
Abstract
Background
Deceased donor liver transplant (DDLT) is an uncommon procedure in India. We present our experience of DDLT from a public sector teaching hospital.
Methods
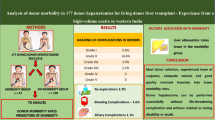
A retrospective analysis of all DDLT was performed from April 2012 till September 2016. Demographics, intraoperative, donor factors, morbidity, and outcome were analyzed.
Results
During the study period, 305 liver transplants were performed, of which 36 were DDLT (adult 32, pediatric 4; 35 grafts; 1 split). The median age was 42.5 (1–62) years; 78% were men. The median donor age was 28 (1–77) years; 72.2% were men. About 45% of organs were procured from outside of Delhi and 67% of all grafts used were marginal. Three of 38 liver grafts (7.8%) were rejected due to gross steatosis. Commonest indication was cryptogenic cirrhosis (19.4%). The median model for end-stage liver disease sodium and pediatric end-stage liver disease scores were 23.5 (9–40) and 14.5 (9–22), respectively. Median warm and cold ischemia times were 40 (23–56) and 396 (111–750) min, respectively. Major morbidity of grade III and above occurred in 63.8%. In hospital (90 days), mortality was 16.7% and there were two late deaths because of chronic rejection and biliary sepsis. The overall survival was 77.8% at median follow up of 8.6 (1–54) months.
Conclusions
DDLT can be performed with increasing frequency and safety in a public sector hospital. The perioperative and long-term outcomes are acceptable despite the fact that most organs were extended criteria grafts.


Similar content being viewed by others


References
Narasimhan G, Kota V, Rela M. Liver transplantation in India. Liver Transpl. 2016;22:1019–24.
Annual report 2015–2016. In: National Capital Region Planning Board. 2016. http://ncrpb.nic.in/pdf_files/Annual%20Report%202015-16.pdf. Accessed 15 Jan 2017
Organ Report. In: National Organ and Tissue Transplant Organization. 2014. http://www.notto.nic.in/organreport.htm. Accessed 15 Jan 2017.
Feng S, Goodrich NP, Bragg-Gresham JL, et al. Characteristics associated with liver graft failure: the concept of a donor risk index. Am J Transplant. 2006;6:783–90.
Gruttadauria S, Cintorino D, Mandala’ L, et al. Acceptance of marginal liver donors increases the volume of liver transplant: early results of a single-center experience. Transplant Proc. 2005;37:2567–8.
Briceño J, Marchal T, Padillo J, Solórzano G, Pera C. Influence of marginal donors on liver preservation injury. Transplantation. 2002;74:522–6.
Briceño J, Solórzano G, Pera C. A proposal for scoring marginal liver grafts. Transpl Int. 2000;13 Suppl 1:S249–52.
Briceno J, Lopez-Cillero P, Rufian S, et al. Impact of marginal quality donors on the outcome of liver transplantation. Transplant Proc. 1997;29:477–80.
Briceño J, Padillo J, Rufián S, Solórzano G, Pera C. Assignment of steatotic livers by the Mayo model for end-stage liver disease. Transpl Int. 2005;18:577–83.
Tisone G, Manzia TM, Zazza S, et al. Marginal donors in liver transplantation. Transplant Proc. 2004;36:525–6.
Adam R, Cailliez V, Majno P, et al. Normalised intrinsic mortality risk in liver transplantation: European Liver Transplant Registry study. Lancet. 2000;356:621–7.
Verran D, Kusyk T, Painter D, et al. Clinical experience gained from the use of 120 steatotic donor livers for orthotopic liver transplantation. Liver Transpl. 2003;9:500–5.
Nickkholgh A, Weitz J, Encke J, et al. Utilization of extended donor criteria in liver transplantation: a comprehensive review of the literature. Nephrol Dial Transplant. 2007;22 Suppl 8:viii29–36.
Bruzzone P, Giannarelli D, Adam R, European Liver and Intestine Transplant Association, European Liver Transplant Registry. A preliminary European Liver and Intestine Transplant Association-European Liver Transplant Registry study on informed recipient consent and extended criteria liver donation. Transplant Proc. 2013;45:2613–5.
Joya-Vazquez PP, Dodson FS, Dvorchik I, et al. Impact of anti-hepatitis Bc-positive grafts on the outcome of liver transplantation for HBV-related cirrhosis. Transplantation. 2002;73:1598–602.
Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240:205–13.
Englesbe MJ, Merion RM. The riskiest job in medicine: transplant surgeons and organ procurement travel. Am J Transplant. 2009;9:2406–15.
Routh D, Sharma S, Naidu CS, Rao PP, Sharma AK, Ranjan P. Comparison of outcomes in ideal donor and extended criteria donor in deceased donor liver transplant: a prospective study. Int J Surg. 2014;12:774–7.
Godara R, Naidu CS, Rao PP, et al. Use of marginal grafts in deceased donor liver transplant: assessment of early outcomes. Indian J Gastroenterol. 2014;33:136–40.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
VP, DPB, SK, KGSB, PKS, SVS, VS, CKP, and SKS declare that they have no conflicts of interest.
Ethics statement
The study was approved by the institute’s ethics review board and is in compliance with the Helsinki Declaration, 1964, and its subsequent modifications. Standard medical care was provided to all participants. Written informed consent in a standard format was obtained from all patients who underwent surgery. Since this was a retrospective study, participation in this study did not change the consent process or decision for surgery. Formal consent for participation in this study is therefore not required.
Rights and permissions
About this article

Cite this article
Pamecha, V., Borle, D.P., Kumar, S. et al. Deceased donor liver transplant: Experience from a public sector hospital in India. Indian J Gastroenterol 37, 18–24 (2018). https://doi.org/10.1007/s12664-017-0801-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12664-017-0801-1