
Abstract
Purpose
The purpose of this paper is to review the current evidence relating anesthetic depth to long-term survival after surgery.
Source
Using PubMed as the principal source, this review included published studies in all languages comparing mortality in patients with low- and high-processed electro-encephalo-graphic index values.
Principal findings
All published studies used the bispectral index (BIS) monitor to measure anesthetic depth. The majority of the published observational studies were post hoc analyses of studies undertaken for other purposes. Most of these studies report a statistically significant association between deep general anesthesia (i.e., BIS values < 45) and death. Some studies also suggest an association between deep general anesthesia and myocardial infarction or postoperative cognitive decline. The combination of low BIS values and low delivered anesthetic concentrations (thus defining increased anesthetic sensitivity) may identify patients at particularly high risk. One of the three available randomized controlled trials reports worse outcomes in the BIS = 50 group compared with the BIS > 80 group, and two report no difference in mortality between the BIS = 35 and BIS = 50-55 groups.
Conclusions
The available evidence on anesthetic depth and long-term survival is inconclusive. Randomized controlled trials with carefully controlled arterial blood pressure are required.
Résumé
Objectif
L’objectif de cet article est de passer en revue les données probantes actuelles reliant la profondeur de l’anesthésie et la survie à long terme après une chirurgie.
Source
En utilisant PubMed comme source principale, ce compte-rendu a inclus les études publiées, toutes langues confondues, comparant la mortalité chez les patients avec des valeurs d’indice bispectral peropératoire bas ou élevé.
Constatations principales
Toutes les études publiées se sont fondées sur le moniteur de l’indice bispectral (BIS) pour mesurer la profondeur de l’anesthésie. La majorité des études observationnelles publiées étaient en fait des analyses post hoc d’études menées à d’autres fins. La plupart de ces études rapportent une association significative d’un point de vue statistique entre une anesthésie générale profonde (soit des valeurs de BIS < 45) et le décès. Certaines études suggèrent également qu’il existerait une association entre une anesthésie générale profonde et l’infarctus du myocarde ou le déclin cognitif postopératoire. La combinaison de faibles valeurs de BIS et de faibles concentrations anesthésiques (définissant ainsi une sensibilité anesthésique accrue) pourrait peut-être identifier les patients à risque particulièrement élevé. L’une des trois études randomisées contrôlées disponibles rapporte des pronostics moins bons dans le groupe où les valeurs de BIS = 50 par rapport au groupe aux valeurs de BIS > 80, et deux ne rapportent aucune différence en matière de mortalité entre les groupes de BIS = 35 et BIS = 50-55.
Conclusion
Les données probantes dont nous disposons sur le lien entre la profondeur de l’anesthésie et la survie à long terme ne sont pas concluantes. Il faut réaliser d’autres études randomisées contrôlées dans lesquelles la pression artérielle sera contrôlée de façon minutieuse.
Similar content being viewed by others


Anesthetic administration based on population estimates of dosing that prevent movement or response to command in the vast majority of patients inevitably leads to some patients receiving more anesthesia than they need.1,2 This can result in unwanted consequences such as hypotension and/or low cardiac output in patients with low cardiovascular reserve. With the increasing number of elderly and frail patients having surgery, there has been a similarly increasing need to provide the optimal depth of anesthesia for each patient rather than administering population-based doses of anesthetics to everyone.3
We define the optimal depth of general anesthesia as one in which the patient is at low risk of recall of intraoperative events, even if the balance between anesthetic delivery and surgical stimulation changes suddenly for any reason. In addition, the optimal depth should allow maintenance of blood pressure and heart rate at acceptable levels with minimal intervention and should avoid or easily manage hemodynamic responses to stress. An optimal depth prevents patient movement even when muscle relaxants are not used and allows the patient to emerge from anesthesia shortly after the end of the procedure, free of side effects and ready for assessment and prompt discharge to the ward or home.
Achieving the optimal depth of general anesthesia for each patient can be challenging.4,5 Most factors encourage the delivery of relatively deep general anesthesia - i.e., the patient does not want to be aware,6 the surgeon wants good operating conditions,7 and for the anesthesiologist, deeper anesthesia smooths its delivery and requires fewer dose adjustments in anticipation of changing surgical stimulation.8 Fewer factors encourage striving for a lighter depth of anesthesia that is slightly deeper than that required to prevent awareness. The use of short-acting hypnotic and analgesic drugs generally allows patients to emerge rapidly from deeper general anesthesia regardless of the depth obtained.8 The issue of waste and environmental pollution, a consequence of the delivery of anesthetic drugs in excess of requirements, is rarely discussed.9 Thus, relatively deep general anesthesia is the norm in routine clinical practice.10-12 Nevertheless, recent research suggests an association between deep general anesthesia and poorer outcomes in surgical patients.4,5,11,13-21 The dilemma is whether this evidence is strong enough for clinicians to change their practice.
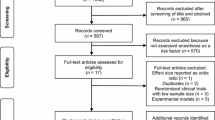
Our aim, therefore, was to review the current evidence relating anesthetic depth to long-term survival after surgery. We searched the peer-reviewed literature using PubMed. Published studies in all languages comparing mortality in patients with low- and high-processed electro-encephalo-graphic (EEG) index values are included in the review. Our review follows a chronological sequence as the evidence was published.
Measuring the depth of general anesthesia
We use ‘deep’ and ‘light’ general anesthesia in this review because these terms are widely used and understood. We do not use these terms to imply excessive or inadequate anesthesia - these are defined by the outcome for the patient. In the absence of EEG monitoring, the depth of anesthesia is usually extrapolated from clinical signs, hemodynamic responses, and the delivery of anesthetic drugs as predicted by the end-tidal concentration of inhaled anesthetics and the modelled effect-site concentration of intravenous anesthetics.22 When processed EEG monitors such as the bispectral index (BIS) are used, additional information is available in the form of the index value as well as the amount of burst suppression on the raw EEG.22,23 Light general anesthesia is identified by BIS values of 50-60, and deep general anesthesia is identified by BIS values < 40 and the advent of burst suppression, which commonly occurs with BIS values < 30.22,23 The inclusion of processed EEG indices in intraoperative patient monitoring allows anesthesiologists to identify patients who are more or less sensitive to anesthetics (i.e., have a lower or higher BIS value than would normally be expected from clinical signs, hemodynamic indices, and anesthetic delivery indices).23
Observational studies on anesthetic depth and poor outcomes
The majority of observational studies have been post hoc analyses of studies undertaken for other purposes, for example, determining whether the use of processed EEG monitors reduces the incidence of awareness. All have used the BIS monitor to measure anesthetic depth, and most report statistically significant associations between BIS values < 45 and death.
Monk et al. 13 published a novel study describing an association between low BIS values and poorer survival. They studied patients aged ≥ 18 yr presenting for major noncardiac surgery and reported that longer duration of anesthesia with BIS values < 45 was associated with poorer one-year survival (Table 1). In his editorial accompanying the Monk et al. study, Cohen24 highlighted the arbitrary nature of this definition of deep anesthesia and the reliance on the BIS monitor for its measurement. This limitation applies to all subsequent studies that have relied on BIS to define anesthetic depth.4,5,11,14-16,19-21,25,26
Monk et al. 13 speculated that the reason for the association might be an inherently toxic effect of anesthetics, perhaps through a pro-inflammatory mechanism.27,28 These effects may not only increase mortality but also impair cognitive function as volatile anesthetics have been associated with neuronal apoptosis in rodents29,30 and cognitive decline in rodents31 and humans.12,32 In a recent review, Hudson and Hemmings33 counselled: “It is unlikely that definitive clinical studies absolving general anesthetics of neurotoxicity will become available in the near future, requiring clinicians to use careful judgement when using these profound neuro-depressants in vulnerable patients”.
Both Monk et al.13 and Cohen24 called for carefully planned randomized controlled trials that would further explore the association between anesthetic depth and poor outcomes. In the ensuing years, however, most of the new evidence has arisen from post hoc analyses of cohort studies and randomized controlled trials established to investigate other hypotheses, each with nuances that add to the controversy (Table 2). For example, Lindholm et al. 11 conducted a suite of studies on adult noncardiac surgery patients originally recruited to a cohort study on awareness. In the first study, longer durations with BIS values < 45 were associated with poorer two-year survival, but only if pre-existing malignancy was not included in the regression model (Table 1). As Kalkman et al.34 subsequently pointed out, when covariates that are strongly associated with mortality are included, it becomes more difficult to establish the influence of covariates with weaker associations.
The immune compromise associated with general anesthesia may promote the growth and metastatic ability of cancer cells that survive after surgery; this might explain the association of increased mortality with higher anesthetic doses.35-37 Lindholm et al. progressed to investigating a dose-response relationship with cancer progression by looking at the duration of anesthesia and duration of BIS < 45 in two groups of patients.14,15 They reported no association between either the duration of anesthesia or the duration of BIS < 45 and the development of new malignancies within five years in patients with15 or without14 known malignancy at the time of the index surgery (Table 1). This analysis was limited, however, by the fact that a number of potentially important covariates (e.g., opioid administration) could not be included due to lack of evidence about how to categorize the information. Nevertheless, the relationship between deep anesthesia and cancer progression remains speculative at best.
Other authors have reported on post hoc analyses of patients randomized to clinical trials. In our own study,16 we examined long-term follow-up of patients in the B-Aware Trial38 who were randomized to BIS-guided anesthesia or routine care. The risk of poor outcomes was not significantly different between the two groups; however, patients with BIS values < 40 for more than five minutes appeared at greater risk of death than patients who never recorded these values (Table 1). Deep anesthesia was also associated with greater risk of myocardial infarction and stroke. In his editorial commentary on this study, Kurata39 noted the lack of detailed information about hypotension as a limitation of this study relative to others. Indeed, the lack of availability of key covariates is common in post hoc analyses of studies designed for another purpose.
Intraoperative hypotension has been independently associated with poor outcomes in numerous studies, including many quoted in this review13,16,17,19,20,26 and has been proposed as a mediator between deep anesthesia and poor outcomes.39-41 The degree and duration of hypotension resulting in harm likely varies from individual to individual,41,42 but on an empiric basis, a mean arterial pressure (MAP) of < 55 mmHg has been identified as requiring immediate treatment.43 Avoidance of confounding by arterial hypotension will be vital to a definitive randomized controlled trial of anesthetic depth and poor outcomes.44
The next set of analyses arose from the B-Unaware Trial45 which randomized patients at risk of awareness to either BIS-guided or end-tidal anesthetic concentration-guided anesthesia. The risk of poor outcomes was not significantly different between the two groups.25,26 In the cardiac surgery subgroup, a longer cumulative duration of time spent with BIS < 45 was associated with poorer long-term survival (Table 1).25 This finding was not replicated in the noncardiac surgery group where there was no significant association between anesthetic depth and death (Table 1).26 Kertai et al. concluded that the discrepancy between their two studies indicated that low BIS values were an epiphenomenon of the relationship between anesthetic sensitivity and poor outcomes.26
Anesthetic sensitivity is evidenced by indications of excessively deep anesthesia (usually defined by a lower than expected processed EEG index) concurrent with low anesthetic delivery (usually defined by low minimum alveolar concentration [MAC] values) and likely reflects patient comorbidity and/or frailty. Low MAC has been reported as an independent risk factor for mortality in several studies,19,46 suggesting, unfortunately, that the problem may not be controllable - at least not during the anesthetic. This conclusion was emphasised by Monk and Weldon47 who wondered: “Is low BIS just a marker of comorbidity and imminent death or will intraoperative BIS optimization improve outcomes in high-risk patients?”
All the foregoing studies based their assessment of anesthetic depth on BIS values. Two studies instead used the suppression ratio (SR) generated by the BIS monitor to explore the relationship between burst suppression and outcomes. The SR is the percentage of the previous 63-sec epoch of EEG that is recognized as being isoelectric. In their innovative study, Watson et al.18 reported that the presence of any SR value > 0 was associated with higher mortality, which, in their study, was assessed at six months in mechanically ventilated intensive care patients (Table 1). This raised the possibility that the burst suppression pattern associated with low BIS values48 rather than the BIS value itself is associated with poor outcomes. Subsequently, Willingham et al.17 combined data from the B-Unaware45 and BAG-RECALL49 studies and reported that more than five cumulative minutes of SR > 0 was not associated with death at 90 days, although the interaction between burst suppression and MAP was significant (Table 1). In our editorial commentary to their study,50 we pointed out that the increased effort to adjust for confounding factors in the Willingham study compared with the Watson study and the difference in the length of time to the assessment of mortality risk may have accounted for their discordant results.
Burst suppression is not a normal physiological EEG rhythm.23,48 It can be produced by anesthetic agents, hypothermia, and a range of cerebral ischemic insults, and it is associated with long-term cerebral damage.51 In the context of general anesthesia, the onset of burst suppression often represents unnecessarily deep anesthesia,23 although care should be taken to rule out the other more sinister causes.
The largest observational study to date was conducted by Sessler et al. at the Cleveland Clinic.19 The authors collected BIS, MAP, MAC, and 30-day outcome data in 24,210 patients. They performed a case-based analysis based on their hospital mean (SD) BIS, MAP, and MAC that defined the reference state [46 (4), 87 (5) mmHg, and 0.56 (0.11), respectively] with low and high values defined as > 1 standard deviation from the mean. They also conducted a time-based analysis based on thresholds that discriminated well between patients who survived 30 postoperative days and those who did not (MAP < 75 mmHg, BIS < 45, and MAC < 0.8).
In the case-based analysis, patients with low BIS values but high MAP and MAC values (‘single low’) had lower 30-day mortality than reference patients (Table 1). A combination of low BIS and low MAP (‘double low’) was not associated with a significant effect on survival. In fact, only a ‘double low’ that included low MAC or a ‘triple low’ with low MAC, BIS, and MAP was significantly associated with 30-day mortality, providing support for the theory that anesthetic sensitivity is the crucial element in this equation. In the time-based analysis, longer duration of triple low was associated with higher mortality and longer duration of hospital stay. Sessler et al. are continuing this line of research with a randomized controlled trial in which anesthesiologists are alerted (or not) to low values occurring during each of their cases and a primary outcome of 90-day mortality is measured (ClinicalTrials.org NCT00998894).
In their editorial commentary, Kheterpal and Avidan highlighted the centre-specific thresholds for the case-based analyses as a limitation.40 For example, a MAP of 82 mmHg is higher than common definitions of hypotension.43 Clinically relevant thresholds rather than centre-specific means would have increased the generalizability of the results.
Subsequently, investigators at the Duke University Medical Center also investigated the ‘triple low’ and its relationship with mortality. In their study, Kertai et al. 20 conducted a time-based analysis using thresholds of BIS < 45, MAP < 75 mmHg, and MAC < 0.7. Longer cumulative duration of triple low and cumulative duration of low BIS were not associated with increased 30-day mortality in their study (Table 1). Myles52 commented that “The weight of evidence supporting a causal relation between triple low, or a low BIS, and excess mortality is unconvincing, but the concept is not yet ready to be dismissed because the triple low state … is potentially modifiable such that it could change how we practice anesthesia around the world.” Once again, the authors20 and editorialist52 called for definitive randomized controlled trials.
Randomized trials on anesthetic depth and outcome
All the randomized trials to date have used the BIS monitor to measure anesthetic depth. One trial reported increased mortality in a BIS = 50 group vs a BIS > 80 group, and two reported no difference between BIS = 35 and BIS = 50-55 groups.
A novel randomized controlled trial designed specifically for this purpose - the Dexamethasone, Light Anesthesia, and Tight Glucose Control (DeLiT) study - aimed to test interventions that may reduce inflammation following anesthesia and surgery.4 Deep anesthesia was defined as BIS = 35 and light anesthesia as BIS = 55. Unfortunately, the trial was stopped when an interim analysis revealed that all three interventions crossed futility boundaries for the primary outcome of death and major complications at 30 days postoperatively. Mean (SD) BIS values in the deep and light groups were 44 (7) and 50 (6), respectively, and anesthetic depth had no significant effect on the primary outcome (Table 1).
In one study to date on sedation, Brown et al. 21 randomized elderly patients to deep (BIS = 50) and light (BIS > 80) sedation during spinal anesthesia for hip fracture surgery. The primary analysis revealed significantly more delirium in the deep than in the light sedation patients,53 consistent with other recent work.12,54 In the follow-up study,21 the authors reported no difference in one-year mortality between patients receiving deep vs light sedation (Table 1). Nevertheless, in patients with significant comorbidities (Charlson score55 > 4), there was a significant association between deep sedation and poorer survival. There was no evidence that intraoperative hypotension or postoperative delirium were mediators in determining one-year mortality. In our accompanying editorial,56 we highlighted the small sample size of this study, which increases the risk of imbalance in baseline characteristics (seen in this study), the risk of failing to show a true effect, and the risk of showing a spurious effect. The advantage of studying patients at high risk of poor outcomes was matched by the reduced generalizability of the results.
The Australian and New Zealand College of Anaesthetists Clinical Trials Network (http://www.anzca.edu.au/fellows/Research/clinical-trials-network.html) is leading an international randomized controlled trial of deep (BIS = 35) and light (BIS = 50) volatile-based general anesthesia (the Balanced Anesthesia Study) (Australian New Zealand Clinical Trials Registry No: 12612000632897). In total, 6,500 patients will be required to explore our hypothesis of a 20% relative risk reduction for one-year mortality in the BIS = 50 group. The choice of BIS targets for light and deep anesthesia was based on previous studies where BIS has been blinded and on the manufacturer’s recommendations.44 Anesthesiologists will also be asked to maintain MAP between patient-specific limits that they identify before randomization.
We prepared for the main trial with a pilot study in 125 patients recruited at five centres (Table 1).5 Pilot study results showed a significant difference between the BIS or spectral entropy values (mean difference, 8; 95% confidence interval [CI], 6 to 10; P < 0.001) and end-tidal anesthetic concentrations (mean difference, −0.35; 95% CI, −0.44 to −0.26; P <0.001), while MAPs in the two groups were similar (mean difference, 2; 95% CI, −2 to 6; P = 0.86). Ten percent of the patients died by one year postoperatively, and the incidence of death or major complications was 28% in the BIS = 35 group and 17% in the BIS = 50 group (P = 0.15).
The Balanced Anesthesia Study will have important ramifications regardless of the results. If results show an important outcome difference, anesthesiologists will have strong guidance that can be implemented immediately. If no difference is present, anesthesiologists can be confident in choosing the depth of anesthesia that is appropriate for the patient and the surgery. Secondary analyses will illuminate the relationship between anesthetic sensitivity (i.e., there will be patients who self-identify as ‘sensitive’ by having low BIS and low MAC) and poor outcomes. If actively targeting specific BIS values in these high-risk patients proves clinically unfeasible (as it did in the DeLiT study),4 we will have important information about the utility of this intervention. At the time of writing (May 10, 2015), 2,331 patients had been recruited at 50 centres worldwide (http://balancedstudy.org.nz).
Conclusions
We have described the available evidence from observational and randomized controlled trials on the relationship between anesthetic depth and long-term survival after surgery. All studies used the BIS monitor to describe anesthetic depth. The evidence from these studies is inconclusive, and the proposed mechanisms for poorer outcomes are speculative. A causality dilemma remains: Is deep general anesthesia the cause of poor outcomes or do low BIS values reflect anesthetic sensitivity as a marker of a high-risk patient?
We previously proposed a model3 explaining this causality dilemma. In this model, we proposed that excessive anesthetic administration - either in absolute terms as evidenced by high MAC values or in relative terms as evidenced by lower MAC values than expected in a similar group of patients - leads to low processed EEG index values, but it has its deleterious effects on outcome via direct toxic effects or organ hypoperfusion (or both). It is also acknowledged, however, that frail patients in poor health, as evidenced by sensitivity to anesthetics, may also suffer worse outcomes because of their poor health and frailty and not due to anesthetic effects per se. It is important to understand the limitations of such models as this as well as observational research. The only way to resolve this causality dilemma is with carefully designed randomized controlled trials.
What options are open to anesthesiologists as they read the literature on this subject and wait for definitive evidence? We recommend that they strive for the optimal anesthetic depth, deep enough to avoid intraoperative responsiveness and postoperative recall but light enough to avoid intraoperative hypotension and postoperative side effects. Titration of anesthetic depth using a processed EEG monitor and attention to clinical signs, hemodynamic responses, and anesthetic delivery indices will allow identification of patients with anesthetic sensitivity.
References
Smith C, McEwan AI, Jhavieri R, et al. The interaction of fentanyl on the CP50 of propofol for loss of consciousness and skin incision. Anesthesiology 1994; 81: 820-8.
Chortkoff BS, Eger EI 2nd, Crankshaw DP, Gonsowski CT, Dutton RC, Ionescu P. Concentrations of desflurane and propofol that suppress response to command in humans. Anesth Analg 1995; 81: 737-43.
Leslie K, Short TG. Low bispectral index values and death: the unresolved causality dilemma. Anesth Analg 2011; 113: 660-3.
Abdelmalak BB, Bonilla A, Mascha EJ, et al. Dexamethasone, light anaesthesia, and tight glucose control (DeLiT) randomized controlled trial. Br J Anaesth 2013; 111: 209-21.
Short TG, Leslie K, Campbell D, et al. A pilot study for a prospective, randomized, double-blind trial of the influence of anesthetic depth on long-term outcome. Anesth Analg 2014; 118: 981-6.
Gan TJ, Ing RJ, de L Gear G, Wright D, El-Moalem HE, Lubarsky DA. How much are patients willing to pay to avoid intraoperative awareness? J Clin Anesth 2003; 15: 108-12.
McIntosh C, Macario A. Managing quality in an anesthesia department. Curr Opin Anaesthesiol 2009; 22: 223-31.
Song D, Joshi GP, White PF. Titration of volatile anesthetics using bispectral index facilitates recovery after ambulatory anesthesia. Anesthesiology 1997; 87: 842-8.
McGain F, Naylor C. Environmental sustainability in hospitals - a systematic review and research agenda. J Health Serv Res Policy 2014; 19: 245-52.
Gan TJ, Glass PS, Windsor A, et al. Bispectral index monitoring allows faster emergence and improved recovery from propofol, alfentanil, and nitrous oxide anesthesia. Anesthesiology 1997; 87: 808-15.
Lindholm M, Traff S, Granath F, et al. Mortality within 2 years after surgery in relation to low intraoperative bispectral index values and preexisting malignant disease. Anesth Analg 2009; 108: 508-12.
Chan MT, Cheng BC, Lee TM, Gin T, CODA Trial Group. BIS-guided anesthesia decreases postoperative delirium and cognitive decline. J Neurosurg Anesthesiol 2013; 25: 33-42.
Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg 2005; 100: 4-10.
Lindholm ML, Granath F, Eriksson LI, Sandin R. Malignant disease within 5 years after surgery in relation to duration of sevoflurane anesthesia and time with bispectral index under 45. Anesth Analg 2011; 13: 778-83.
Lindholm ML, Brudin L, Sandin RH. Cumulated time with low bispectral index values is not related to the risk of new cancer or death within 5 years after surgery in patients with previous or prevailing malignancy. Anesth Analg 2014; 118: 782-7.
Leslie K, Myles PS, Forbes A, Chan MT. The effect of bispectral index monitoring on long-term survival in the B-Aware trial. Anesth Analg 2010; 110: 816-22.
Willingham M, Ben Abdallah A, Gradwohl S, et al. Association between intraoperative electroencephalographic suppression and postoperative mortality. Br J Anaesth 2014; 113: 1001-8.
Watson PL, Shintani AK, Tyson R, Pandharipande PP, Pun BT, Ely EW. Presence of electroencephalogram burst suppression in sedated, critically ill patients is associated with increased mortality. Crit Care Med 2008; 36: 3171-7.
Sessler DI, Sigl JC, Kelley SD, et al. Hospital stay and mortality are increased in patients having a “triple low” of low blood pressure, low bispectral index, and low minimum alveolar concentration of volatile anesthesia. Anesthesiology 2012; 116: 1195-203.
Kertai MD, White WD, Gan TJ. Cumulative duration of “triple low” state of low blood pressure, low bispectral index, and low minimum alveolar concentration of volatile anesthesia is not associated with increased mortality. Anesthesiology 2014; 121: 18-28.
Brown CH 4th, Azman AS, Gottschalk A, Mears SC, Sieber FE. Sedation depth during spinal anesthesia and survival in elderly patients undergoing hip fracture repair. Anesth Analg 2014; 118: 977-80.
Bruhn J, Myles PS, Sneyd R, Struys MM. Depth of anaesthesia monitoring: what’s available, what’s validated and what’s next? Br J Anaesth 2006; 97: 85-94.
Bennett C, Voss LJ, Barnard JP, Sleigh JW. Practical use of the electroencephalogram waveform during general anesthesia: the art and science. Anesth Analg 2009; 109: 539-50.
Cohen NH. Anesthetic depth is not (yet) a predictor of mortality! Anesth Analg 2005; 100: 1-3.
Kertai MD, Pal N, Palanca BJ, et al. Association of perioperative risk factors and cumulative duration of low bispectral index with intermediate-term mortality after cardiac surgery in the B-Unaware Trial. Anesthesiology 2010; 112: 1116-27.
Kertai MD, Palanca BJ, Pal N, et al. Bispectral index monitoring, duration of bispectral index below 45, patient risk factors and intermediate-term mortality after noncardiac surgery in the B-Unaware Trial. Anesthesiology 2011; 114: 545-56.
Crozier TA, Muller JE, Quittkat D, Sydow M, Wuttke W, Kettler D. Effect of anaesthesia on the cytokine responses to abdominal surgery. Br J Anaesth 1994; 72: 280-5.
Kudoh A, Katagai H, Takazawa T, Matsuki A. Plasma proinflammatory cytokine response to surgical stress in elderly patients. Cytokine 2001; 15: 270-3.
Chen G, Gong M, Yan M, Zhang X. Sevoflurane induces endoplasmic reticulum stress mediated apoptosis in hippocampal neurons of aging rats. PloS One 2013; 8: e57870.
Istaphanous GK, Ward CG, Nan X, et al. Characterization and quantification of isoflurane-induced developmental apoptotic cell death in mouse cerebral cortex. Anesth Analg 2013; 116: 845-54.
Culley DJ, Baxter MG, Yukhananov R, Crosby G. Long-term impairment of aquisition of a spatial memory task following isoflurane-nitrous oxide anesthesia in rats. Anesthesiology 2004; 100: 309-14.
Ballard C, Jones E, Gauge N, et al. Optimised anaesthesia to reduce post operative cognitive decline (POCD) in older patients undergoing elective surgery, a randomised controlled trial. PloS One 2012; 7: e37410.
Hudson AE, Hemmings HC Jr. Are anaesthetics toxic to the brain? Br J Anaesth 2011; 107: 30-7.
Kalkman CJ, Peelan LM, Moons KG. Pick up the pieces: depth of anesthesia and long-term mortality. Anesthesiology 2011; 114: 485-7.
Gottschalk A, Sharma S, Ford J, Durieux ME, Tiouririne M. The role of the perioperative period in recurrence after cancer surgery. Anesth Analg 2010; 110: 1636-43.
Snyder GL, Greenberg S. Effect of anaesthetic technique and other perioperative factors on cancer recurrence. Br J Anaesth 2010; 105: 106-15.
Salo M. Effects of anaesthesia and surgery on the immune response. Acta Anaesthesiol Scand 1992; 36: 201-20.
Myles PS, Leslie K, McNeil J, Forbes A, Chan MT. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomised controlled trial. Lancet 2004; 363: 1757-63.
Kurata J. Deep hypnosis as a sign of “imbalance” in balanced anesthesia. Anesth Analg 2010; 110: 663-5.
Kheterpal S, Avidan MS. “Triple low” murderer, mediator, or mirror. Anesthesiology 2012; 116: 1176-8.
Bijker JB, van Klei WA, Vergouwe V, et al. Intraoperative hypotension and 1-year mortality after noncardiac surgery. Anesthesiology 2009; 111: 1217-26.
Brady K, Hogue CW. Intraoperative hypotension and patient outcome does “one size fit all?”. Anesthesiology 2013; 119: 495-7.
Walsh M, Devereaux PJ, Garg AX, et al. Relationship between intraoperative mean arterial pressure and clinical outcomes after noncardiac surgery: toward an empirical definition of hypotension. Anesthesiology 2013; 119: 507-15.
Short TG, Leslie K, Chan MT, Campbell D, Frampton C, Myles P. Rationale and design of the balanced anesthesia study: a prospective randomized clinical trial of two levels of anesthetic depth on patient outcome after major surgery. Anesth Analg 2015; . DOI:10.1213/ANE.0000000000000797.
Avidan MS, Zhang L, Burnside BA, et al. Anesthesia awareness and the bispectral index. N Engl J Med 2008; 358: 1097-108.
Leslie K, Myles PS, Chan MT, et al. Nitrous oxide and long-term morbidity and mortality in the ENIGMA trial. Anesth Analg 2011; 112: 387-93.
Monk TG, Weldon BC. Anesthetic depth is a predictor of mortality: It’s time to take the next step. Anesthesiology 2010; 112: 1070-2.
Bruhn J, Bouillon TW, Shafer SL. Bispectral index (BIS) and burst suppression: revealing a part of the BIS algorithm. J Clin Monit Comput 2000; 16: 593-6.
Avidan MS, Jacobsohn E, Glick D, et al. Prevention of intraoperative awareness in a high-risk surgical population. N Engl J Med 2011; 365: 591-600.
Short TG, Leslie K. ‘Known unknowns and unknown unknowns’: electroencephalographic burst suppression and mortality. Br J Anaesth 2014; 113: 897-9.
Besch G, Liu N, Samain E, et al. Occurrence of and risk factors for electroencephalogram burst suppression during propofol-remifentanil anaesthesia. Br J Anaesth 2011; 107: 749-56.
Myles PS. Untangling the triple low: causal inference in anesthesia research. Anesthesiology 2014; 121: 1-3.
Sieber FE, Zakriya KJ, Gottschalk A, et al. Sedation depth during spinal anesthesia and the development of postoperative delirium in elderly patients undergoing hip fracture repair. Mayo Clin Proc 2010; 85: 18-26.
Radtke FM, Franck M, Lendner J, Kruger S, Wernecke KD, Spies CD. Monitoring depth of anaesthesia in a randomized trial decreases the rate of postoperative delirium but not postoperative cognitive dysfunction. Br J Anaesth 2013; 110(Suppl 1): i98-105.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40: 373-83.
Leslie K, Short TG. Sedation depth and mortality: a large randomized trial is required. Anesth Analg 2014; 118: 903-5.
Funding
This work was supported by the New Zealand Health Research Council (12-308-Short), the Australian National Health and Medical Research Council (APP1042727), and the Research Grants Council, Hong Kong Special Administrative Region, China (461513).
Conflicts of interest
Kate Leslie is a chief investigator of the Balanced Anesthesia Study. (Australian and Zealand Clinical Trials Registry No: ACTRN12612000632897). Timothy Short is a chief investigator of the Balanced Anesthesia Study (Australian and New Zealand Clinical Trials Registry No: ACTRN12612000632897).
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is accompanied by an editorial. Please see Can J Anesth 2016; 63: this issue.
Author contributions
Kate Leslie and Timothy Short reviewed the literature and drafted the manuscript.
Rights and permissions
About this article

Cite this article
Leslie, K., Short, T.G. Anesthetic depth and long-term survival: an update. Can J Anesth/J Can Anesth 63, 233–240 (2016). https://doi.org/10.1007/s12630-015-0490-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12630-015-0490-0