
Abstract
Introduction
Atopic dermatitis (AD) is a chronic disease that occurs mainly in children. Topical corticosteroids are the main treatment for mild to moderate AD, although they can induce side effects. The efficacy and tolerability of xyloglucan and pea protein (XG-PP) was compared with hydrocortisone in pediatric patients with AD as a steroid-sparing solution.
Methods
A prospective, multicenter, comparative study enrolled 42 patients (age 0.5–12 years) with mild-to-moderate AD, assigned 1:1 to XG-PP or hydrocortisone ointment. Treatments were applied twice daily for 14 consecutive days and assessed at baseline, day 8, and day 15. Efficacy endpoints were AD Severity Index (ADSI) score, Scoring Atopic Dermatitis (SCORAD) index, and Patient-Oriented Eczema Measure (POEM). Tolerability was assessed by the occurrence of adverse events (AEs).
Results
Both treatments significantly improved ADSI mean score from baseline to day 15; in the XG-PP arm, ADSI score decreased from 10.55 to 4.15 (p = 0.00001), and in the hydrocortisone arm, from 10.65 to 4.30 (p = 0.0001). In the XG-PP arm, the mean SCORAD score decreased from 65.86 to 30.26 (p = 0.00001) and in the hydrocortisone arm from 68.84 to 31.19 (p = 0.0001) at day 15. An overall decrease from moderate to mild AD for both arms (p = 0.0001) was observed with POEM. For all the three indexes evaluated, no statistical significant differences between the study arms evolution from baseline to day 8 or to day 15 were found. No AEs were reported.
Conclusion
XG-PP provided a comparable efficacy to hydrocortisone ointment in managing AD, thus representing a safe and effective steroid-sparing alternative in pediatric patients with AD.
Trial Registration
Retrospectively registered on 24 November 2021 in the ISRCTN registry: 11118799.
Similar content being viewed by others


Why carry out this study? |
Atopic dermatitis (AD) affects between 10% and 20% of the pediatric population worldwide and has increased in developed and low-income countries in recent decades. Topical corticosteroids (TCS) are the mainstay to control skin inflammation and flare-ups in pediatric populations in the short term. |
Although TCS have a good safety profile, adverse effects are possible, and the skepticism of patients and parents toward TCS often leads to non-compliance to treatment, which may result in unsatisfactory outcomes. |
On the basis of the efficacy and tolerability of xyloglucan (XG) and pea protein (PP) in adult patients with AD, we expect to observe high tolerability and amelioration of signs and symptoms of AD in infants and children following a 14-day topical treatment with XG and PP. |
What was learned from the study? |
Topical treatment with XG and PP provides rapid symptom improvement in pediatric patients affected by mild and moderate AD with an efficacy similar to topical hydrocortisone. |
This study confirms that the topical combination of XG and PP also evokes benefits in pediatric patients with mild to moderate AD. |
The study shows that the novel natural-based cream containing XG and PP represents a possible alternative therapy for the treatment of AD in children. |
Introduction
Atopic dermatitis (AD) is a common chronic inflammatory skin disease that usually affects the face, scalp, trunk, flexural surfaces, and hands. The severity of the disease can range from mild to severe disease that is difficult to control [1, 2]. AD is characterized by dryness and lichenification and is often accompanied by a combination of pruritic erythema, excoriations, and serous exudate [3,4,5]. AD affects between 10% and 20% [6] of the pediatric population worldwide and has increased in developed countries in recent decades. Fifty to 60% of patients diagnosed with AD experience symptoms before the age of 1 year [3, 6, 7]. Numerous studies have shown that skin barrier dysfunction and immune system dysregulation play key roles in AD development. Skin barrier dysfunction has been linked to several gene mutations among which the most notable is the filaggrin (FLG) gene, which encodes the filaggrin protein, a key player in stratum corneum development and structure [8, 9].
Since AD is a chronic condition, the main goal of treatment is to reduce the number of exacerbations of the disease and to limit their severity and duration [10]. Basic therapy focuses on restoring skin barrier function by hydrating the skin with emollients or moisturizers. Topical treatments containing naturally derived non-pharmacological substances have gained much attention in the last few years. These topical solutions act through several synergistic mechanisms of action to preserve the lipid content of the skin barrier, preventing transepidermal water loss (TEWL), and thus moisturizing the skin. These solutions reduce inflammation and itch to improve atopic lesions. These types of moisturizers could be effective not only as maintenance therapy for AD but also when used synergistically with anti-inflammatory pharmacological therapies to prevent flare-ups [11, 12]. Topical corticosteroids (TCS) are the mainstay to control skin inflammation and flare-ups in pediatric populations in the short term. Topical treatments based on calcineurin inhibitors are also used for long-term management of disease flare-ups.
Although TCS have a good safety profile, adverse effects are possible, such as cutaneous atrophy, striae, purpura, telangiectasia, acne-like eruption, and systemic absorption with resulting adrenal suppression [13, 14]. The skepticism of patients and parents toward TCS often leads to non-compliance to treatment, which may result in unsatisfactory outcomes [15,16,17]. Plant-based products have been studied for a long time as an alternative and complementary strategy for the treatment of skin diseases, including AD [18]. Xyloglucan (XG) and pea protein (PP), in addition to emollients and skin conditioners, are the main components of a product manufactured by Devintec SAGL for the treatment of AD in children. XG and PP are substances of natural origin: XG is a non-ionic, neutral, branched polysaccharide consisting of a cellulose-like backbone derived from tamarind seeds [19]. XG is a US Food and Drug Administration (FDA)-approved food additive, a stabilizing agent, and a pharmaceutical excipient. Known for its wound-healing properties, XG can be used as a mucosae and tissue protectant, with restorative functions [20]. PPs are hypoallergenic proteins derived from peas [21], they are particularly rich in glutamine, aspartic acid, arginine, and lysine [22], and have been studied for their ability to help attenuate inflammatory symptoms and microbial colonization [23]. By synergistically creating a protective barrier over the skin, XG and PP have the ability to protect the tissue from external insults, by avoiding the adhesion and proliferation of bacteria, while promoting the natural recovery of the damaged skin barrier. Preclinical AD models demonstrated the ability of XG and PP to preserve epidermal integrity, reduce mast cell degranulation and type 2 interleukins, and support FLG recovery with comparable efficacy to hydrocortisone, suggesting that XG-PP-based products could be a promising approach for the treatment of this condition [24, 25]. Moreover, a double-blind, parallel, randomized, placebo-controlled clinical trial showed that a XG-PP-based formulation significantly improves AD severity even in an adult population, after only 8 days of treatment, representing an alternative solution for mild to moderate AD in adult patients [26].
The aim of the study was to evaluate, in infants and children with AD, the efficacy and tolerability of XG-PP-based topical treatment compared to hydrocortisone, commonly prescribed in the pediatric population.
Methods
Study Design
The present study is a prospective, multicenter, comparative clinical trial sponsored by Novintethical Pharma SA. The study was carried out between August 2019 and April 2020 in five medical centers in Romania, where a hydrocortisone ointment (10 mg/g) is the standard of care for the treatment of AD. Topical corticosteroids are recommended for AD-affected patients who have failed to respond to good skin care and regular use of emollients. The study was performed following the Declaration of Helsinki in accordance with the guideline on Good Clinical Practice (GCP) of the European Community. The study protocol (DERCBS18-06) received full regulatory approval from Romanian National Committee of Bioethics for Medicine and Medical Devices and has been registered in the ISRCTN registry (TN11118799).
Inclusion and Exclusion Criteria
Pediatric patients between 6 months and 12 years old with confirmed diagnosis of AD were considered eligible for the study. Patients were excluded from the study if they presented illness within 4 days before study enrollment or any medical condition that may affect study participation, if they had diagnosis or history of other dermatological conditions, if they had previous allergic reactions or known sensitivity to one or more of the study ingredients, or if they used medications that could affect the study or products that could have an effect similar to the product studied (e.g., corticosteroids, anti-inflammatory drugs). Parents or legal guardians signed a written informed consent prior to treatment.
Treatments
Patients were enrolled in the treatment study in a 1:1 ratio of XG-PP-based cream or hydrocortisone (10 mg/g ointment) with a regimen of two applications/day for 14 consecutive days. It was decided to use hydrocortisone—a low potency topical steroid normally used as standard of care in this category of patients and approved by the ethical committee—for the safety of the children in the study (i.e., to avoid potential complications of high potency topical steroids).
Patients performed three clinical visits: at day 0 (baseline), at day 8 (after 7 days of treatment), at day 15 (end of treatment).
Study Objectives and Endpoints
The primary objective of this study was the evaluation of the efficacy of the product containing XG-PP in alleviating the signs of AD. The primary endpoints were the change from baseline in AD Severity Index (ADSI) [27], a 4-point scale from none (0) to severe (3) for erythema, pruritus, exudation, excoriation, crusts, erosions, and lichenification; the change from baseline in the Scoring Atopic Dermatitis (SCORAD) index [28], calculated according to signs scored by the investigators; and the change from baseline in the Patient-Oriented Eczema Measure (POEM) 5-point scale [29]. All endpoints were evaluated at day 0, day 8, and day 15. ADSI score results can range between minimum 0 and maximum 15; the latter was considered the highest severity in AD evaluation. The SCORAD index assesses the extent (0–100), intensity (0–18), and subjective symptoms (0–20) in patients with AD. The intensity consists of six items: erythema, edema and papules, excoriations, lichenification, vesicles and crusts, and dryness. The subjective items included daily pruritus and sleeplessness. Both subjective items were scored on a 100-mm visual analogue scale where zero corresponds to not at all and 100 to the worst condition. The POEM assesses AD severity according to the following categories: POEM score 0–2, clear or almost clear; score 3–7, mild eczema; score 8–16, moderate eczema; score 17–24, severe eczema; score 25–28, very severe eczema.
The secondary objective was to assess the tolerability of the product studied by monitoring the occurrence of adverse events (AEs), defined as any unwarranted medical occurrence in a patient (any adverse event whether device related or not). The following parameters were evaluated: percentage of participants who experienced AEs, number of patients who discontinued the study as a result of AEs, and AD progression.
Statistical Analysis
Assuming a mean difference of 10 in the change in SCORAD index from baseline to day 15 based on previous studies and expert agreement, a standard deviation of 11, a significance level (α) of 0.05, a power of 80%, and a dropout rate of 10%, we calculated a sample size of 21 patients in each group [30]. Continuous data were expressed in terms of mean, standard deviation (SD), and number of observations. Categorical data were summarized in terms of the number of patients and percentages. To evaluate statistically significant differences in the demographic characteristics at baseline between the two study groups, t test or chi-square test was used. To examine the primary outcome, the t test and Wilcoxon signed-rank test were applied to compare the mean scores of ASDI scale, SCORAD index, and POEM scale in the two treatment groups. A p value less than 0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics 20.
Results
Population Characteristics
A total of 42 patients were enrolled in the study, 21 patients in each treatment group. There were 11 and 8 male patients in the XG-PP-based product and hydrocortisone groups, respectively (p = 0.53). The mean age of patients was 4 years (range 1–11) in the study product group and 7 years (range 1–12) in the hydrocortisone group (p = 0.18). The study groups showed similar results and no statistical differences at baseline were observed (Table 1).
Primary Endpoints
The primary endpoints of the study were the change in mean ADSI score, SCORAD index, and POEM score in both treatment arms from baseline to days 8 and 15. Both arms showed clinically significant improvement in ADSI score at day 8 and day 15. In the XG-PP treatment group, ADSI score decreased from a mean of 10.55 at baseline to 6.25 at day 8 (p = 0.00001), and 4.15 at day 15 (p = 0.00001). In the hydrocortisone group, the ADSI mean score decreased from 10.65 at baseline to 6.85 at day 8 (p = 0.00001), and to 4.30 at day 15 (p = 0.00001). No statistically significant differences were found between the study arms when comparing the decrease from baseline to day 8 (p = 0.91) or to day 15 (p = 0.92) (Fig. 1a).

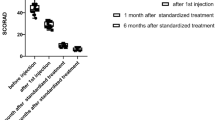
a ADSI mean score results at the time-point evaluations. No statistically significant differences were found between the study arms when comparing the decrease from baseline to day 8 (p = 0.91) or to day 15 (p = 0.92). Statistically significant differences were found in the study arm compared to day 0 with p = 0.00001 at day 8 and at day 15 in both the XG-PP and hydrocortisone treatment groups (*). b SCORAD mean score results at the time-point evaluations. No statistically significant differences were observed between study arms when comparing the decrease in SCORAD index from baseline to day 8 (p = 0.88) or to day 15 (p = 0.93). Statistically significant differences were found in the study arm compared to day 0: p = 0.00001 at day 8 and at day 15 in the XG-PP treatment arm; p = 0.0002 at day 8 and p = 0.00001 at day 15 in the hydrocortisone treatment group (*). c Score results at the time-point evaluations. No statistically significant differences were found between study arms when comparing score decrease from baseline to day 8 (p = 0.89) or from baseline to day 15 (p = 0.75). Statistically significant differences were found in the study arm compared to day 0 with a value of p = 0.00001 at day 8 and at day 15 in both the XG-PP and hydrocortisone treatment groups (*)
Analysis of the SCORAD index showed a significant improvement in mean scores for both arms. In the XG-PP arm, the mean SCORAD score decreased significantly from baseline (65.86) to day 8 (53.21; p = 0.00001) and to day 15 (30.26; p = 0.00001). In the hydrocortisone arm, a statistically significant decrease in the mean SCORAD score was observed between baseline (68.84) and day 8 (53.55; p = 0.0002) and baseline and day 15 (31.19; p = 0.00001). No statistically significant differences were observed between study arms when comparing the decrease in SCORAD index from baseline to day 8 (p = 0.88) or to day 15 (p = 0.93) (Fig. 1b). Assessment of the POEM score showed improvement in the group of patients treated with the XG-PP-based product. The mean score of 15.15 at baseline, indicating moderate eczema, decreased to 10.50 (p = 0.00001) at day 8 and to 6.85 at day 15 (p = 0.00001), indicating mild eczema. In the hydrocortisone group, the POEM mean score at baseline was 15.60, indicating moderate eczema, which improved to 10.65 and to 6.50 on day 15, indicating mild eczema; comparison between baseline and day 8 or day 15 showed a statistically significant difference in patient evolution (p = 0.00001). No statistically significant differences were found between study arms when comparing score decrease from baseline to day 8 (p = 0.89) or from baseline to day 15 (p = 0.75) (Fig. 1c).
Secondary Endpoints
Evaluation of the secondary endpoints showed that there was no AE or AD progression on day 8, 15, and 28 of treatment with XG-PP.
Discussion
This study confirms the beneficial effects of the novel topical treatment containing XG-PP in relieving symptoms associated with AD in pediatric patients, with a comparable efficacy to that of hydrocortisone, confirming the initial assumption that XG and PP are effective to protect the tissue from external insults by synergistically creating a protective barrier over the skin [31]. Improvements assessed by the primary endpoints demonstrated a rapid and continuous effect of the product. Indeed, ADSI, SCORAD, and POEM mean scores showed a statistically significant decrease from baseline to day 8 of the assessment and another significant decrease on day 15. In addition, patients enrolled had moderate AD at baseline, as indicated by the POEM score, and 2 weeks of treatment with XG and PP reduced the mean AD grade of the study cohorts to “mild,” indicating that pediatric patients with moderate AD are the potential target population for XG and PP cream. In particular, POEM is well recognized to be a feasible tool also for clinical practice [1, 7, 32]. Tolerability analysis confirmed the good safety profile of the study product as no AEs nor dropouts were reported.
Several clinical trials comparing the efficacy of TCS with emollients are available, but they are mostly characterized by inconsistent study design [33, 34]. A recently published meta-analysis of AD pediatric studies found that treatments with TCS tended to be more effective than vehicles or moisturizers, but generalization is not possible because of the wide heterogeneity of products with different moisturizing properties [33]. Interestingly, several studies have shown that the co-administration of TCS and emollients or moisturizers improves symptoms associated with AD [35, 36]. In this regard, a new generation of emollients containing active non-pharmacological ingredients has gained attention for their corticosteroid-sparing effect when used as an alternative to TCS [11]. A multicenter, open-label trial using an oat-based emollient in the maintenance therapy of 108 children (ages 6 months–6 years) with moderate AD demonstrated that the number of flares and use of TCS significantly decreased during 3 months of treatment [37]. Additionally, in subjects above 3 years of age with mild and stable AD, the treatment containing vitamin E, tocopherol, glycerine, and enriched with Aqua posae filiformis and microresyl significantly reduces AD clinical signs and symptoms and increases skin hydration after 28 days, thus improving the patients’ quality of life [38].
The results of this study show that the novel natural-based cream containing XG and PP represents a possible substitute therapy for the treatment of AD in children taking TCS. Notably, XG and PP can significantly reduce AD-associated symptoms within a week of treatment which may avoid short- and long-term AEs caused by TCS and improve treatment adherence [39,40,41,42].
Importantly, this is the first clinical study to verify the efficacy and safety of a topical formulation containing XG and PP in children, confirming the results observed in preclinical studies [25]. Additionally, oral utilization of XG and PP in adults demonstrated no systemic adverse events during 6 months of treatment [43, 44]. To date, the literature revealed that phytotherapeutic treatments for AD and products of natural origin are often considered adjunctive therapies for the treatment of moderate to severe AD [18, 45]. Clinical trials assessing the efficacy and safety of topical phytotherapy for AD treatment are limited. In one randomized controlled study, 55% of subjects treated with aloe vera reported drying up of the skin on test areas while no serious adverse effects were recorded [46]. More recent data showed that aloe vera [47] or Cardiospermum halicacabum [48] based creams exhibit a good efficacy profile. On the other hand, other studies indicated that a prolonged use of topical aloe vera-based products could lead to unwanted side effects such as urticaria [49], contact dermatitis [50,51,52], and widespread dermatitis [53].
The reported results are significant because the treatment studied was shown to be as effective and safe as the standard short-term steroid-sparing therapy for pediatric patients with mild to moderate AD. The reported results of XG and PP also suggest that this novel therapeutic could act as an effective and safe alternative maintenance treatment after the patient has undergone reactive therapy with topical corticosteroids.
The importance of a fast-acting product with the ability to decrease symptom severity within 1 week greatly impacts the daily lives of patients and their families which leads to an improved AD management [54]. Controlled clinical trials are advisable to explore the possibility that such treatment may reduce the severity of AD over time, thereby reducing the burden of disease on the patients and caregivers. In addition, the inclusion of a quality of life tool in the study endpoints would be useful to assess the impact of the treatment on everyday life; the same applies to objective measures such as self-report questionnaires that can provide information about patients’ feelings regarding product tolerability.
There are a few limitations to the study. First, the number of participants included into the study is limited. Further studies should be based on larger groups of patients. Moreover, patients were screened and enrolled by dermatologists at their individual offices and/or medical centers. The doctors had to confirm a diagnosis of AD through a clinical evaluation based on their experience in order to enroll a patient. However, a more stringent selection process would be beneficial. Secondly, it was not possible to collect some information such as the date of eczema onset, comorbidities, and the percentage of participants previously treated with systemic agents and/or topical corticosteroids. Lastly, the follow-up period was 2 weeks. Given the promising safety and efficacy results obtained, longer follow-up studies, including other scores such as EASI, VAS pruritus, and IGA, are needed to demonstrate the efficacy in preventing flare-ups and the establishment of long-term disease control.
Conclusion
Topical treatment with XG and PP provides rapid and durable benefits in pediatric patients affected by mild and moderate AD. The efficacy of this treatment is comparable to mild-potency topical corticosteroid therapy. Use of XG-PP can therefore be considered as a steroid-sparing strategy. XG-PP is also characterized by an excellent tolerability, embodying a potential maintenance treatment. Future research in children should extend studies on the fast action of the treatment to improve quality of life and the ability to reduce flare-ups for long-term AD management.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Boguniewicz M, Fonacier L, Guttman-Yassky E, Ong PY, Silverberg J, Farrar JR. Atopic dermatitis yardstick: practical recommendations for an evolving therapeutic landscape. Ann Allergy Asthma Immunol. 2018;120:10–22.e2.
Schneider L, Tilles S, Lio P, et al. Atopic dermatitis: a practice parameter update 2012. J Allergy Clin Immunol. 2013;131:227–95.
Gür Çetinkaya P, Şahiner ÜM. Childhood atopic dermatitis: current developments, treatment approaches, and future expectations. Turk J Med Sci. 2019;49:963–84.
Chu CY. Treatments for childhood atopic dermatitis: an update on emerging therapies. Clin Rev Allergy Immunol. 2021;61:114–27.
Zaniboni MC, Samorano LP, Orfali RL, Aoki V. Skin barrier in atopic dermatitis: beyond filaggrin. An Bras Dermatol. 2016;91:472–8.
Kowalska-Olędzka E, Czarnecka M, Baran A. Epidemiology of atopic dermatitis in Europe. J Drug Assess. 2019;8:126–8.
Fishbein AB, Silverberg JI, Wilson EJ, Ong PY. Update on atopic dermatitis: diagnosis, severity assessment, and treatment selection. J Allergy Clin Immunol Pract. 2020;8:91–101.
Lyons JJ, Milner JD, Stone KD. Atopic dermatitis in children: clinical features, pathophysiology, and treatment. Immunol Allergy Clin North Am. 2015;35:161–83.
Kim BE, Leung DYM. Significance of skin barrier dysfunction in atopic dermatitis. Allergy Asthma Immunol Res. 2018;10:207–15.
Thomsen SF. Atopic dermatitis: natural history, diagnosis, and treatment. ISRN allergy. 2014;2014:354250.
Araviiskaia E, Pincelli C, Sparavigna A, Luger T. The role of a novel generation of emollients, “emollients plus”, in atopic dermatitis. Clin Cosmet Investig Dermatol. 2022;15:2705–19.
Wollenberg A, Kinberger M, Arents B, et al. European guideline (EuroGuiDerm) on atopic eczema—part II: non-systemic treatments and treatment recommendations for special AE patient populations. J Eur Acad Dermatol Venereol. 2022;36:1904–26.
Abraham A, Roga G. Topical steroid-damaged skin. Indian J Dermatol. 2014;59:456–9.
Drake LA, Dinehart SM, Farmer ER, et al. Guidelines of care for the use of topical glucocorticosteroids. J Am Acad Dermatol. 1996;35:615–9.
Fischer G. Compliance problems in paediatric atopic eczema. Australas J Dermatol. 1996;37(Suppl 1):S10–3.
Smith SD, Hong E, Fearns S, Blaszczynski A, Fischer G. Corticosteroid phobia and other confounders in the treatment of childhood atopic dermatitis explored using parent focus groups. Australas J Dermatol. 2010;51:168–74.
Charman CR, Morris AD, Williams HC. Topical corticosteroid phobia in patients with atopic eczema. Br J Dermatol. 2000;142:931–6.
Hussain Z, Thu HE, Shuid AN, Kesharwani P, Khan S, Hussain F. Phytotherapeutic potential of natural herbal medicines for the treatment of mild-to-severe atopic dermatitis: a review of human clinical studies. Biomed Pharmacother. 2017;93:596–608.
Gnessi L, Bacarea V, Marusteri M, Piqué N. Xyloglucan for the treatment of acute diarrhea: results of a randomized, controlled, open-label, parallel group, multicentre, national clinical trial. BMC Gastroenterol. 2015;15:153.
Ajovalasit A, Redondo-Gómez C, Sabatino MA, et al. Carboxylated-xyloglucan and peptide amphiphile co-assembly in wound healing. Regen Biomater. 2021;8: rbab040.
Mathai JK, Liu Y, Stein HH. Values for digestible indispensable amino acid scores (DIAAS) for some dairy and plant proteins may better describe protein quality than values calculated using the concept for protein digestibility-corrected amino acid scores (PDCAAS). Br J Nutr. 2017;117:490–9.
Dahl WJ, Foster LM, Tyler RT. Review of the health benefits of peas (Pisum sativum L.). Br J Nutr. 2012;108(Suppl 1):S3–10.
Ndiaye F, Vuong T, Duarte J, et al. Anti-oxidant, anti-inflammatory and immunomodulating properties of an enzymatic protein hydrolysate from yellow field pea seeds. Eur J Nutr. 2012;51:29–37.
Campolo M, Casili G, Paterniti I, et al. Effect of a product containing xyloglucan and pea protein on a murine model of atopic dermatitis. Int J Mol Sci. 2020;21:3596.
Campolo M, Lanza M, Filippone A, et al. Evaluation of a product containing xyloglucan and pea protein on skin barrier permeability. Skin Pharmacol Physiol. 2020;33:231–6.
Sowlati M, Orzan O-A, Morariu SH, Etropolska Z, Veraldi S, Dimitrov S. Topical application of a formulation containing pea proteins and xyloglucan in adult patients with atopic dermatitis: a double-blind, parallel, randomized, placebo-controlled, multicenter study. J Clin Aesthet Dermatol. 2023;16:35–41.
Silverberg JI, Tallman AM, Ports WC, Gerber RA, Tan H, Zielinski MA. Evaluating the efficacy of crisaborole using the atopic dermatitis severity index and percentage of affected body surface area. Acta Derm Venereol. 2020;100(13):adv00170.
Kunz B, Oranje AP, Labrèze L, Stalder JF, Ring J, Taïeb A. Clinical validation and guidelines for the SCORAD index: consensus report of the European Task Force on Atopic Dermatitis. Dermatology. 1997;195:10–9.
Charman CR, Venn AJ, Williams HC. The Patient-Oriented Eczema Measure: development and initial validation of a new tool for measuring atopic eczema severity from the patients’ perspective. Arch Dermatol. 2004;140:1513–9.
Sakpal TV. Sample size estimation in clinical trial. Perspect Clin Res. 2010;1:67–9.
Piqué N, Gómez-Guillén MDC, Montero MP. Xyloglucan, a plant polymer with barrier protective properties over the mucous membranes: an overview. Int J Mol Sci. 2018;19:673.
Chopra R, Silverberg JI. Assessing the severity of atopic dermatitis in clinical trials and practice. Clin Dermatol. 2018;36:606–15.
Fishbein AB, Mueller K, Lor J, Smith P, Paller AS, Kaat A. Systematic review and meta-analysis comparing topical corticosteroids with vehicle/moisturizer in childhood atopic dermatitis. J Pediatr Nurs. 2019;47:36–43.
Nankervis H, Thomas KS, Delamere FM, Barbarot S, Rogers NK, Williams HC. Scoping systematic review of treatments for eczema. Southampton (UK): NIHR Journals Library; 2016.
Szczepanowska J, Reich A, Szepietowski JC. Emollients improve treatment results with topical corticosteroids in childhood atopic dermatitis: a randomized comparative study. Pediatr Allergy Immunol. 2008;19:614–8.
van Zuuren EJ, Fedorowicz Z, Christensen R, Lavrijsen A, Arents BWM. Emollients and moisturisers for eczema. Cochrane Database Syst Rev. 2017;2:CD012119.
Mengeaud V, Phulpin C, Bacquey A, Boralevi F, Schmitt AM, Taieb A. An innovative oat-based sterile emollient cream in the maintenance therapy of childhood atopic dermatitis. Pediatr Dermatol. 2015;32:208–15.
Cestari S, Correia P, Kerob D. Emollients, “plus” are beneficial in both the short and long term in mild atopic dermatitis. Clin Cosmet Investig Dermatol. 2023;16:2093–102.
Eichenfield LF, Totri C. Optimizing outcomes for paediatric atopic dermatitis. Br J Dermatol. 2014;170(Suppl):31–7.
Kojima R, Fujiwara T, Matsuda A, et al. Factors associated with steroid phobia in caregivers of children with atopic dermatitis. Pediatr Dermatol. 2013;30:29–35.
Bos B, Antonescu I, Osinga H, Veenje S, de Jong K, de Vries TW. Corticosteroid phobia (corticophobia) in parents of young children with atopic dermatitis and their health care providers. Pediatr Dermatol. 2019;36:100–4.
Bass AM, Anderson KL, Feldman SR. Interventions to increase treatment adherence in pediatric atopic dermatitis: a systematic review. J Clin Med. 2015;4:231–42.
Trifan A, Burta O, Tiuca N, Petrisor DC, Lenghel A, Santos J. Efficacy and safety of Gelsectan for diarrhoea-predominant irritable bowel syndrome: a randomised, crossover clinical trial. United Eur Gastroenterol J. 2019;7:1093–101.
Bellini M, Berti G, Bonfrate L, et al. Use of GELSECTAN® in patients with Irritable Bowel Syndrome (IBS): an Italian experience. Patient Prefer Adherence. 2021;15:1763–74.
Tumpang MA, Ramli NA, Hussain Z. Phytomedicines are efficient complementary therapies for the treatment of atopic dermatitis: a review of mechanistic insight and recent updates. Curr Drug Targets. 2018;19:674–700.
Paulsen E, Korsholm L, Brandrup F. A double-blind, placebo-controlled study of a commercial Aloe vera gel in the treatment of slight to moderate psoriasis vulgaris. J Eur Acad Dermatol Venereol. 2005;19:326–31.
Panahi Y, Rastgar N, Zamani A, Sahebkar A. Comparing the therapeutic effects of aloe vera and olive oil combination cream versus topical betamethasone for atopic dermatitis: a randomized double-blind clinical trial. J Pharmacopuncture. 2020;23:173–8.
Fai D, Fai C, Di Vito M, Martini C, Zilio G, De Togni H. Cardiospermum halicacabum in atopic dermatitis: clinical evidence based on phytotherapic approach. Dermatol Ther. 2020;33: e14519.
Morrow DM, Rapaport MJ, Strick RA. Hypersensitivity to aloe. Arch Dermatol. 1980;116:1064–5.
Shoji A. Contact dermatitis to Aloe arborescens. Contact Dermatitis. 1982;8:164–7.
Nakamura T, Kotajima S. Contact dermatitis from aloe arborescens. Contact Dermatitis. 1984;11:51.
Savchak VI. Ostryĭ bulleznyĭ allergichekiĭ dermatit ot mestnogo primenenniia list’ev aloé [Acute bullous allergic dermatitis due to local application of aloe leaves]. Vestn Dermatol Venerol. 1977;12:44–5.
Hogan DJ. Widespread dermatitis after topical treatment of chronic leg ulcers and stasis dermatitis. CMAJ. 1988;138:336–8.
Patel NU, D’Ambra V, Feldman SR. Increasing adherence with topical agents for atopic dermatitis. Am J Clin Dermatol. 2017;18:323–32.
Acknowledgements
We thank the participants of the study.
Medical Writing and Editorial Assistance
The authors didn’t receive any medical writing or editorial assistance for this article.
Funding
Sponsorship for this study was funded by Novintethical Pharma SA, and Rapid Service Fee was funded by Devintec SAGL.
Author information
Authors and Affiliations
Contributions
Roni P. Dodiuk-Gad contributed to results, discussion, reading and approval of the manuscript. Stefano Veraldi contributed to study conception and design, discussion of results, manuscript reading and approval (but did not participate in data collection and analysis). All other authors contributed to the study conception, design, data collection and analysis. All authors discussed the results, contributed to the final manuscript, read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of Interest
The authors have no conflict of interests to declare.
Ethical Approval
The study was performed following the Declaration of Helsinki in accordance with the guideline on Good Clinical Practice (GCP) of the European Community. The study protocol (DERCBS18-06) received full regulatory approval from Romanian National Committee of Bioethics for Medicine and Medical Devices and has been registered in the ISRCTN registry (TN11118799).
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sowlati, M., Morariu, SH., Orzan, O. et al. Efficacy and Tolerability of a Novel Topical Treatment Containing Pea Protein and Xyloglucan in the Management of Atopic Dermatitis in Children: A Prospective, Multicenter Clinical Study. Dermatol Ther (Heidelb) 13, 2669–2679 (2023). https://doi.org/10.1007/s13555-023-01035-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13555-023-01035-6