
Abstract
Background
Nipple-sparing mastectomy (NSM) is increasingly used in breast cancer patients, as it offers better cosmetic outcomes and improves quality of life. Nipple–areola complex (NAC) involvement must be accurately determined to identify which patients may be candidates for NSM. We aimed to identify the predictors of NAC involvement and develop a clinical predictive model to determine the patients for whom NAC preservation may be considered.
Patients and methods
Patients (n = 168) with primary operable breast cancer who underwent subcutaneous mastectomy for breast reconstruction at Saitama Medical Center from July 2013 to December 2017 were selected from the hospital’s surgical database.
Results
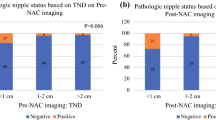
The clinicopathological factors of tumor size ≧ 4 cm (p < 0.001), nipple-to-tumor distance (NTD) < 1 cm by mammography (p = 0.002), NTD < 1 cm by magnetic-resonance imaging (MRI) (p < 0.001), nipple contrast findings by MRI (p < 0.001), tumor in central portion (p < 0.001), multicentric/focal lesion (p < 0.001), and clinical node involvement (p = 0.014) were significantly associated with the presence of NAC involvement. Each predictor was scored 0 or 1. A score of 0–3 points was defined as low risk, 4 points as intermediate risk, and 5–7 points as high risk. Using these classification criteria, NAC involvement rate was determined to be 3.5% in low-risk, 68.7% in intermediate-risk, and 90.0% in high-risk specimens. A significant correlation was observed between the risk group and NAC involvement (p < 0.001).
Conclusion
This nipple–areola complex involvement predictive index can be used to determine the appropriate indication for NSM in breast cancer patients who request NAC preservation with more oncological safety.

Similar content being viewed by others


References
Fisher B, Anderson S, Redmond CK, Wolmark N, Wickerham DL, Cronin WM. Reanalysis and results after 12 years of follow-up in a randomized clinical trial comparing total mastectomy with lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med. 1995;333:1456–61.
Arriagada R, Le MG, Rochard F, Contesso G. Conservative treatment versus mastectomy in early breast cancer: patterns of failure with 15 years of follow-up data. Institut Gustave-Roussy Breast Cancer Group. J Clin Oncol. 1996;14:1558–64.
Kroll SS, Schusterman MA, Tadjalli HE, Singletary SE, Ames FC. Risk of recurrence after treatment of early breast cancer with skin-sparing mastectomy. Ann Surg Oncol. 1997;4:193–7.
Simmons RM, Fish SK, Gayle L, La Trenta GS, Swistel A, Christos P, et al. Local and distant recurrence rates in skin-sparing mastectomies compared with non-skin-sparing mastectomies. Ann Surg Oncol. 1999;6:676–81.
Toth BA, Forley BG, Calabria R. Retrospective study of the skin-sparing mastectomy in breast reconstruction. Plast Reconstr Surg. 1999;104:77–84.
Toth BA, Lappert P. Modified skin incisions for mastectomy: the need for plastic surgical input in preoperative planning. Plast Reconstr Surg. 1991;87:1048–53.
Newman LA, Kuerer HM, Hunt KK, Kroll SS, Ames FC, Ross MI, et al. Presentation, treatment, and outcome of local recurrence afterskin-sparing mastectomy and immediate breast reconstruction. Ann Surg Oncol. 1998;5:620–6.
Slavin SA, Schnitt SJ, Duda RB, Houlihan MJ, Koufman CN, Morris DJ, et al. Skin-sparing mastectomy and immediate reconstruction: oncologic risks and aesthetic results in patients with early-stage breast cancer. Plast Reconstr Surg. 1998;102:49–62.
Kroll SS, Khoo A, Singletary SE, Ames FC, Wang BG, Reece GP, et al. Local recurrence risk after skin-sparing and conventional mastectomy: a 6-year follow-up. Plast Reconstr Surg. 1999;104:421–5.
Petit JY, Veronesi U, Luini A, Orecchia R, Rey PC, Martella S, et al. When mastectomy becomes inevitable: the nipple-sparing approach. Breast. 2005;14:527–31.
Benediktsson KP, Perbeck L. Survival in breast cancer after nipple-sparing subcutaneous mastectomy and immediate reconstruction with implants: a prospective trial with 13 years median follow-up in 216 patients. Eur J Surg Oncol. 2008;34:143–8.
Wellisch DK, Schain WS, Noone RB, Little JW 3rd. The psychological contribution of nipple addition in breast reconstruction. Plast Reconstr Surg. 1987;80:699–704.
Petit JY, Veronesi U, Orecchia R, Rey P, Martella S, Didier F, et al. Nipple sparing mastectomy with nipple areola intraoperative radiotherapy: one thousand and one cases of a five years experience at the European institute of oncology of Milan (EIO). Breast Cancer Res Treat. 2009;117:333–8.
Petit JY, Veronesi U, Rey P, Rotmensz N, Botteri E, Rietjens M, et al. Nipple-sparing mastectomy: risk of nipple-areolar recurrences in a series of 579 cases. Breast Cancer Res Treat. 2009;114:97–101.
Garcia-Etienne CA, Cody Iii HS 3rd, Disa JJ, Cordeiro P, Sacchini V. Nipple-sparing mastectomy: initial experience at the Memorial Sloan-Kettering Cancer Center and a comprehensive review of literature. Breast J. 2009;15:440–9.
Rusby JE, Smith BL, Gui GP. Nipple-sparing mastectomy. Br J Surg. 2010;97:305–16.
Jensen JA, Orringer JS, Giuliano AE. Nipple-sparing mastectomy in 99 patients with a mean follow-up of 5 years. Ann Surg Oncol. 2011;18:1665–70.
Verma GR, Kumar A, Joshi K. Nipple involvement in peripheral breast carcinoma: a prospective study. Indian J Cancer. 1997;34:1–5.
Moon JY, Chang YW, Lee EH, Seo DY. Malignant invasion of the nipple-areolar complex of the breast: usefulness of breast MRI. AJR Am J Roentgenol. 2013;201:448–55.
Byon W, Kim E, Kwon J, Park YL, Park C. Magnetic resonance imaging and clinicopathological factors for the detection of occult nipple involvement in breast cancer patients. J Breast Cancer. 2014;17:386–92.
Karamchandani DM, Chetlen AL, Riley MP, Schetter S, Hollenbeak CS, Mack J. Pathologic-radiologic correlation in evaluation of retroareolar margin in nipple-sparing mastectomy. Virchows Arch. 2015;466:279–87.
Brachtel EF, Rusby JE, Michaelson JS, Chen LL, Muzikansky A, Smith BL, et al. Occult nipple involvement in breast cancer: clinicopathologic findings in 316 consecutive mastectomy specimens. J Clin Oncol. 2009;27:4948–54.
Loewen MJ, Jennings JA, Sherman SR, Slaikeu J, Ebrom PA, Davis AT, et al. Mammographic distance as a predictor of nipple-areola complex involvement in breast cancer. Am J Surg. 2008;195:391–4 (discussion 4–5).
Yamashiro N, Tozaki M, Ogawa T, Kawano N, Suzuki T, Ozaki S, et al. Preoperative MRI marking technique for the planning of breast-conserving surgery. Breast Cancer. 2009;16:223–8.
Schecter AK, Freeman MB, Giri D, Sabo E, Weinzweig J. Applicability of the nipple-areola complex-sparing mastectomy: a prediction model using mammography to estimate risk of nipple-areola complex involvement in breast cancer patients. Ann Plast Surg. 2006;56:498–504 (discussion).
Paepke S, Schmid R, Fleckner S, Paepke D, Niemeyer M, Schmalfeldt B, et al. Subcutaneous mastectomy with conservation of the nipple-areola skin: broadening the indications. Ann Surg. 2009;250:288–92.
Chattopadhyay D, Gupta S, Jash PK, Murmu MB, Gupta S. Skin sparing mastectomy with preservation of nipple areola complex and immediate breast reconstruction in patients with breast cancer: a single centre prospective study. Plast Surg Int. 2014;2014:589068.
Crowe JP Jr, Kim JA, Yetman R, Banbury J, Patrick RJ, Baynes D. Nipple-sparing mastectomy: technique and results of 54 procedures. Arch Surg. 2004;139:148–50.
Luo D, Ha J, Latham B, Ingram D, Connell T, Hastrich D, et al. The accuracy of intraoperative subareolar frozen section in nipple-sparing mastectomies. Ochsner J. 2010;10:188–92.
Kneubil MC, Lohsiriwat V, Curigliano G, Brollo J, Botteri E, Rotmensz N, et al. Risk of locoregional recurrence in patients with false-negative frozen section or close margins of retroareolar specimen in nipple-sparing mastectomy. Ann Surg Oncol. 2012;19:4117–23.
Eisenberg RE, Chan JS, Swistel AJ, Hoda SA. Pathological evaluation of nipple-sparing mastectomies with emphasis on occult nipple involvement: the Weill-Cornell experience with 325 cases. Breast J. 2014;20:15–21.
Duarte GM, Tomazini MV, Oliveira A, Moreira L, Tocchet F, Worschech A, et al. Accuracy of frozen section, imprint cytology, and permanent histology of sub-nipple tissue for predicting occult nipple involvement in patients with breast carcinoma. Breast Cancer Res Treat. 2015;153:557–63.
Morales Piato JR, Aguiar FN, Mota BS, Ricci MD, Doria MT, Alves-Jales RD, et al. Improved frozen section examination of the retroareolar margin for prediction of nipple involvement in breast cancer. Eur J Surg Oncol. 2015;41:986–90.
Ponzone R, Maggiorotto F, Carabalona S, Rivolin A, Pisacane A, Kubatzki F, et al. MRI and intraoperative pathology to predict nipple-areola complex (NAC) involvement in patients undergoing NAC-sparing mastectomy. Eur J Cancer. 2015;51:1882–9.
Alperovich M, Choi M, Karp NS, Singh B, Ayo D, Frey JD, et al. Nipple-sparing mastectomy and sub-areolar biopsy: to freeze or not to freeze? Evaluating the role of sub-areolar intraoperative frozen section. Breast J. 2016;22:18–23.
Chan SE, Liao CY, Wang TY, Chen ST, Chen DR, Lin YJ, et al. The diagnostic utility of preoperative breast magnetic resonance imaging (MRI) and/or intraoperative sub-nipple biopsy in nipple-sparing mastectomy. Eur J Surg Oncol. 2017;43:76–84.
Lambert PA, Kolm P, Perry RR. Parameters that predict nipple involvement in breast cancer. J Am Coll Surg. 2000;191:354–9.
Lagios MD, Gates EA, Westdahl PR, Richards V, Alpert BS. A guide to the frequency of nipple involvement in breast cancer. A study of 149 consecutive mastectomies using a serial subgross and correlated radiographic technique. Am J Surg. 1979;138:135–42.
Morimoto T, Komaki K, Inui K, Umemoto A, Yamamoto H, Harada K, et al. Involvement of nipple and areola in early breast cancer. Cancer. 1985;55:2459–63.
Menon RS, van Geel AN. Cancer of the breast with nipple involvement. Br J Cancer. 1989;59:81–4.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors report no conflicts of interest related to this study.
Ethical approval
This study was approved by the Institutional Review Board of the Saitama Medical Center (IRB no. 18-20).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Seki, H., Sakurai, T., Mizuno, S. et al. A novel nipple–areola complex involvement predictive index for indicating nipple-sparing mastectomy in breast cancer patients. Breast Cancer 26, 808–816 (2019). https://doi.org/10.1007/s12282-019-00987-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12282-019-00987-y