
Abstract
Introduction
The fixed-ratio combination of insulin glargine (iGlar) plus lixisenatide (iGlarLixi) has proven efficacious in clinical trials; however, there is limited evidence of its benefits in a variety of real-world patients with type 2 diabetes mellitus (T2DM) who present in routine clinical practice.
Methods
A large integrated claims and EHR database was used to identify two real-world (RW) cohorts (ages ≥ 18) with T2DM who were eligible for treatment with iGlarLixi. At baseline, the first cohort (insulin cohort) received insulin with or without oral antidiabetic drugs (OADs), and the second cohort (OAD-only cohort) received OADs only. A Monte Carlo patient-level simulation was applied to each cohort based on treatment strategies and efficacies from the LixiLan-L and LixiLan-O trials to estimate reductions in glycated hemoglobin A1C (A1C) and the percentage achieving age-based A1C goals (≤ 7% for ages < 65 and ≤ 8% for ages ≥ 65) at 30 weeks.
Results
The RW insulin (N = 3797) and OAD-only (N = 17,633) cohorts differed considerably in demographics, age, clinical characteristics, baseline A1C levels, and background OAD therapies compared to the populations in the Lixilan-L and Lixilan-O trials. Regardless of the cohort description, A1C goals were achieved among 52.6% vs. 31.6% (p < 0.001) of patients in the iGlarLixi vs. the iGlar arms in the insulin cohort simulation, while A1C goals were achieved among 59.9% vs. 49.3% and 32.8% (p < 0.001) of patients in the OAD-only cohort simulation in the iGlarLixi vs. the iGlar and lixisenatide arms, respectively.
Conclusions
Irrespective of the treatment regimen at baseline (insulin vs. OAD only), this patient-level simulation demonstrated that a greater proportion of patients achieved their A1C goals with iGlarlixi compared to iGlar or lixisenatide alone. These findings suggest that the benefits of iGlarLixi extend to clinically distinct RW populations.
Similar content being viewed by others


Nearly half of the patients with type 2 diabetes who receive routine antidiabetic therapy do not maintain an A1C value < 7.0%, and about 22% have an A1C value > 8.0%. |
Due to higher glycemic control and the simplified once-a-day regimen, the 2023 standards of care guidelines from the American Diabetes Association recommend the use of fixed-ratio combination therapy for patients with unmet A1C goals on GLP-1RA or GIP/GLP-1RA, as well as for patients on complex insulin regimens. |
iGlarLixi has proven to be efficacious compared to its mono-components in clinical trials. This study provides evidence of its benefits in diverse real-world populations with T2DM who present in routine clinical practice. |
Introduction
Diabetes is a lifelong chronic condition that is imposing a significant burden on patients and healthcare systems and affects more than 536 million people worldwide, a number which is expected to grow to 642 million by 2030 [1]. As per the 2022 National Diabetes Statistics Report, about 37.3 million people in the United States (US) have diabetes, accounting for $379 billion in health care costs [2], with the largest share (73%) attributable to direct medical treatment [3]. Type 2 diabetes mellitus (T2DM) accounts for more than 95% of all diabetes cases [4]. Among adults ≥ 65 years in the US, about 29.2% have the disease and 48.8% are believed to live with prediabetes [5].
Historically, metformin was prescribed as the first-line therapy for T2DM due to its high efficacy, low cost, weight neutrality, and few adverse events [6]; however, evidence points to the need for treatment intensification for patients with T2DM who fail to achieve their optimal glycemic targets [7, 8]. The 2023 standards of care in diabetes (SOC) guidelines from the American Diabetes Association (ADA) recommend treatments like sodium-glucose cotransporter 2 inhibitors (SGLT2) and/or glucagon-like peptide 1 receptor agonists (GLP-1 RA) or gastric inhibitory peptide (GIP)/GLP-1RA, based on existing comorbidities and other patient-centered treatment factors, as the first line of therapy. The ADA now also recommends GLP-1 RA or GIP/GLP-1RA as the first injectable for patients not meeting A1C targets and the addition of basal insulin as a free or a fixed-ratio combination for those unable to achieve A1C goals with GIP/GLP-1 RA [9].
Fixed-ratio combination (FRC) therapy combines basal insulin and GLP-1RAs. Compared to basal insulin alone, titratable FRCs have been shown to provide improved glycemic control and an acceptable safety profile, with a lower risk of hypoglycemia and potential weight gain in patients with T2DM [10]. The 2023 ADA SOC guidelines point to the potential benefits, such as simplified treatment regimens and more rapid achievement of glycemic control, of FRCs over the separate use of GLP-1 RA and basal insulin [9].
Insulin glargine (iGlar) 100 units/mL and lixisenatide are combined in iGlarLixi, a titratable FRC, which is given as a single, daily injection to patients with uncontrolled glycemic levels on a diet and exercise alone [11]. The efficacy and safety profile of iGlarLixi have previously been demonstrated in the LixiLan-L and LixiLan-O phase III, randomized, open-label, parallel-group trials, which included patients with T2DM who were not treated successfully on basal insulin ± OADs or metformin alone at randomization. In the LixiLan-O trial, iGlarLixi was associated with greater reductions in A1C levels from baseline compared to iGlar or lixisenatide after 30 weeks on a background dose of metformin 2000 mg or a lower dose of 1500 mg when patients were intolerant [12], while in the Lixilan-L trial, iGlarLixi achieved a greater reduction in A1C compared to iGlar [13]. Side effects, including symptomatic hypoglycemia, were comparable between insulin arms in both trials, while GI side effects were lower than lixisenatide alone in the LixiLan-O trial.
In addition, real-world evidence (RWE) studies, including SoliComplex [14], SoliPersistency [15], and those conducted in several European countries, including STAR-RO [16], iGLAR-6 M HU [17], and Ensure [18], have further pointed to the greater efficacy, enhanced safety profile, simplicity of administration, greater adherence/persistence, and lower pharmacy costs of iGlarLixi compared to alternative T2DM treatment options, including complex insulin regimens. However, additional larger-scale evaluations of varied real-world (RW) populations of patients who typically present in routine clinical practice, including patients having wider ranges of A1C levels compared to those in controlled clinical trials, are needed.
This study uses an integrated claims and EHR database to identify two RW cohorts of adults with T2DM who meet the criteria for treatment with iGlarLixi and applies a Monte Carlo simulation to mirror the treatment arms in the LixiLan-O and LixiLan-L trials and evaluate the clinical benefits of iGlarLixi.
Methods
This study was conducted in accordance with the Guidelines for Good Pharmacoepidemiology Practice [19]. Internal review board approval was not sought, as all analyses were based on a microsimulation applied to anonymized retrospective patient data. The electronic health record datasets analyzed during the current study are licensed by Sanofi from Optum, and permission to access and use data that are not publicly available from Optum was obtained.
Identification of Real-World Cohorts
The cohorts of patients with T2DM used for the simulation were derived from the Optum Humedica integrated EHR and claims database. These data consist of almost 107 million patients and include information on demographics (age, gender, race, ethnicity, geographic region), diagnostic codes, laboratory visits and tests, provider data, and information on dispensed prescription drugs, including National Drug Code (NDC), days of supply, dosage strength, and quantity.
Individuals with at least one diagnosis of T2DM (Table S1 in the Supplementary Information) from January 1st, 2007 to June 30th, 2021 (the most recent data available during study conduct) were first identified. The cohorts were then limited to adults (≥ 18 years old) with a valid A1C value [Logical Observation Identifiers Names and Codes (LOINC) 4548–4, 17,855–8, 17,856–6] in the range of 5% to 13% in the most recent year (July 1st, 2020 to June 30th, 2021). The most recent A1C reading was used to assign a patient-specific index date. Individuals were required to have continuous enrollment of at least 1 year prior to their index date, which was used to ascertain their baseline characteristics, A1C values, and background diabetes therapies.
To be included, individuals needed to have at least one anti-diabetic medication prescription and to have a body mass index (BMI) of between 10 and 40 kg/m2, as LixiLan trials included adults with BMI < 40 kg/m2. Only individuals with fills of basal insulins, with or without bolus, or intermediate-acting insulin (neutral protamine Hagedorn, NPH) and/or OADs [including metformin, sulfonylurea, alpha-glucosidase (AG) inhibitors, dipeptidyl peptidase-4 inhibitors (DPP-IVi), sodium-glucose cotransporter-2 (SGLT2) inhibitors, thiazolidinediones (TZD), and fixed-dose combinations of DPP-IVi and TZD, metformin and DPP-IVi, metformin and SGLT-2, metformin and sulfonylurea, metformin and TZD, SGLT-2 and DPP-IVi, and sulfonylurea and TZD] were included. Although the concomitant use of DPP-IVi with GLP-1 RA or iGlarLixi is not recommended, adults on DPP-IVi at baseline were included in the cohort as potential patients for treatment with iGlarLixi alone or in combination with metformin upon discontinuing DPP-IVi.
Individuals were excluded if they were treated with other classes of insulin or OADs for which there was no information about efficacy from the published literature, or if they had missing or unconventional (assumed erroneous) information on dosage. Individuals who were pregnant were also excluded.
Insulin and OAD dosages were calculated by multiplying each drug’s strength by its quantity and dividing it by days of supply. An overlap of different types of insulin therapies and OADs was allowed; however, those prescribed more than four different types of OADs as of their index date were excluded. The first cohort, termed the insulin cohort, consisted of individuals who were on a daily dosage of ≤ 60 units of basal insulin with or without OADs at the index date. A threshold daily dosage of ≤ 60 units of basal insulin was used, as this mirrors the maximum daily dose of the iGlar component of iGlarlixi. Individuals prescribed bolus insulin only, without any other insulins or OADs at index, were omitted from this cohort, as bolus insulin is short-acting and is usually prescribed with other insulins or OADs in the US. The second cohort, termed the OAD-only cohort, consisted of adults prescribed OADs only at index, excluding those prescribed any insulin.
Simulation
A Monte Carlo patient-level simulation model was developed to evaluate the benefits of iGlarLixi observed in the clinical trials in a varied RW population with baseline A1C levels and background therapies that align more closely with patients presenting in routine clinical practice. The principles and utility of patient-level simulations have been shown previously [20].
Bootstrapping with replacement was first used to generate 1,000,000 replicates for each of the two cohorts. This approach was consistent with previous applications of patient-level simulations [20]; larger samples drawn at random from the original cohorts allow for better incorporation of sampling uncertainty as well as stable estimates. Separate models following a patient-specific probabilistic path and the logic shown in Fig. 1 were then applied to each bootstrap-sampled cohort to emulate the treatment strategy and the treatment efficacy from the Lixilan-L and Lixilan-O trials. Background therapies like DPP-IVi, TZD, and SGLT2i except for metformin were removed to align with the treatment strategies from LixiLan-L and LixiLan- O trials, and the patient-specific baseline A1C was adjusted accordingly.

Conceptual representation of the patient-level microsimulation model used in this study
At baseline, an increment or reduction in A1C due to OAD/insulin treatment was applied to each cohort; this was based on estimates from the literature (Table S2 in the Supplementary Information), assuming a normal distribution of efficacy estimates for each treatment and applying an instantaneous A1C change. If a patient was on a fixed-dose combination OAD therapy, the efficacies of the individual OAD components were used due to the lack of efficacy data on all the combinations available in the RW data. Specifically, in the insulin cohort, if a sampled patient was on one or more OADs and/or on basal insulin during the 1-year prior period, their A1C value was adjusted using efficacies associated with specific OADs and basal insulin to create a patient profile with treatments resembling those of patients at randomization in the Lixilan-L trial. At index, the A1C value of a sampled patient treated with a metformin dose < 1500 mg during the prior 1-year period was adjusted using the efficacy associated with a metformin dose of 1500 mg. The A1C value of a metformin-treated patient whose dosage was ≥ 1500 mg was adjusted using the efficacy associated with that specific metformin dosage.
In the OAD-only cohort, if a sampled patient was on one or more OADs during the prior 1-year period, their A1C was adjusted using efficacy estimates associated with the specific OAD to create a patient profile with treatments resembling those of patients at randomization in the Lixilan-O trial. At index, the A1C value of a sampled patient treated with a metformin dose < 1500 mg or untreated with metformin during the prior 1-year period was adjusted using the efficacy associated with a metformin dose of 1500 mg. The A1C value of a sampled patient treated with a metformin dose ≥ 1500 mg during the 1-year lookback period was adjusted using the efficacy associated with that specific metformin dose.
For the insulin cohort simulation, two clones were created for each sampled patient, mirroring treatment with iGlarLixi vs. iGlar. Efficacy at 30 weeks was estimated for each clone, drawing from a normal distribution defined by parameters reported in the LixiLan-L trials and stratified by the value of A1C at index (Table S3 in the Supplementary Information). For the OAD-only cohort simulation, three clones were created for every sampled patient, mirroring treatments with iGlarLixi, lixisenatide, and iGlar, respectively. Efficacy at 30 weeks was simulated for each clone, drawing from a normal distribution informed by parameters reported in the Lixilan-O trial (Table S4 in the Supplementary Information).
Model-based estimates were summarized by calculating the average change in A1C levels and by calculating the proportion of patients who achieved age-based A1C goals at 30 weeks. For the latter, we used thresholds of ≤ 7% for ages < 65 years and ≤ 8% for ages ≥ 65 years aligned with the standards of care. In sensitivity analyses, thresholds of 7% and 8% were used for all patients.
Results
Description of the Two Cohorts
A total of 7,525,219 individuals with at least one diagnosis of T2DM were initially identified in the Optum data. After applying all exclusion and inclusion criteria, 3,798 and 17,633 individuals were identified for insulin and the OAD-only cohorts, respectively (Fig. 2).

CONSORT diagram
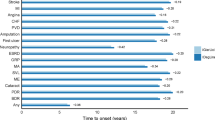
Table 1 summarizes the baseline characteristics of each cohort. The average age was 65.8 years in the insulin cohort and 64.2 in the OAD-only cohort. The average BMI was 29.8 kg/m2 in the insulin cohort (30.2 kg/m2 in the < 65 and 29.6 kg/m2 in the ≥ 65 years age groups) and 30.8 kg/m2 in the OAD-only cohort (31.8 kg/m2 in the < 65 and 30.0 kg/m2 in the ≥ 65 years age groups). The mean baseline A1C level in the insulin cohort was 8.9%, with a higher value for the < 65 (9.0%) compared to the ≥ 65 (8.5%) years age group. Similarly, in the OAD-only cohort, the average A1C level was 8.3%, with a higher mean value of 8.4% for the < 65 age group compared to 8.1% for those above 65 years. Nearly half (49.68%) of those in the insulin cohort and 43.59% of those in the OAD-only cohort were female. In both cohorts, the majority were Caucasian (71.8% and 71.9%, respectively), followed by African American (14.8% and 11.76%, respectively) and Asian cohorts (1.97% and 4.19%, respectively). Both cohorts were characterized by a high presence of comorbidities, with hypertension being the most prevalent (78.20% for the insulin cohort and 74.83% for the OAD-only cohort). Among different diabetic complications, diabetic neuropathy was the most prevalent for both the insulin cohort (28.79% for < 65 years and 36.06% for ≥ 65 years) and the OAD-only cohort (13.38% for < 65 years and 21.83% for ≥ 65 years). Overall, in both cohorts, the prevalence of comorbidities and complications was higher in the ≥ 65 years age group.
The RW cohorts differed considerably in their background OAD therapies compared to the population in the Lixilan-L and Lixilan-O trials. In the LixiLan-L cohort, a majority of patients were either on metformin only (48.9%) or a combination of metformin and sulfonylurea (SU) (34.6%) at screening. In the RW insulin cohort, 32.6% of patients were on metformin (18.8% on monotherapy), and 15.9% were on SU as a monotherapy or in combination with other OADs. Similarly, in the LixiLan-O trial, 53.9% were on SU, 0.3% were on sodium-glucose cotransporter-2 inhibitors (SGLT2i), and 2.4% were on dipeptidyl peptidase-4 inhibitors (DPP-IVi) at screening as second-line therapy in addition to metformin. In the OAD cohort, 69.7% were on metformin (36.7% on monotherapy), 38% of the patients were on SU, 16% were on SGLT2i, and 14.4% were on DPP-IVi as monotherapy or in combination with other OADs.
Insulin Cohort Simulation Estimates
Differences across the three arms in the insulin cohort simulation along with 95% confidence intervals (CIs) are presented in Table 2. When age-based thresholds were used, average A1C levels at week 30 decreased by 0.66 and the proportion who achieved age-based goals increased by 20.95 percentage points. When a threshold of ≤ 8% was used for all patients, average A1C levels at week 30 decreased by 0.66 and the proportion who achieved age-based goals increased by 18.97%. When a threshold of ≤ 7% was used for all patients, average A1C levels at week 30 decreased by 0.65 compared to A1C levels at intensification, and the proportion who achieved age-based goals increased by 26.11%.
OAD-Only Cohort Simulation Estimates
Differences across the three arms in the OAD-only cohort simulation, along with 95% CIs, are presented in Table 3. When age-based thresholds were used, average A1C levels at week 30 decreased by 0.36 and the proportion who achieved age-based goals increased by 10.61% in the iGlarLixi vs. iGlar comparison. Average A1C levels at week 30 decreased by 0.87 and the proportion who achieved age-based goals increased by 27.09% in the iGlarLixi vs. lixisenatide comparison.
When an A1C ≤ 8% threshold was used for all patients, average A1C levels at week 30 decreased by 0.38 and the proportion who achieved age-based goals increased by 10.38% in the iGlarLixi vs. iGlar comparison. Average A1C levels at week 30 decreased by 0.91 and the proportion who achieved age-based goals increased by 28.12% in the iGlarLixi vs. lixisenatide comparison. When an A1C ≤ 7 threshold was used for all patients, average A1C levels at week 30 decreased by 0.35 and the proportion who achieved age-based goals increased by 11.33% in the iGlarLixi vs. iGlar comparison. Average A1C levels at week 30 decreased by 0.84 and the proportion who achieved age-based goals increased by 28.12% in the iGlarLixi vs. lixisenatide comparison.
Discussion
Despite improvements during the past decade, achieving target glycemic control remains a challenge that is further complicated by higher rates of comorbidities, increased odds of impaired functional status and cognition, and likely lower persistence due to the complex treatment regimens often utilized by older adults with T2DM [21]. Nearly 50% of patients with T2DM who receive routine antidiabetic therapy do not maintain an A1C value of < 7.0%, and about 22% have an A1C value of > 8.0% [22]. In this patient-level simulation applied to two RW cohorts of patients with T2DM, iGlarLixi was consistently more effective than iGlar and lixisenatide alone in improving glycemic control by lowering A1C overall and in separate analyses of patients aged ≥ 65 years and those aged < 65 years.
These results are aligned with the existing evidence on the effectiveness of iGlarLixi; in the iGlarLixi-6 M HU study performed in a real-life setting in Hungary [17], a similar efficacy to the one in the Lixilan-O and Lixilan-L trials was reported. The SoliComplex study [14] reported higher persistence with iGlarLixi (43.7%) than multiple daily injection (MDI) or premixed insulin (22.3%) or free-dose combinations in the SoliPersistency study, along with similar adherence, a similar A1C reduction, and lower healthcare resource utilization and costs. Similar outcomes were observed for the STAR RO [16] study comparing iGlarLixi with OAD ± basal insulin and the SoliSimplify study [23] comparing iGlarLixi versus MDI insulin (RAI) regimen in adults with T2D, which reported that iGlarLixi exhibited equivalent glycaemic control to MDI without causing weight gain. Therefore, results from this, along with evidence from previous studies and the 2023 ADA SOC guidelines, suggest that in RW populations, iGlarLixi may outperform complex insulin regimens or iGlar and lixisenatide alone, as it achieves higher A1C reductions and better glycemic control without raising the risk of hypoglycemia, lowers weight gain, and improves gastrointestinal tolerability compared to its mono-components.
This study has clinically relevant implications for patients, practitioners, and payers. Overall, iGlarLixi offers simpler and more convenient treatment initiation, dosing schedules, and titration for healthcare professionals and patients as compared to complex insulin regimens [22]. Older adults face greater challenges related to T2DM management, driven by chronic illness, comorbidities, and the risk of overtreatment and related hypoglycemia [24]. Severe hypoglycemia among older adults has been linked with greater healthcare resource utilization and costs and higher mortality compared to non-severe and moderate hypoglycemia [25, 26]. The 2023 ADA SOC guidelines aim to reflect the clinical and treatment management complexity of older adults, including comorbidities, higher rates of cognitive impairment, and functional dependence. De-escalation, reducing treatment complexity, minimizing hypoglycemia, and recommending an individualized approach to A1C goals that depends on coexisting chronic illnesses have been emphasized in current clinical treatment guidelines for this heterogeneous population [9]. The 2023 ADA SOC guidelines list FRCs as agents with very high glycemic efficacy and recommend that patients who do not meet their A1C goals with GLP-1RA or GIP/GLP-1RA should be treated with FRCs. Because of its simple, once-daily dosing regimen, iGlarLixi may therefore be particularly suitable for older adults who require less treatment complexity to mirror their functional, social, and psychological status, and it has been proven to improve persistency in RWE studies. The SoliSimplify [23] and SoliComplex [14] studies compared real-world cohorts; however, additional studies need to evaluate the comparative risk of side effects, including hypoglycemia, among older adults initiating iGlarLixi instead of alternative treatments in real-world settings. Results from this study provide insights to healthcare professionals about the characteristics of patients who present in routine clinical practice. The majority in both cohorts were over 65 years old, and the vast majority had comorbidities, including depression, hyperlipidemia, chronic kidney disease (CKD), hypertension, and heart disease, further reinforcing the emphasis on patient-centered individualized treatment, particularly among older patients, as stated in the 2023 ADA SOC guidelines.
Reductions in A1C have been linked with reduced healthcare utilization and costs. For example, a large US-based study of patients with T2DM found that a 1 percentage point reduction in A1C levels resulted in about $545 lower annual total healthcare costs per patient [27]. Future studies are needed to directly quantify the economic benefits of iGlarLixi associated with A1C reduction in RW settings and the corresponding impact on Medicare and other payers.
The model results were validated by simulating the patient-level data from the LixiLan-L and LixiLan-O trials so that the A1C levels before treatment intensifications were the same. Each patient was simulated as being on treatments they were originally assigned in the trials, and the treatment effect was probabilistically sampled from a normal distribution generated from the reported parameters in the trials. For the LixiLan-L scenario, 54.5% of the patients achieved their A1C goal with iGlarlixi and 26.4% with iGlar, which is similar to the 54.8% and 29.6% of patients achieving their goal on iGlarlixi and iGlar, respectively, in the trial. Similarly, for the LixiLan-O scenario, 80.6% of the patients achieved their A1C goal with iGlarlixi, 66.3% with iGlar, and 35.9% with lixisenatide alone. In the trial, 73.7% of the patients achieved their A1C goal with iGlarlixi, 59.4% with iGlar, and 32.3% with lixisenatide alone.
Despite the higher A1C levels in these RWE cohorts, the proportion of patients achieving A1C goals continued to be significantly higher with iGlarlixi than with its mono-components, as was observed in the trials. While fewer patients achieved A1C goals due to a higher A1C before treatment intensification, both RW cohorts achieved a higher absolute reduction as compared to what was observed in the trials. In the insulin cohort, patients achieved an absolute A1C reduction of 2.4% and 1.7% on iGlarLixi and iGlar alone, respectively, as compared to the 1.1% and 0.6% absolute reductions in the iGlarLixi and iGlar-only treatment arms observed in the LixiLan-L trial. Similarly, in the OAD-only cohort, patients achieved an absolute A1C reduction of 1.8%, 1.4%, and 0.9% on iGlarLixi, iGlar only, and lixisenatide only, respectively, as compared to the 1.6%, 1.3%, and 0.8% absolute reductions in the iGlarLixi, iGlar-only, and lixisenatide-only treatment arms observed in the LixiLan-O trial.
Similar to previous studies, this study has several limitations. While it evaluated the impact of iGlarlixi on glycemic levels, due to the limited availability of data in the claims database, we were unable to model discontinuation specifically due to adverse side effects and GI side effects. The LixiLan-L and LixiLan-O trials, as well as results from several observational studies, have shown a lower risk of gastrointestinal side effects associated with iGlarLixi compared to lixisenatide alone and a lower weight gain compared to iGlar alone [12, 13]. In addition, this study relied on several assumptions related to baseline intensification and effectiveness at 30 weeks. These assumptions were informed by prior published evidence; however, further RW studies of iGlarlixi are warranted to provide additional support for its overall clinical benefits, risks, and impact on costs, especially in older patients, as iGlarLixi is available at a consistently low price of $35. To emulate patient treatments at randomization in the LixiLan trials, patients were removed from all background therapies except metformin, which might not always be the case in routine clinical practice for patients initiating iGlarLixi. Finally, the two cohorts obtained for this simulation were based on a large integrated claims and EHR dataset, which may not be fully representative of the US population; further, because of some missing data on dosage, number of RAI shots, and duration of T2DM, caution needs to be exercised in the interpretation and generalization of the study results.
Conclusion
In this patient-level simulation applied to two clinically and demographically varied RW cohorts of patients with T2DM with different baseline therapies, iGlarLixi was associated with a greater improvement in A1C levels compared to iGlar or lixisenatide alone. These results persisted in separate analyses among adults < 65 years as well as older patients (≥ 65 years of age) and when different A1C goals were used. These findings suggest that the benefits of iGlarLixi extend to clinically and demographically varied RW populations.
References
International Diabetes Federation. Diabetes data report 2000-2045. https://diabetesatlas.org/data/en/world/. Accessed 9 Sep 2022.
International Diabetes Federation. United States of America diabetes report 2000–2045. https://diabetesatlas.org/data/en/country/211/us.html. Accessed 7 Sep 2022.
American Diabetes Association. Economic costs of diabetes in the U.S. in 2017. Diabetes Care. 2018;41(5):917–28.
World Health Organization. Diabetes. https://www.who.int/news-room/fact-sheets/detail/diabetes. Updated 16 Sep 2022. Accessed 19 Sep 2022.
Centers for Disease Control and Prevention. National diabetes statistics report. https://www.cdc.gov/diabetes/data/statistics-report/index.html#print. Page last reviewed 18 Jan 2022. Accessed 7 Sep 2022.
Baker C, Retzik-Stahr C, Singh V, Plomondon R, Anderson V, Rasouli N. Should metformin remain the first-line therapy for treatment of type 2 diabetes? Ther Adv Endocrinol Metab. 2021;12:2042018820980225.
Pantalone KM, Wells BJ, Chagin KM, Ejzykowicz F, Yu C, Milinovich A, et al. Intensification of diabetes therapy and time until A1C goal attainment among patients with newly diagnosed type 2 diabetes who fail metformin monotherapy within a large integrated health system. Diabetes Care. 2016;39(9):1527–34.
Buysman EK, Fan T, Blauer-Peterson C, Miller-Wilson LA. Glycaemic impact of treatment intensification in patients with type 2 diabetes uncontrolled with oral antidiabetes drugs or basal insulin. Endocrinol Diabetes Metab. 2018;1(3): e00019.
ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, Collins BS, Cusi K, Das SR, Gibbons CH, Giurini JM, Hilliard ME, Isaacs D, Johnson EL, Kahan S, Khunti K, Kosiborod M, Leon J, Lyons SK, Murdock L, Perry ML, Prahalad P, Pratley RE, Seley JJ, Stanton RC, Sun JK, Woodward CC, Young-Hyman D, Gabbay RA. Summary of revisions: standards of care in diabetes 2023. Diabetes Care. 2023;46(Suppl 1):S5–9. https://doi.org/10.2337/dc23-Srev. (PMID: 36507641).
Rosenstock J, Handelsman Y, Vidal J, Ampudia Blasco FJ, Giorgino F, Liu M, et al. Propensity-score-matched comparative analyses of simultaneously administered fixed-ratio insulin glargine 100 U and lixisenatide (iGlarLixi) vs sequential administration of insulin glargine and lixisenatide in uncontrolled type 2 diabetes. Diabetes Obes Metab. 2018;20(12):2821–9.
Handelsman Y, Chovanes C, Dex T, Giorgino F, Skolnik N, Souhami E, et al. Efficacy and safety of insulin glargine/lixisenatide (iGlarLixi) fixed-ratio combination in older adults with type 2 diabetes. J Diabetes Complications. 2019;33(3):236–42.
Rosenstock J, Aronson R, Grunberger G, Hanefeld M, Piatti P, Serusclat P, et al. Benefits of LixiLan, a titratable fixed-ratio combination of insulin glargine plus lixisenatide, versus insulin glargine and lixisenatide monocomponents in type 2 diabetes inadequately controlled on oral agents: the LixiLan-O randomized trial. Diabetes Care. 2016;39(11):2026–35.
Aroda VR, Rosenstock J, Wysham C, Unger J, Bellido D, Gonzalez-Galvez G, et al. Efficacy and safety of LixiLan, a titratable fixed-ratio combination of insulin glargine plus lixisenatide in type 2 diabetes inadequately controlled on basal insulin and metformin: the LixiLan-L randomized trial. Diabetes Care. 2016;39(11):1972–80.
Lajara R, Heller C, Pantalone MK, Lew E, Li X, Dex T, Kilpatrick R. 739-P: iGlarLixi vs. premixed insulin initiation in adults with type 2 diabetes (T2D) advancing from basal insulin (BI) therapy: SoliComplex real-world study. Diabetes. 2022;71(Supplement 1):739.
Edelman S, Cassarino D, Kayne D, Dex T, Li X, Pasquel FJ. Treatment persistence and adherence in people with type 2 diabetes switching to iGlarLixi vs free-dose combinations of basal insulin and glucagon-like peptide 1 receptor agonist. J Manag Care Spec Pharm. 2022;28(9):958–68.
Bala C, Cerghizan A, Mihai BM, Moise M, Guja C. Real-world evidence on the use of a fixed-ratio combination of insulin glargine and lixisenatide (iGlarLixi) in people with suboptimally controlled type 2 diabetes in Romania: a prospective cohort study (STAR.Ro). BMJ Open. 2022;12(5):e060852.
Kis JT, Nagy G, Kovacs G. Effectiveness of IGlarLixi, a fixed-ratio combination of insulin glargine 100 U/mL and lixisenatide, in people with type 2 diabetes. Diabetes Ther. 2021;12(9):2517–29.
Candido R, Modugno M, Gabellieri E, Nicolucci A, Rossi Mc, Larosa M, et al. 110-LB: Efficacy, safety, and appropriateness of iGlarLixi, a fixed-ratio combination (FRC) in type 2 diabetes (T2D) in real-world settings: results from the ENSURE Study. Diabetes. 2021;70(Supplement 1).
International Society of Pharmacoepidemiology Public Policy Committee. Guidelines for good pharmacoepidemiology practice (GPP). Pharmacoepidemiol Drug Saf. 2016;25(1):2–10.
Cannon CP, Khan I, Klimchak AC, Reynolds MR, Sanchez RJ, Sasiela WJ. Simulation of lipid-lowering therapy intensification in a population with atherosclerotic cardiovascular disease. JAMA Cardiol. 2017;2(9):959–66.
Juarez DT, Ma C, Kumasaka A, Shimada R, Davis J. Failure to reach target glycated A1c levels among patients with diabetes who are adherent to their antidiabetic medication. Popul Health Manag. 2014;17(4):218–23.
Hinnen D, Strong J. iGlarLixi: a new once-daily fixed-ratio combination of basal insulin glargine and lixisenatide for the management of type 2 diabetes. Diabetes Spectr. 2018;31(2):145–54.
McCrimmon RJ, Cheng AYY, Galstyan G, Djaballah K, Li X, Coudert M, et al. iGlarLixi versus basal plus rapid-acting insulin in adults with type 2 diabetes advancing from basal insulin therapy: the SoliSimplify real-world study. Diabetes Obes Metab. 2023;25(1):68–77.
Mahoney GK, Henk HJ, McCoy RG. Severe hypoglycemia attributable to intensive glucose-lowering therapy among US adults with diabetes: population-based modeling study, 2011–2014. Mayo Clin Proc. 2019;94(9):1731–42.
Bajpai S, Wong-Jacobson S, Liu D, Mitchell B, Haynes G, Syring K, et al. Health care resource utilization and cost of severe hypoglycemia treatment in insulin-treated patients with diabetes in the United States. J Manag Care Spec Pharm. 2021;27(3):385–91.
McCoy RG, Van Houten HK, Ziegenfuss JY, Shah ND, Wermers RA, Smith SA. Increased mortality of patients with diabetes reporting severe hypoglycemia. Diabetes Care. 2012;35(9):1897–901.
Lage MJ, Boye KS. The relationship between HbA1c reduction and healthcare costs among patients with type 2 diabetes: evidence from a U.S. claims database. Curr Med Res Opin. 2020;36(9):1441–7.
Acknowledgements
The authors thank the study investigators and patients involved in the study.
Funding
The study was funded by Sanofi US, Bridgewater, New Jersey. The sponsor participated in the design and conduct of the study, the analysis of the data, and the preparation of this manuscript. The sponsor is also responsible for funding the Rapid Service Fee for publication. Ankita Chauhan, Mihail Samnaliev, Jennifer Ken-Opurum, Sistla S.S. Srinivas, and Aashay Mehta are consultants to Sanofi US.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Medical Writing and Editorial Assistance
Medical writing and editorial support were provided by Pratikshya Ray in accordance with Good Publication Practice guidelines [19], and were funded by Sanofi US.
Author Contributions
Ankita Chauhan, Mihail Samnaliev, Jennifer Ken-Opurum, Sistla S.S. Srinivas, Aashay M. Mehta, Terry Dex, Scott Charland, Andrew Revel, and Ronald Preblick contributed to the concept, design, data collection, interpretation, analysis, and drafting of the manuscript. All authors had full access to all the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
Disclosures
The authors Ankita Chauhan, Mihail Samnaliev, Jennifer Ken-Opurum, Sistla S.S. Srinivas, Aashay M. Mehta, Terry Dex, Scott Charland, Andrew Revel, and Ronald Preblick declare that they have no competing interests.
Compliance with Ethics Guidelines
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments. Internal review board approval was not sought, as all analyses were based on a microsimulation applied to anonymized retrospective patient data. The electronic health record datasets analyzed during the current study are licensed by Sanofi from Optum, and permission to access and use data not publicly available from Optum was obtained.
Data Availability
All data generated during this study are included in this published article. References to the original publications involving the data source utilized in this study have been listed in the main text of this manuscript. The electronic health record datasets analyzed during the current study are licensed by Sanofi from Optum, and are not publicly available.
Author information
Authors and Affiliations
Corresponding author
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Chauhan, A., Samnaliev, M., Ken-Opurum, J. et al. Clinical Benefits of Treating Patients with Type 2 Diabetes Mellitus with iGlarLixi: A Patient-Level Simulation Study. Diabetes Ther 14, 1331–1344 (2023). https://doi.org/10.1007/s13300-023-01419-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13300-023-01419-z