
Abstract
Background
The purpose of this work was to identify the results of pelvic exenteration for recurrent, persistent or locally advanced cervical cancer in terms of survival performed for 41 patients in Salah Azaiez Institute.
Patients and Methods
We conducted a retrospective unicentric study. The association between PE and OS was estimated using the method of Kaplan–Meier using SPSS ver 24.
Results
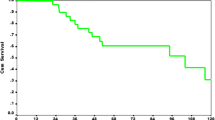
Median age at the time of intervention was 53.9 years old. FIGO stage IIB was the most frequent (46.3%). Eighteen patients had pelvic exenteration after neoadjuvant treatment. Resection margins were free of tumor in 83.3% of cases. Twenty-three patients underwent pelvic exenteration for recurrence of cervical cancer treated. The median time of recurrence was 23.4 months. Free resection margins were obtained in 69.5% of cases. Postoperative complications were noted in 61% of patients. Two deaths were seen in the early postoperative period. After a median follow-up of 40.5 months, 24.4% of recurrences were noted. Overall survival at 5 years was 51% and recurrence-free survival at one year was 39%. Prognostic factors which impact overall and recurrence-free survival were the size of recurrence and resection margins after exenteration. The time between the end of initial treatment and recurrence was the only predictive factor of recurrence after pelvic exenteration.
Conclusion
Pelvic exenteration remains a curative treatment of cervical cancer in certain indications despite high morbidity. A rigorous preoperative selection of candidate may reduce the morbidity and improve the survival of patients.



Similar content being viewed by others


References
Bray F, Ferlay J, Soerjomataram I, et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424.
Rozario SD, da Silva IF, Koifman RJ, et al. Characterization of women with cervical cancer assisted at Inca by histological type. Rev Saúde Pública. 2019;53:88.
Sardain H, Lavoué V, Foucher F, et al. L’exentération pelvienne curative en cas de récurrence d’un cancer du col de l’utérus à l’ère de la radio-chimiothérapie concomitante: revue de la littérature. J Gynécol Obstét Biol Reprod. 2016;45(4):315–29.
Marnitz S, Köhler C, Müller M, et al. Indications for primary and secondary exenterations in patients with cervical cancer. Gynecol Oncol. 2006;103(3):1023–30.
Brunschwig A. Complete excision of pelvic viscera for advanced carcinoma. A one-stage abdominoperineal operation with end colostomy and bilateral ureteral implantation into the colon above the colostomy. Cancer. 1948;1(2):177–83.
Ferron G, Pomel C, Martinez A, et al. Exentération pelvienne: actualités et perspectives. Gynécol Obstét Fertil. 2012;40(1):43–7.
Benn T, Brooks RA, Zhang Q, et al. Pelvic exenteration in gynecologic oncology: a single institution study over 20 years. Gynecol Oncol. 2011;122(1):14–8.
Unger JB, Ivy JJ, Connor P, et al. Detection of recurrent cervical cancer by whole-body FDG PET scan in asymptomatic and symptomatic women. Gynecol Oncol. 2004;94(1):212–6.
Höckel M. Laterally extended endopelvic resection. Gynecol Oncol. 2003;91(2):369–77.
LaPolla JP, Schlaerth JB, Gaddis O, et al. The influence of surgical staging on the evaluation and treatment of patients with cervical carcinoma. Gynecol Oncol. 1986;24(2):194–206.
Golda T, Biondo S, Kreisler E, et al. Follow-up of double-barreled wet colostomy after pelvic exenteration at a single institution. Dis Colon Rectum. 2010;53(5):822–9.
Schmidt A-M, Imesch P, Fink D, et al. Indications and long-term clinical outcomes in 282 patients with pelvic exenteration for advanced or recurrent cervical cancer. Gynecol Oncol. 2012;125(3):604–9.
Smith B, Jones EL, Kitano M, et al. Influence of tumor size on outcomes following pelvic exenteration. Gynecol Oncol. 2017;147(2):345–50.
Westin SN, Rallapalli V, Fellman B, et al. Overall survival after pelvic exenteration for gynecologic malignancy. Gynecol Oncol. 2014;134(3):546–51.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Hanene bouaziz is MD, Department of Surgical Oncology, Salah Azaiez Institute, Tunis, Tunisia; Nesrine Tounsi is a Surgery Oncologist, Department of Surgical Oncology, Salah Azaiez Institute, Tunis, Tunisia; Racha Ben Romdhane is a Resident, Department of Surgical Oncology, Salah Azaiez Institute, Tunis, Tunisia; Monia Hechiche is a Professor, Department of Surgical Oncology, Salah Azaiez Institute, Tunis, Tunisia; Maher Slimane is a Asst. Professor, Department of Surgical Oncology, Salah Azaiez Institute, Tunis, Tunisia; Khaled Rahal is a Professor, Department of Surgical Oncology, Salah Azaiez Institute, Tunis, Tunisia.
Rights and permissions
About this article

Cite this article
Bouraoui, I., Bouaziz, H., Tounsi, N. et al. Survival After Pelvic Exenteration for Cervical Cancer. J Obstet Gynecol India 72, 66–71 (2022). https://doi.org/10.1007/s13224-021-01502-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s13224-021-01502-0