (PSM) for anti-HBs-positive and anti-HBs-negative participants. The matched covariates included age, sex, race, BMI, educational level, smoking, drinking, diabetes, hypertension, emphysema or chronic bronchitis, and cardiovascular diseases. To unravel the potentially distinct roles of anti-HBs in mortality among individuals of different sexes, races, ages, and chronic diseases, we performed stratified analyses by baseline age, sex, race, BMI, hepatitis B vaccination, and chronic diseases. To evaluate the effect of premature death, we examined the relationships with deaths occurring before 65 years old, before 70 years old, before 75 years old, and before 80 years old among participants younger than 65 years old at baseline.
We also performed a series of sensitivity analyses to test the robustness of the results. First, we removed participants with missing covariate values and ran complete case analyses. Second, hepatitis C infection can be another liver injury source affecting the APRI and FIB-4 index scores. And for patients with chronic hepatitis B who achieved HBsAg loss, chronic liver disease (such as liver cirrhosis) during their HBsAg carriage phase may also add bias. Thus, patients with liver cirrhosis (based on APRI and FIB-4 scores) or patients with CHC were also excluded to verify the results.
All statistical analyses were performed using SAS 9.4 (SAS Institute Inc, Cary, NC), which allows appropriate use of the NHANES survey weights to project the results to the noninstitutionalized general population of the USA. R software (R Foundation for Statistical Computing, Vienna, Austria) and package “survminer” and “hdnom” were used to plot Kaplan–Meier curves and nomograms. Results with a P value < 0.05 were considered statistically significant.
Results
Baseline Characteristics
Out of 101,316 participants in NHANES 1999–2018, 3455 participants (3.4%) met the inclusion criteria (age > 20 years, serum HBsAg negative, and anti-HBc positive). Among them, 2645 subjects were anti-HBs positive and 810 were anti-HBs negative (isolated anti-HBc). Table 1 shows the baseline characteristics of the study participants. Most participants (73.7%) had never been vaccinated against hepatitis B. Among them, HBV infection in 249 (7.21%) subjects was complicated with CHC, and HBV infection in 142 (4.11%) subjects was complicated with cirrhosis. Few participants (6.52%) are aware of hepatitis B, and a tiny minority of participants (0.86%) have ever received treatment for hepatitis B.
Risk Factors for Increased Mortality Among Individuals with Resolved HBV Infection
Among 3455 participants in NHANES 1999–2018, 741 deaths occurred during a mean follow-up of 10.3 years (cumulative mortalities comprised 21.4%). For cause-specific deaths, the cumulative mortalities were 5.8% for heart disease (201 deaths), 4.6% for cancer (162 deaths), and 10.9% for other illnesses (378 deaths). Univariate and multivariate Cox regressions (stepwise) were used to confirm which factors were associated with a higher risk of death. Hazard ratios (HRs) and 95% confidence intervals for mortality are listed in Table 2. Participants who were older, male, having low education, non-Hispanic white, having smoker status, having low physical activity, having coexisting cirrhosis or chronic diseases, unvaccinated against hepatitis B, and anti-HBs negative had higher mortality. When multivariate Cox analysis was used, age, race, marital status, smoking status, physical activity level, cirrhosis, diabetes, cardiovascular diseases, COPD, cancer, and anti-HBs were significant risk factors (Table 2). The results remained almost unchanged when we removed participants with missing values for covariates (Supplementary Material Table S2).
Establishment and Validation of a Nomogram Tool for Mortality Risk Stratification Among Individuals with Resolved HBV Infection
A nomogram for predicting 10-year mortality was established on the basis of penalized Cox regression analysis in the training cohort (Fig. 2). In the nomogram, the status of each predictor is projected through a straight line to the upper limit of the rating scale, giving the corresponding score. The total score of each predictor was summed to calculate the total score. The predicted probability of 10-year mortality can be obtained by projecting the overall score line directly onto the bottom probability scale line.

Nomogram for predicting 10-year mortality among individuals with resolved HBV infections
The bootstrap-based validation results in the training and validation cohorts were stable. The time-dependent AUC (area under the ROC curve) differs from 0.78 to 0.83 in the training cohorts and 0.75 to 0.85 in the validation cohort (Fig. 3a). We also split the samples into three risk groups; the differences in survival time for different risk groups are shown in Fig. 3b. The model calibration results are summarized in Fig. 3c.

Bootstrap-based validation and calibration in training and validation cohorts. a Time-dependent AUC at each time point in the training cohort and validation cohorts; b the differences in survival time for different risk groups with Kaplan–Meier survival curves; c the model calibration results
Relationships Between Anti-HBs and Mortality Among Individuals with Resolved HBV Infection
Table 3 shows the baseline characteristics of study participants across hepatitis B surface antibody statuses in the NHANES 1999–2018. Of the 3455 participants, 810 (23.44%) were anti-HBs negative (isolated anti-HBc). Compared with people in the anti-HBs-positive group, the individuals in the anti-HBs-negative group were more likely to be male, elderly, less educated, currently smoking, and diagnosed with diabetes and hypertension. These indices became comparable after PSM. Participants who were anti-HBs negative had a higher self-reported liver condition (p < 0.001), percentage of HCV RNA positivity (p < 0.001), and higher FIB-4 score (p = 0.002) than participants who were anti-HBs positive. After PSM, those trends remained similar.
Anti-HBs-negative individuals had higher all-cause mortality than anti-HBs-positive populations, which remained statistically significant after the removal of cirrhosis or CHC or after PSM (Fig. 4). Table 4 summarizes the association between hepatitis B surface antibodies and all-cause mortality. After adjustment for age, sex, race/ethnicity, education level, marital status, body mass index, alcohol use, smoking status, diabetes, hypertension, cardiovascular diseases, emphysema or chronic bronchitis, cancer, cirrhosis, CHC, and liver condition, participants who were anti-HBs negative demonstrated a significantly higher association with all-cause mortality (aHR 1.23, 95% CI 1.02–1.46). The results remained almost unchanged when we removed participants with missing values for covariates, excluded participants with positive HCV RNA or liver cirrhosis, or even after propensity score matching. For cause-specific mortality, compared with anti-HBs-positive participants, the fully adjusted hazard ratios in participants who were anti-HBs negative in NHANES 1999–2018 were 0.71 (95% CI 0.48–1.06) for heart disease, 1.44 (95% CI 1.01–2.05) for cancer, and 1.44 (95% CI 1.13–1.83) for other diseases. Individuals who were anti-HBs negative had a significant increase in cancer mortality (Fig. 4 and Table 4). The results remained unchanged when we removed participants with missing values for covariates, and excluded participants with positive HCV RNA or liver cirrhosis. However, this association was only borderline significant after propensity score matching (aHR 1.416, 95% CI 0.965–2.077, P = 0.076). In the subgroup analyses, compared with their counterparts, the associations between anti-HBs and mortality were more substantial among participants who were younger than 65 years old, male, of other ethnicities, and without chronic diseases (Fig. 5). When stratified by age at death to evaluate the effect on premature death, the associations were similar to our main results (Supplementary Material Table S3).

Kaplan–Meier estimates of overall survival in NHANES 1999–2018. Participants were assigned by hepatitis B surface antibody. a All cases; P for all cause < 0.001; P for cancer = 0.002. b Participants with cases of CHC and cirrhosis removed; P for all cause < 0.001; P for cancer = 0.036

Associations between hepatitis B surface antibody and risk of all-cause mortality stratified by baseline sex, race, age, BMI, hepatitis B vaccination status, and chronic diseases diagnoses in NHANES 1999–2018. Risk estimates were adjusted for baseline age (not adjusted in subgroup analysis by age), sex (not adjusted in subgroup analysis by sex), and race/ethnicity (not adjusted in subgroup analysis by race)
Discussion
Surveillance procedures after HBsAg loss are not well established, and the role of anti-HBs remains controversial. In this national population-based prospective cohort study, individuals who were older, male, non-Hispanic white, unvaccinated against hepatitis B and anti-HBs negative, and those who had lower education and physical activity levels, current smoking status, and coexisting cirrhosis or chronic diseases had higher mortality among patients with resolved HBV infections. In particular, anti-HBs-negative status was associated with an increased risk of death from all causes and cancer for adults with resolved HBV infections. Our data revealed that the role of anti-HBs in resolved HBV infection should not be ignored, and more rigorous surveillance is needed for isolated anti-HBc-positive populations.
Comparison with Other Studies
Rigorous surveillance of the entire population of individuals with resolved HBV infections is neither necessary nor likely to be cost-effective. Risk stratification and targeted surveillance strategies may be needed. Surveillance procedures after HBsAg loss are not well established, and there are few related reports. Recently, a study has shown that age, cirrhosis, family history of HCC, and alcohol consumption can independently predict HCC development after HBsAg loss in highly endemic settings [18]. However, that study did not consider outcomes other than HCC (such as cirrhosis, HBsAg seroreversion, and HBV reactivation). All-cause mortality is one of the most critical and final health outcome indicators. Risk factors for increased mortality among US adults with resolved HBV infection remain unclear. In our analysis, age, race, marital status, smoking status, physical activity level, cirrhosis, and self-reported diagnoses of diabetes, cardiovascular diseases, COPD, cancer, and anti-HBs were significant factors for increased mortality. We also developed and validated a nomogram tool for risk stratification of mortality among individuals with resolved HBV infections, which can provide a valuable reference for surveillance decisions.
As a common indicator of hepatitis B and immune status screening, we paid special attention to the role of anti-HBs. Previous studies have focused on hepatocellular carcinoma risk after HBsAg loss, most of which achieved favorable clinical outcomes compared to viral suppression without HBsAg loss [19,20,21]. However, despite the protective effect of HBsAg loss, the role of anti-HBs seroconversion remains controversial. Some studies have noted that anti-HBs seroconversion does not affect the risk of hepatocellular carcinoma or the durability of functional cure once achieved HBsAg loss [22, 23]. In contrast, other studies also confirmed that anti-HBs seroconversion might impact the durability of NA- or PEG-IFN-induced HBsAg loss [24,25,26]. Therefore, large-scale prospective data were needed to unveil the role of anti-HBs seroconversion in long-term health consequences.
To the best of our knowledge, this study is the first to show the association between hepatitis B surface antibodies and mortality in a representative prospective cohort of a resolved HBV infection population. The effect of anti-HBs on mortality among resolved HBV infections in our study appears to be consistent with the results in the general and renal dialysis populations after vaccination [9, 27]. Previous studies have confirmed that intact immune responses are needed for the anti-HBs response to hepatitis B vaccination, and this response could be influenced by individual inflammation or health status. Therefore, the anti-HBs response could be an additional independent predictor of mortality [27]. In our study, compared with individuals who were anti-HBs positive, individuals who were anti-HBs negative had worse baseline health status. The protective effect on all-cause and cancer-related mortality may also reflect the overall health status of the participants. However, some protective effects remained in the fully adjusted model or after PSM, suggesting that these factors could not fully explain the impact of anti-HBs in reducing mortality.
The associations between anti-HBs and mortality among resolved HBV infections might be explained by the following reasons. First, in some cases, HBV cannot be eradicated because of the persistence of cccDNA and HBV DNA integration; HBV reactivation can occur spontaneously or upon immunosuppression [28]. The reactivation of HBV can accelerate the death of patients in the setting of immunocompromised conditions or in those who suffer from serious diseases [29,30,31]. The ability of anti-HBs to inhibit the reactivation of the hepatitis B virus thus partly leads to a reduction in mortality. The role of anti-HBs in inhibiting the reactivation of the hepatitis B virus may further reduce mortality, partially explaining our findings. Secondly, in acute hepatitis B, anti-HBs usually appear a few weeks after HBsAg seroclearance (in CHB, it may take much longer); anti-HBs can prevent viral spread from cells that remain infected after hepatitis resolution [23]. This notion is supported by the evidence that chimpanzees with resolving hepatitis B are protected from viral rechallenge [32]. In addition, our study indicated that participants who were anti-HBs negative had a higher percentage of HCV RNA positivity and higher FIB-4 scores than patients who were anti-HBs positive at baseline. FIB-4 scores can be used to assess the severity of liver fibrosis and correlate with disease outcomes [14]. Isolated anti-HBc has also been reported to be associated with coinfection with HCV, HIV, and occult HBV infection in previous studies [3, 33, 34]. Those factors may also be associated with increased all-cause mortality in participants who are anti-HBs negative (Fig. 6).

Potential theoretical link between hepatitis B surface antibody and risk of mortality
Although HBsAg loss is currently considered the optimal therapeutic endpoint of hepatitis B infection, the role of anti-HBs in resolved HBV infection should not be ignored. Anti-HBs seroconversion may offer some potential benefits for patients with resolved HBV infection. Thus, our results support that more rigorous surveillance is needed for isolated anti-HBc-positive populations. Additionally, hepatitis B vaccination and screening for occult hepatitis B might be required for this group.
Strengths and Limitations of this Study
The advantages of this study lie in its large sample size, national representativeness, high follow-up rate, and long-term mortality. Moreover, various potential confounding factors, including socioeconomic and health status, were adjusted or balanced to guarantee reliable results. In addition, our data are more representative and extensive because the population-based data used here represented a more comprehensive range of patients and could be more applicable to routine clinical practice. However, in regular randomized controlled trials, patients with multiple comorbidities or who are at high risk of HBV reactivation are often excluded.
This study has several limitations. First, this study lacks data on HBV regular monitoring, and occult HBV (liver and serum HBV DNA) has not been assessed in this study. However, occult HBV infection among individuals with resolved HBV infections is extremely low (the median prevalence was 1% as reported) [35, 36], and isolated anti-HBc positive populations were reported to be associated with occult HBV infection [33, 34], which further supports our conclusion that people who are anti-HBs negative and have resolved HBV infections seem to need more surveillance. Second, only qualitative results of anti-HBs were obtained, and the results were not continuously measured. The proportion of patients with positive anti-HBs may increase or decrease over time after HBsAg loss [3, 19, 24], which might lead to the misclassification of the individuals in the anti-HBs group. In addition, some study data, such as HCC and liver-related mortality, were missing. However, recent findings supported that HBV might be involved in general cancer development (not merely hepatocellular but also nonhepatocellular cancers) [37], and our data supported that anti-HBs might generate some beneficial effects on cancer development. Last, the theoretical link between anti-HBs negativity and overall mortality remains quite poor. Further studies are needed to monitor anti-HBs-related outcomes and reveal the underlying mechanism. Long-term studies are still needed for anti-HBs-related outcomes in individuals who are chronic carriers of HBsAg who achieved HBsAg loss in highly endemic settings.
Conclusions
Age, race, marital status, smoking status, physical activity level, cirrhosis, diabetes, cardiovascular diseases, chronic obstructive pulmonary diseases, cancer, and anti-HBs were all significant factors for increased mortality among individuals with resolved HBV infections, which may be a helpful reference for surveillance-related decision-making. Anti-HBs-negative status was associated with an increased risk of all-cause and cancer-related mortality among US adults with resolved HBV infections. This indicated that the role of anti-HBs in resolved HBV infection should not be ignored as a part of humoral immunity. Therefore, more rigorous surveillance is needed for populations of individuals who are isolated anti-HBc positive. Further studies are needed to monitor anti-HBs-related outcomes and reveal the underlying mechanism. Clinical trials on the long-term health consequences of HBsAg loss in highly endemic settings are also warranted.
References
European Association for the Study of the Liver. EASL 2017 Clinical Practice Guidelines on the management of hepatitis B virus infection. J Hepatol. 2017;2017(67):370–98.
Sarin SK, Kumar M, Lau GK, et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 update. Hepatol Int. 2016;10(1):1–98.
Terrault NA, Lok ASF, McMahon BJ, et al. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology. 2018;67:1560–99.
Huang SW, Chen C, Kong HY, et al. Prevalence of cirrhosis/advanced fibrosis among HBsAg-negative and HBcAb-positive US adults: a nationwide population-based study. Infect Dis Ther. 2022;11:1901–16.
Tong MJ, Nguyen MO, Tong LT, et al. Development of hepatocellular carcinoma after seroclearance of hepatitis B surface antigen. Clin Gastroenterol Hepatol. 2009;7(8):889–93.
Simonetti J, Bulkow L, McMahon BJ, et al. Clearance of hepatitis B surface antigen and risk of hepatocellular carcinoma in a cohort chronically infected with hepatitis B virus. Hepatology. 2010;51(5):1531–7.
Jinjuvadia R, Liangpunsakul S, Antaki F. Past exposure to hepatitis B: a risk factor for increase in mortality? J Clin Gastroenterol. 2014;48(3):267–71.
Brunskole Hummel I, Zitzmann A, Erl M, et al. Characteristics of immune memory 10–15 years after primary hepatitis B vaccination. Vaccine. 2016;34(5):636–42.
He WQ, Guo GN, Li C. The impact of hepatitis B vaccination in the United States, 1999–2018. Hepatology. 2022;75(6):1566–78.
Cornberg M, Lok ASF, Terrault NA, et al. Guidance for design and endpoints of clinical trials in chronic hepatitis B—report from the 2019 EASL-AASLD HBV treatment endpoints conferences. J Hepatol. 2020;72:539–57.
Centers for Disease Control and Prevention. About the National Health and Nutrition Examination Survey. https://www.cdc.gov/nchs/nhanes/about_nhanes.htm. Accessed Oct 2022.
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. https://wwwn.cdc.gov/nchs/nhanes/default.aspx. Accessed Oct 2022.
Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320:2020–8.
National Cancer Institute. Developing the Healthy Eating Index. https://epi.grants.cancer.gov/hei/developing.html#f1b. Accessed Oct 2022.
Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38:518–26.
Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis patients with HIV/HCV co-infection. Hepatology. 2006;43:1317–25.
National Center for Health Statistics. 2019 Public-Use Linked Mortality Files. https://www.cdc.gov/nchs/data-linkage/mortality-public.htm#. Accessed Oct 2022.
Yang H, Bae SH, Nam H, et al. A risk prediction model for hepatocellular carcinoma after hepatitis B surface antigen seroclearance. J Hepatol. 2022;77(3):632–41.
Kim GA, Lim YS, An J, et al. HBsAg seroclearance after nucleoside analogue therapy in patients with chronic hepatitis B: clinical outcomes and durability. Gut. 2014;63:1325–32.
Song AX, Wang XX, Lu JF, et al. Durability of hepatitis B surface antigen seroclearance and subsequent risk for hepatocellular carcinoma: a meta-analysis. J Viral Hepatitis. 2021;28:601–12.
Liu J, Yang HI, Lee MH, et al. Spontaneous seroclearance of hepatitis B seromarkers and subsequent risk of hepatocellular carcinoma. Gut. 2014;63:1648–57.
Yuen MF, Wong DKH, Fung J, et al. HBsAg seroclearance in chronic hepatitis B in Asian patients: replicative level and risk of hepatocellular carcinoma. Gastroenterology. 2008;135:1192–9.
Yip TC, Wong GL, Wong VW. Durability of hepatitis B surface antigen seroclearance in untreated and nucleos(t)ide analogue-treated patients. J Hepatol. 2017;S0168–8278(17):32332–42.
Wu YL, Liu YL, Lu JF, et al. Durability of interferon-induced hepatitis B surface antigen seroclearance. Clin Gastroenterol Hepatol. 2020;18:514.
Huang D, Wu D, Wang P, et al. End-of-treatment HBcrAg and HBsAb levels identify durable functional cure after Peg-IFN-based therapy in patients with CHB. J Hepatol. 2022;S0168–8278(22):00066–76.
Xu H, Locarnini S, Wong D, et al. Role of anti-HBs in functional cure of HBeAg+ chronic hepatitis B patients infected with HBV genotype A. J Hepatol. 2022;76:34–45.
Zitt E, Hafner-Giessauf H, Wimmer B, et al. Response to active hepatitis B vaccination and mortality in incident dialysis patients. Vaccine. 2017;35(5):814–20.
Shi Y, Zheng M. Hepatitis B virus persistence and reactivation. BMJ. 2020;370: m2200.
Paul S, Dickstein A, Saxena A, et al. Role of surface antibody in hepatitis B reactivation in patients with resolved infection and hematologic malignancy: a meta-analysis. Hepatology. 2017;66:379–88.
Jun CH, Kim BS, Oak CY, et al. HBV reactivation risk factors in patients with chronic HBV infection with low replicative state and resolved HBV infection undergoing hematopoietic stem cell transplantation in Korea. Hepatol Int. 2017;11(1):87–95.
Nishida T, Matsubara T, Yakushijin T, et al. Prediction and clinical implications of HBV reactivation in lymphoma patients with resolved HBV infection: focus on anti-HBs and anti-HBc antibody titers. Hepatol Int. 2019;13(4):407–15.
Moss B, Smith GL, Gerin JL, et al. Live recombinant vaccinia virus protects chimpanzees against hepatitis B. Nature. 1984;311:67–9.
Moretto F, Catherine FX, Esteve C, et al. Isolated anti-HBc: significance and management. J Clin Med. 2020;9:202.
Wu T, Kwok RM, Tran TT. Isolated anti-HBc: the relevance of hepatitis B core antibody—a review of new issues. Am J Gastroenterol. 2017;112(12):1780–8.
Raimondo G, Locarnini S, Pollicino T, et al. Update of the statements on biology and clinical impact of occult hepatitis B virus infection. J Hepatol. 2019;71:397–408.
Mak LY, Wong DK, Pollicino T, et al. Occult hepatitis B infection and hepatocellular carcinoma: epidemiology, virology, hepatocarcinogenesis and clinical significance. J Hepatol. 2020;73(4):952–64.
Song C, Lv J, Liu Y, et al. Associations between hepatitis B virus infection and risk of all cancer types. JAMA Netw Open. 2019;2(6):e195718.
Acknowledgements
We would like to thank all NHANES participants. The authors also thank Huang Da (Tongji Hospital) and Kong Hong-Yan (Tongji Hospital) for their help in the writing of the article.
Funding
This research received no specific grant from any public, commercial or not-for-profit funding agency. No funding or sponsorship was received for the publication of this article. The Rapid Service Fee was funded by the authors.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Contributions
Study concept and design: Shuai-Wen Huang, Qin Ning, Chen Chen, and Xi-Tang Li; Acquisition of data: Shuai-Wen Huang, Chen Chen, Xi-Tang Li, Qin Ning, and Jia-Quan Huang; Analysis and interpretation of data: Shuai-Wen Huang, Xi-Tang Li, Chen Chen, and Jia-Quan Huang; Drafting of the manuscript: Shuai-Wen Huang, Xi-Tang Li, Jia-Quan Huang, Qin Ning, and Chen Chen; Study supervision: Qin Ning, and Jia-Quan Huang.
Disclosures
Shuai-Wen Huang, Xi-Tang Li, Chen Chen, Qin Ning and Jia-Quan Huang all declare that there is no conflict of interest regarding the publication of this article.
Compliance with Ethics Guidelines
The study was conducted according to the principles of the Helsinki Declaration. The approval of the study from the NCHS ethics review board was waived because the research relied on publicly available, deidentified secondary data. All participants signed informed consent forms.
Data Availability
The data sets used and analyzed during the current study are available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Huang, SW., Li, XT., Chen, C. et al. Effect of Anti-HBs on Mortality Among Resolved HBV Infection: a Population-Based Prospective Cohort Study. Infect Dis Ther 12, 871–890 (2023). https://doi.org/10.1007/s40121-023-00766-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40121-023-00766-5