
Abstract
Cord blood (CB) has been an alternative stem cell source for patients with a wide variety of hematological diseases. Cord blood confers the advantages of rapid availability and higher tolerance to two HLA antigen mismatches compared with unrelated donors, and this has increased opportunities for patients who do not have suitable donors or require urgent transplantation. Although the higher rate of engraftment failure remains a serious concern after cord blood transplantation (CBT), the mechanisms underlying this risk have gradually been clarified, which has helped to improve engraftment. Recent studies of CBT and other alternatives have reported comparable outcomes. Moreover, CBT shows promise even when patients are in a non-remission status, which may reflect the potent graft-versus-leukemia effect of CB. Here we compare the most recent outcomes of CBT with those of other stem cell sources and discuss the potential of CB and several outstanding issues that require resolution.
Similar content being viewed by others


Background
Since Gluckman and colleagues achieved the first sibling human leukocyte antigen (HLA)-matched cord blood transplantation (CBT) during 1988 in a pediatric patient with Fanconi anemia [1], cord blood (CB) has gradually become an established source of hematopoietic stem cells for transplantation. Cord blood has several advantages over other stem cell sources, including widespread availability with rapid access, increased tolerance to human leukocyte antigen (HLA) mismatches and a decreased incidence of severe graft-versus-host disease (GVHD). Thus, CBT has provided opportunities for allogeneic hematopoietic stem cell transplantation (Allo-HSCT) to a far wider range of patients who lack suitable HLA-identical siblings or matched unrelated donors within reasonable time periods. Although high rates of engraftment failure and non-relapse mortality (NRM) after CBT have been a serious concern, progress has been significant. Over 40,000 individuals worldwide have been transplanted with CB to date [2]. The annual number of CBT in Japan now exceeds 1,300 and the cumulative number of CBT reached 15,544 in 2017, accounting for almost one-third of the numbers of total CBT performed worldwide. The average body weight for a Japanese person is less than that for Europeans and North Americans, and body weight is a factor that affects the likelihood of finding a suitable CB donor. More European and North American patients have been transplanted with double units (DCBT) and the number of adult recipients of DCBT has surpassed the number of those transplanted with single units since 2005 in Europe [3], whereas almost all CBT in Japan is single CB. Furthermore, the numbers of CBT have recently decreased in Europe and in the USA [2]. This is not apparently due to comparative findings between CBT and other types of stem cell sources, but rather an increase in medical expenses associated with CBT and the expansion of haplo-identical transplants with post-transplant cyclophosphamide (Haplo-PT-CY).
Comparison with other stem cell sources
The outcomes of CBT have never been compared with those of alternative sources in randomized prospective studies. Table 1 shows the major retrospective comparisons of CB with other sources [4,5,6,7,8]. Eapen et al. recently compared CBT with bone marrow transplantation (BMT) or peripheral blood progenitor cell transplantation (PBPCT) matched at the allele levels of HLA-A, -B, -C, and DRB1 from unrelated donors that are generally regarded as the gold standard [6]. A retrospective analysis of data derived from 1,525 patients with acute leukemia (single CBT n = 165; PBPCT n = 888; BMT n = 472) found slower neutrophil recovery in recipients of CBT than PBPCT or BMT. Rates of non-relapse mortality (NRM) were higher after CBT than after 8/8 allele-matched PBPCT (HR 1.62, p < 0.01) or BMT (HR 1.69, p < 0.01), whereas rates of leukemia relapse were similar regardless of the stem cell source. The prevalence of grades 2–4 acute and chronic GVHD was lower in recipients of CBT compared with allele-matched PBPCT (HR, 0.57; p < 0.01 and HR, 0.38; p < 0.01, respectively), whereas rates of chronic, but not acute GVHD, were lower after CBT than after allele-matched BMT. Leukemia-free survival (LFS) after CBT was comparable to 8/8 and 7/8 allele-matched PBPCT or BMT. Atsuta et al. compared data from a Japanese registry of CBT and 8/8 allele-matched unrelated BMT (UBMT), and the outcomes of patients with acute myeloid leukemia (AML) and acute lymphoblastic leukemia (ALL) were separately assessed [7]. In AML patients, CBT recipients showed higher NRM rate and similar relapse rate, resulting in poorer overall and leukemia-free survival rates compared with recipients of UBMT. All these parameters were comparable between CBT and UBMT recipients who had ALL. Terakura et al. more recently analyzed the outcomes for 2,472 adults with acute leukemia who received their first myeloablative transplantation between 2000 and 2010. They compared transplantation outcomes of 8/8 and 7/8 allele-matched UBMT with those of CBT (8/8 UBMT, n = 1,001; 7/8 UBMT,, = 656; CBT, n = 815) [8]. Severe acute GVHD and NRM after UCBT were comparable with 8/8 UBMT, whereas those after 7/8 UBMT were significantly higher. The incidence of extensive chronic GVHD was significantly lower after CBT than 8/8 and 7/8 UBMT. The OS of patients with AML who underwent CBT and 8/8 UBMT was similar, whereas that of 7/8 UBMT was poor. Overall survival did not significantly differ among the three groups with ALL. These findings derived from registry data support the notion that CB can be transplanted into adults with acute leukemia when an HLA-matched unrelated adult donor is unavailable and when a transplant is urgently required.
A CB graft and related donor with HLA 1-antigen mismatch or haplo-match can serve as an alternative to HLA-identical siblings or matched unrelated donors, particularly when the need for transplantation is immediate. Kanda et al. compared the outcomes of a first myeloablative or reduced-intensity transplantation (2288 CBT, 525 RD/1AG-MM-GVH) with single CBT from a related donor with an HLA 1-antigen mismatch in the GVH direction (RD/1AG-MM-GVH) in a national registry of Japanese patients with leukemia or myelodysplastic syndrome (MDS) [9]. The survival rates were comparable between the CBT and RD/1AG-MM-GVH groups and better than that of the RD/1AG-MM-GVH group with an HLA-B mismatch. Neutrophil and platelet engraftment were significantly slower, whereas the incidence of acute or chronic GVHD was significantly lower in the CBT group.
In 2 parallel phase 2 trial of DCBT and Haplo-PT-CY (50 DCBT, 50 Haplo-PT-CY), in which all patients received the same reduced-intensity conditioning (RIC) regimen of fludarabine, cyclophosphamide and 2 Gy of total body irradiation (TBI) (Flu/Cy/TBI), the 1-year disease-free survival (DFS) rates were comparable at 46% and 48%, respectively. The NRM at 1 year was higher, but relapse rates were lower after DCBT than Haplo PT-CY (24% vs. 7%, and 31% vs. 45%, respectively) [10]. Patietns with high risk for relapse may benefit from CBT, while assessment of NRM rsik for each patients and strategies to reduce NRM should be warranted. The ongoing national US randomized comparison of DCBT vs. Haplo PT-CY in RIC patients will be the first prospective comparison of these two graft sources (BMT CTN1101).
Excellent outcomes of CBT exceeding those of other sources have been reported (Table 1). Although studies were from single institutions with relatively few patients [11, 12], the results suggest that CBT has comparable or even greater potential than other approaches and that improvements of clinical outcomes might be possible.
Factors associated with engraftment failure and clinical strategies to overcome this issue
Cell dose is one of the most important factors associated with engraftment. The median numbers of total nucleated cells (TNC) or CD 34+ cells infused from a single CB graft is tenfold less than those infused during adult donor stem cell grafts. Moreover, very few passively transferred T cells that would protect against graft rejection are found in CB grafts. Several studies have associated higher doses of infused TNC with better engraftment [13,14,15,16], and CB units comprising > 2.5–3.0 × 107 TNC/kg are generally recommended to avoid risk of engraftment failure after single CBT. However, engraftment does not fail in all patients who receive CB units containing less than this “threshold”. Nakasone et al. retrospectively analyzed the outcomes of patients listed in a Japanese registry who were transplanted with a single unit of CB containing 0.5–2.5 × 107 TNC/kg [17]. They found that engraftment was more favorable for patients who were transplanted with low TNC and high CD 34+ cells than with high TNC and low CD 34+ cells. Several studies have recognized the importance of the infused dosage of CD 34+ cells [15, 18, 19].
The degree of HLA disparity is also important, but the significance varies among studies. Kurtzberg et al. analyzed data derived from 191 children who received a single CBT in multicenter prospective phase II study and found better neutrophil engraftment in those who received 5 or 6 of 6 matched units than 3 or 4 of 6 (Hazard ratio 1.39, p = 0.04 in multivariate analysis) [20]. Yet, several other studies found no relationship between HLA disparity and engraftment [14, 21]. Atsuta et al. investigated the effect of HLA disparity on the outcomes of single CBT in 498 pediatric and 1,800 adult patients in Japan [22]. They also found no correlation between HLA disparity and neutrophil engraftment in either group, although more mismatched HLA loci correlated with increased risk of NRM in the pediatric patients. Barker et al. retrospectively analyzed the combined effects of TNC and HLA match on the outcomes of 1,061 adult and pediatric CBT recipients with leukemia or myelodysplasia [23]. They found that TNC dose and HLA mismatch were independent predictors of engraftment, NRM or OS. A greater HLA mismatch resulted in a notably greater importance of TNC to engraftment and OS. For example, units that were 4/6 HLA-matched to recipients required TNC > 5.0 × 107/kg to achieve a similar NRM to that of 5/6 units with TNC > 2.5 × 107/kg. These findings suggest that a better HLA match could compensate for a lower dose of TNC.
Finding donor-specific anti-HLA antibodies (DSA) in recipients is associated with poor engraftment. A retrospective analysis of myeloablative single-unit CBT by Takanashi et al. found that engraftment was achieved in 32% and 83% of 386 patients with and without DSA, respectively [24]. The notion has been suggested that unrecognized DSA against HLA-C, -DP, -DQ or DRB3/4/5 antigens, which are not routinely typed in CB grafting, adversely affect engraftment in HLA-mismatched CBT [25]. HLA typing at these loci or cytotoxic crossmatch tests before transplantation might help to avoid transplantation with CB units that have unrecognized DSA. However, these methods have not yet been fully evaluated in the setting of CBT.
Conditioning regimens are more crucial to achieve successful engraftment in CBT compared with others sources. In a study of the outcomes of 10 adult patients who underwent DCBT with fludarabine plus a myeloablative dose of intravenous busulfan (Flu/Bu4) regimen at Duke University found that only 2 of 10 patients became engrafted with donor hematopoietic cells [26]. Considering that the FluBu4 regimen has been widely applied to allogeneic BMT or PBPCT without an increase in the incidence of engraftment failure [27, 28], more intensive immune suppression before transplantation seems crucial to ensure CB engraftment. Nakasone et al. retrospectively analyzed the impact of TBI on neutrophil engraftment in 1,464 adult recipients of CBT using registry data [29] and found that TBI significantly and favorably affected engraftment in both myeloablative conditioning (MAC) and RIC groups. Conversely, Yamamoto et al. recently investigated the novel non-TBI regimen of Flu/Bu4 + Mel regimen that was expected to increase lymphoablative and myeloablative effects. They found better engraftment and survival rates even in patients with myeloid malignancies not in remission [30].
Strategies to increase the infused cell dose and possibly improve outcomes have included DCBT. Brunstein et al. retrospectively reviewed the outcomes of 110 patients with high-risk hematological malignancies who underwent single or double CBT after the RIC regimen [31]. The targeted TNC dose was set at 3.0 × 107/kg, and patients were to receive DCBT when a single unit contained fewer cells. Overall rates of engraftment (94% vs. 91%), overall survival and NRM did not significantly differ between single vs. double. Relapse rates were notably lower in the DCBT, than the single group (30% vs. 41% p = 0.07), whereas the incidence of acute GVHD tended to be higher in the DCBT group. Although DCBT has become popular due to the relatively larger body weight of North American and European populations, randomized single and double CBT data have never been compared in adult patients. A randomized phase III clinical comparison of single and double CBT of 224 pediatric patients found no significant differences after single and double CBT between overall rates of engraftment (89% vs. 88%), relapse rates at 1 year (12% vs. 14%), NRM at one year (19% vs. 22%), or disease-free survival (70% vs. 64%) [32]. Presently, the use of double units is justifiable only when one unit does not contain enough TNC [33].
Early immune reactions after CBT and GVHD prophylaxis
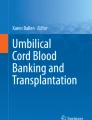
Because CB contains immature immune cells, it is thought to be less active in inducing allogeneic immune reactions than other sources of stem cells. However, several studies including ours have identified a unique clinical manifestation characterized by non-infectious high-grade fever, skin eruption, diarrhea, jaundice, and body weight gain soon after CBT [34,35,36,37,38,39,40,41] (Table 2). The onset occurred around post-transplant day 9, and it has been termed pre-engraftment immune reactions (PIR) or pre-engraftment syndrome (PES). The incidence of PIR ranged from 20 to 78% in various studies, probably because of different definitions, or different transplant procedures with respect to conditioning regimens or GVHD prophylaxis (Table 2). The clinical significance of PIR on transplant outcomes has been controversial. In early studies from us where preparative regimen without anti-thymocyte globulin (ATG) coupled with calcineurin inhibitor (CI) alone as GVHD prophylaxis was mainly used [42, 43], PIR itself sometimes induced severe organ failure including pulmonary complications or hemophagocytic syndrome (HPS), defined as severe PIR, and it has increased the incidence of early NRM among elderly patients. HPS might be a unique and characteristic manifestation after CBT, considering that it has been regarded as a rare complication after BMT or PBPCT. Takagi et al. retrospectively analyzed the outcomes of 119 patients who underwent RIC-CBT and received less intensive GVHD prophylaxis. Twenty patients had HPS, mostly with donor-dominant chimerism, and 14 of them eventually failed engraftment due to the development of HPS [44]. We also reported that HLA disparity in the direction of GVH, but not HVG, adversely affected engraftment kinetics when single CI was administered for GVHD prophylaxis [16]. A novel mechanism of engraftment failure proposed based on these findings was that excessive immune reactions of donor cells result in engraftment failure through the development of HPS after CBT. We also found that the incidence of HPS was significantly higher among patients with severe PIR than without PIR [45]. Thus, PIR and HPS closely correlate and could be considered as post-transplant cytokine-storm syndrome, which can occur after HLA-mismatched transplantation. The mechanisms underlying PIR or HPS have not been clarified. Serum values for inflammatory cytokines such as IL-6 or IL-5, are elevated around the time of PIR onset [46, 47]. We previously showed that rapid T cell chimerism switches to the donor type, and phenotypic conversion from naïve to memory T cells are significantly associated with the development of PIR [48]. Gutman et al. also reported that CD8+ T cells predominately expressed effector memory or effector phenotype and produced IFN-γ in response only to non-engrafted units early after double-unit CBT, reflecting a specific immune response of the dominant, against the non-engrafted units [49]. Donor T cell activation possibly via mismatched HLA could cause inflammatory cytokine secretion and such excessive allogeneic immune reactions will activate macrophages to develop phagocytosis, which will finally cause engraftment failure. Figure 1 shows a schema of HPS development. Contrary to previous notions, CB naïve T cells have powerful proliferative potential to act against allogenic antigens very soon after CBT, which would be the main mechanism behind early immune-related events.

Schema of HPS development. Donor-derived CTL possibly activated by mismatched host HLA lead to release of various inflammatory cytokines that in turn induce macrophage activation in BM accompanied by downregulated CD47 expression on HSC causing them to become vulnerable to phagocytosis. Mycophenolate mofetil might suppress activated CTL and reduce incidence of HPS. BM bone marrow, CTL cytotoxic T lymphocytes, HPS hemophagocytic syndrome, HSC hematopoietic stem cells
Since immune cells in CB units have the conflicting features of immunological immaturity and potential for hyperimmune reactions, and since both directly impact engraftment, GVHD prophylaxis is critical to achieve engraftment. Combining CI with other immuno suppressive agents, including mycophenolate mofetil (MMF), corticosteroids, methotrexate (MTX), sirolimus and ATG have been explored as GVHD prophylaxis in the setting of CBT. Uchida et al. conducted a matched-pair comparison of tacrolimus (TAC) + MMF vs. TAC regimens for GVHD prophylaxis, to determine the effects of MMF. Although the total incidences of any PIR were comparable between TAC + MMF and TAC, the incidences of severe PIR and HPS were significantly decreased in TAC + MMF group, resulting in lower NRM before engraftment and higher engraftment rates for TAC + MMF compared with TAC (90% vs. 66%, p < 0.05) [41]. Combinations of CI and MMF have been applied worldwide [50]. However, only an oral formulation is available in Japan, which raises the concern that the effect might differ among individuals due to variations in bioavailability. Therapeutic drug monitoring of MMF might further improve outcomes [51]. Adding MTX to CI reportedly reduces the incidence of PIR and severe acute GVHD [35, 52], and this has been widely applied in Japan. However, this method is accompanied by the risk of graft rejection and engraftment delay, especially in the RIC setting, possibly due to excessive immunosuppression and the cytotoxic effect of MTX. Reducing the dose of MTX in GVHD prophylaxis has recently been investigated [53]. A retrospective comparison of MMF vs. MTX by Terakura using Japanese registry data [52] showed better engraftment after GVHD prophylaxis using MMF, whereas MTX reduced the incidence or severity of acute GVHD. ATG might also be an alternative strategy for GVHD prophylaxis in terms of reduced incidence of PIR and severe GVHD [37, 54], but this strategy also has various disadvantages including delayed immune recovery, risk of infection or post transplantation lymphoproliferative disorder, and an increased incidence of relapse [55,56,57]. In particular, administering ATG to patients with high-risk malignancies seems highly controversial due to an increased incidence of relapse [58]. Additionally, ATG has a long half-life and multiple factors affect its biological activities, which renders its impact on clinical outcomes highly variable according to the dose, timing of administration, and the status of patients.
Comparable or even more potent GVL effect after CBT, and CBT for patients with high-risk malignancies
Considering that CB grafts contain T cells with an immunologically naïve phenotype, concerns have been raised regarding the capacity of CB-derived lymphocytes to mediate sufficient graft-versus-leukemia (GVL) effects. However, the incidence of relapse after CBT is comparable to that after BMT or PBPCT (Table 1). Moreover, several studies have shown a decreased relapse rate with CBT despite a lower incidence of GVHD. Brunstein et al. found that recipients of myeloablative DCBT had significantly lower rates of relapse at 5 years compared with recipients of matched-related, matched-unrelated (MUD), and mismatched-unrelated (MMUD) donors (15% vs. 43, 37 and 35%, respectively) [59]. Milano et al. analyzed the outcomes of 582 patients at Fred Hutchinson Cancer Research Center who received a first myeloablative allo-HSCT using CB (n = 140), MUD (n = 344), or MMUD (n = 98) donors [12]. They found that the risk of relapse was significantly lower in the CB, than in the group of patients with minimal residual disease transplanted with HSC from unrelated donors. Overall survival was also significantly better for those who received CBT than after MMUD transplantation. Kanda et al. analyzed the impact of acute and chronic GVHD on outcomes in adult patients with acute leukemia or myelodysplastic syndrome who underwent their first CBT (n = 2558) and found that mild acute or chronic GVHD was associated not only with a low risk of relapse but also with a low risk of non-relapse mortality, and provides a survival benefit in UCBT [60]. This effect was not generally observed in other stem cell sources, indicating the unique immunological potential after CBT. The high potential of a GVL effect after CBT has not been clearly explained. The increased level of HLA mismatches or the powerful proliferative potential of CB-derived lymphocytes, as described in developing PIR, could explain the low risk of relapse associated with CBT. A recent report has described that an HLA-DPB1 mismatch induces a GVL effect without developing severe GVHD after single CBT [61].
Patients with advanced disease who need urgent transplantation frequently receive CB grafts because they are rapidly accessible and widely available. This might be associated with the high prevalence of CBT. Although the prognosis of allo-HSCT for advanced hematological malignancies is dismal due to increased risk of relapse regardless of the donor source, the outcomes of CBT with intensified conditioning regimens are encouraging (Table 3). Investigators at the Institute of Medical Science, University of Tokyo have performed single CBT using G-CSF plus high-dose cytarabine (Ara-C) and CY/TBI and the OS at 7 years is 61.4% in patients with myeloid malignancies not in remission [62]. A Spanish group analyzed the outcomes of 49 adults with high-risk AML who underwent single CBT after a MAC regimen consisting of thiotepa, Bu, Flu, and ATG. The leukemia-free survival (LFS) rate at 2 years was 42%, although high NRM due to infections was problematic [63]. A Chinese group also reported successful outcomes in non-remission patients with DFS at 2 years of 40.3% using intensified MAC regimens [64]. A Flu/Cy/TBI 2 Gy regimen has been applied worldwide in the setting of RIC-CBT [50, 65]. However, disease relapse has been a major issue probably due to the low intensity of the regimen [66]. Ponce et al. intensified the regimen by adding thiotepa and increasing the TBI dose to 4 Gy; the 2-year DFS was 60%, although many patients with CR were included [67]. We applied a novel reduced-toxicity MAC regimen by adding Mel to the Flu/Bu4 regimen for single CBT in a relatively older population with myeloid malignancies not in remission. This non-TBI regimen provided durable engraftment and remission with acceptable NRM and 54.9% survival with DFS at 2 years [30].
Taken together, the potential GVL effect of CB combined with novel conditioning regimens and the availability of CB grafts, has improved the outcomes of patients with high-risk hematological malignancies that have historically been difficult to cure.
Conclusion
During the three decades since the first CBT in France, much progress has been made, and CB has become an alternative graft chosen equally with other donors in Japan. Recently, even strong GVL effect of CB grafts despite a low incidence of severe GVHD has been suggested. Although the high engraftment failure rate and associated high NRM remain to be resolved, CB will continue to be an important stem cell source for transplantation in the future, and hopefully, there is even a chance for CB to become the graft of first priority over the others once the problems were overcome, given the obvious advantages of CB such as rapid and wide availability for many transplant candidates.
References
Gluckman E, Broxmeyer HA, Auerbach AD, Friedman HS, Douglas GW, Devergie A, et al. Hematopoietic reconstitution in a patient with Fanconi’s anemia by means of umbilical-cord blood from an HLA-identical sibling. N Engl J Med. 1989;321(17):1174–8.
Niederwieser D, Baldomero H, Szer J, Gratwohl M, Aljurf M, Atsuta Y, et al. Hematopoietic stem cell transplantation activity worldwide in 2012 and a SWOT analysis of the Worldwide Network for Blood and Marrow Transplantation Group including the global survey. Bone Marrow Transplant. 2016;51(6):778–85.
Passweg JR, Baldomero H, Bader P, Basak GW, Bonini C, Duarte R, et al. Is the use of unrelated donor transplantation leveling off in Europe? The 2016 European Society for Blood and Marrow Transplant activity survey report. Bone Marrow Transplant. 2018;53(9):1139–48.
Laughlin MJ, Eapen M, Rubinstein P, Wagner JE, Zhang MJ, Champlin RE, et al. Outcomes after transplantation of cord blood or bone marrow from unrelated donors in adults with leukemia. N Engl J Med. 2004;351(22):2265–75.
Rocha V, Labopin M, Sanz G, Arcese W, Schwerdtfeger R, Bosi A, et al. Transplants of umbilical-cord blood or bone marrow from unrelated donors in adults with acute leukemia. N Engl J Med. 2004;351(22):2276–85.
Eapen M, Rocha V, Sanz G, Scaradavou A, Zhang MJ, Arcese W, et al. Effect of graft source on unrelated donor haemopoietic stem-cell transplantation in adults with acute leukaemia: a retrospective analysis. Lancet Oncol. 2010;11(7):653–60.
Atsuta Y, Suzuki R, Nagamura-Inoue T, Taniguchi S, Takahashi S, Kai S, et al. Disease-specific analyses of unrelated cord blood transplantation compared with unrelated bone marrow transplantation in adult patients with acute leukemia. Blood. 2009;113(8):1631–8.
Terakura S, Atsuta Y, Tsukada N, Kobayashi T, Tanaka M, Kanda J, et al. Comparison of outcomes of 8/8 and 7/8 allele-matched unrelated bone marrow transplantation and single-unit Cord blood transplantation in adults with acute leukemia. Biol Blood Marrow Transplant. 2016;22(2):330–8.
Kanda J, Ichinohe T, Kato S, Uchida N, Terakura S, Fukuda T, et al. Unrelated cord blood transplantation vs related transplantation with HLA 1-antigen mismatch in the graft-versus-host direction. Leukemia. 2013;27(2):286–94.
Brunstein CG, Fuchs EJ, Carter SL, Karanes C, Costa LJ, Wu J, et al. Alternative donor transplantation after reduced intensity conditioning: results of parallel phase 2 trials using partially HLA-mismatched related bone marrow or unrelated double umbilical cord blood grafts. Blood. 2011;118(2):282–8.
Takahashi S, Iseki T, Ooi J, Tomonari A, Takasugi K, Shimohakamada Y, et al. Single-institute comparative analysis of unrelated bone marrow transplantation and cord blood transplantation for adult patients with hematologic malignancies. Blood. 2004;104(12):3813–20.
Milano F, Gooley T, Wood B, Woolfrey A, Flowers ME, Doney K, et al. Cord-blood transplantation in patients with minimal residual disease. N Engl J Med. 2016;375(10):944–53.
Rubinstein P, Carrier C, Scaradavou A, Kurtzberg J, Adamson J, Migliaccio AR, et al. Outcomes among 562 recipients of placental-blood transplants from unrelated donors. N Engl J Med. 1998;339(22):1565–77.
Laughlin MJ, Barker J, Bambach B, Koc ON, Rizzieri DA, Wagner JE, et al. Hematopoietic engraftment and survival in adult recipients of umbilical-cord blood from unrelated donors. N Engl J Med. 2001;344(24):1815–22.
Wagner JE, Barker JN, DeFor TE, Baker KS, Blazar BR, Eide C, et al. Transplantation of unrelated donor umbilical cord blood in 102 patients with malignant and nonmalignant diseases: influence of CD34 cell dose and HLA disparity on treatment-related mortality and survival. Blood. 2002;100(5):1611–8.
Matsuno N, Wake A, Uchida N, Ishiwata K, Araoka H, Takagi S, et al. Impact of HLA disparity in the graft-versus-host direction on engraftment in adult patients receiving reduced-intensity cord blood transplantation. Blood. 2009;114(8):1689–95.
Nakasone H, Tabuchi K, Uchida N, Ohno Y, Matsuhashi Y, Takahashi S, et al. Which is more important for the selection of cord blood units for haematopoietic cell transplantation: the number of CD34-positive cells or total nucleated cells? Br J Haematol. 2019;185(1):166–9.
Terakura S, Azuma E, Murata M, Kumamoto T, Hirayama M, Atsuta Y, et al. Hematopoietic engraftment in recipients of unrelated donor umbilical cord blood is affected by the CD34+ and CD8+ cell doses. Biol Blood Marrow Transplant. 2007;13(7):822–30.
Konuma T, Kato S, Oiwa-Monna M, Tanoue S, Ogawa M, Isobe M, et al. Cryopreserved CD34(+) cell dose, but not total nucleated cell dose, influences hematopoietic recovery and extensive chronic graft-versus-host disease after single-unit cord blood transplantation in adult patients. Biol Blood Marrow Transplant. 2017;23(7):1142–50.
Kurtzberg J, Prasad VK, Carter SL, Wagner JE, Baxter-Lowe LA, Wall D, et al. Results of the Cord Blood Transplantation Study (COBLT): clinical outcomes of unrelated donor umbilical cord blood transplantation in pediatric patients with hematologic malignancies. Blood. 2008;112(10):4318–27.
Arcese W, Rocha V, Labopin M, Sanz G, Iori AP, de Lima M, et al. Unrelated cord blood transplants in adults with hematologic malignancies. Haematologica. 2006;91(2):223–30.
Atsuta Y, Kanda J, Takanashi M, Morishima Y, Taniguchi S, Takahashi S, et al. Different effects of HLA disparity on transplant outcomes after single-unit cord blood transplantation between pediatric and adult patients with leukemia. Haematologica. 2013;98(5):814–22.
Barker JN, Scaradavou A, Stevens CE. Combined effect of total nucleated cell dose and HLA match on transplantation outcome in 1061 cord blood recipients with hematologic malignancies. Blood. 2010;115(9):1843–9.
Takanashi M, Atsuta Y, Fujiwara K, Kodo H, Kai S, Sato H, et al. The impact of anti-HLA antibodies on unrelated cord blood transplantations. Blood. 2010;116(15):2839–46.
Yamamoto H, Uchida N, Matsuno N, Ota H, Kageyama K, Wada S, et al. Anti-HLA antibodies other than against HLA-A, -B, -DRB1 adversely affect engraftment and nonrelapse mortality in HLA-mismatched single cord blood transplantation: possible implications of unrecognized donor-specific antibodies. Biol Blood Marrow Transplant. 2014;20(10):1634–40.
Horwitz ME, Morris A, Gasparetto C, Sullivan K, Long G, Chute J, et al. Myeloablative intravenous busulfan/fludarabine conditioning does not facilitate reliable engraftment of dual umbilical cord blood grafts in adult recipients. Biol Blood Marrow Transplant. 2008;14(5):591–4.
Russell JA, Tran HT, Quinlan D, Chaudhry A, Duggan P, Brown C, et al. Once-daily intravenous busulfan given with fludarabine as conditioning for allogeneic stem cell transplantation: study of pharmacokinetics and early clinical outcomes. Biol Blood Marrow Transplant. 2002;8(9):468–76.
de Lima M, Couriel D, Thall PF, Wang X, Madden T, Jones R, et al. Once-daily intravenous busulfan and fludarabine: clinical and pharmacokinetic results of a myeloablative, reduced-toxicity conditioning regimen for allogeneic stem cell transplantation in AML and MDS. Blood. 2004;104(3):857–64.
Nakasone H, Fuji S, Yakushijin K, Onizuka M, Shinohara A, Ohashi K, et al. Impact of total body irradiation on successful neutrophil engraftment in unrelated bone marrow or cord blood transplantation. Am J Hematol. 2017;92(2):171–8.
Yamamoto H, Uchida N, Yuasa M, Kageyama K, Ota H, Kaji D, et al. A novel reduced-toxicity myeloablative conditioning regimen using full-dose busulfan, fludarabine, and melphalan for single cord blood transplantation provides durable engraftment and remission in nonremission myeloid malignancies. Biol Blood Marrow Transplant. 2016;22(10):1844–50.
Brunstein CG, Barker JN, Weisdorf DJ, DeFor TE, Miller JS, Blazar BR, et al. Umbilical cord blood transplantation after nonmyeloablative conditioning: impact on transplantation outcomes in 110 adults with hematologic disease. Blood. 2007;110(8):3064–70.
Wagner JE Jr, Eapen M, Carter S, Wang Y, Schultz KR, Wall DA, et al. One-unit versus two-unit cord-blood transplantation for hematologic cancers. N Engl J Med. 2014;371(18):1685–94.
Bhella S, Majhail NS, Betcher J, Costa LJ, Daly A, Dandoy CE, et al. Choosing wisely BMT: American Society for Blood and Marrow Transplantation and Canadian Blood and Marrow Transplant Group’s List of 5 tests and treatments to question in blood and marrow transplantation. Biol Blood Marrow Transplant. 2018;24(5):909–13.
Kishi Y, Kami M, Miyakoshi S, Kanda Y, Murashige N, Teshima T, et al. Early immune reaction after reduced-intensity cord-blood transplantation for adult patients. Transplantation. 2005;80(1):34–40.
Narimatsu H, Terakura S, Matsuo K, Oba T, Uchida T, Iida H, et al. Short-term methotrexate could reduce early immune reactions and improve outcomes in umbilical cord blood transplantation for adults. Bone Marrow Transplant. 2007;39(1):31–9.
Patel KJ, Rice RD, Hawke R, Abboud M, Heller G, Scaradavou A, et al. Pre-engraftment syndrome after double-unit cord blood transplantation: a distinct syndrome not associated with acute graft-versus-host disease. Biol Blood Marrow Transplant. 2010;16(3):435–40.
Frangoul H, Wang L, Harrell FE Jr, Ho R, Domm J. Preengraftment syndrome after unrelated cord blood transplant is a strong predictor of acute and chronic graft-versus-host disease. Biol Blood Marrow Transplant. 2009;15(11):1485–8.
Wang X, Liu H, Li L, Geng L, Ding K, Liu X, et al. Pre-engraftment syndrome after unrelated donor umbilical cord blood transplantation in patients with hematologic malignancies. Eur J Haematol. 2012;88(1):39–45.
Park M, Lee SH, Lee YH, Yoo KH, Sung KW, Koo HH, et al. Pre-engraftment syndrome after unrelated cord blood transplantation: a predictor of engraftment and acute graft-versus-host disease. Biol Blood Marrow Transplant. 2013;19(4):640–6.
Kanda J, Kaynar L, Kanda Y, Prasad VK, Parikh SH, Lan L, et al. Pre-engraftment syndrome after myeloablative dual umbilical cord blood transplantation: risk factors and response to treatment. Bone Marrow Transplant. 2013;48(7):926–31.
Uchida N, Wake A, Nakano N, Ishiwata K, Takagi S, Tsuji M, et al. Mycophenolate and tacrolimus for graft-versus-host disease prophylaxis for elderly after cord blood transplantation: a matched pair comparison with tacrolimus alone. Transplantation. 2011;92(3):366–71.
Miyakoshi S, Yuji K, Kami M, Kusumi E, Kishi Y, Kobayashi K, et al. Successful engraftment after reduced-intensity umbilical cord blood transplantation for adult patients with advanced hematological diseases. Clin Cancer Res. 2004;10(11):3586–92.
Uchida N, Wake A, Takagi S, Yamamoto H, Kato D, Matsuhashi Y, et al. Umbilical cord blood transplantation after reduced-intensity conditioning for elderly patients with hematologic diseases. Biol Blood Marrow Transplant. 2008;14(5):583–90.
Takagi S, Masuoka K, Uchida N, Ishiwata K, Araoka H, Tsuji M, et al. High incidence of haemophagocytic syndrome following umbilical cord blood transplantation for adults. Br J Haematol. 2009;147(4):543–53.
Yamamoto H. Hemophagocytic syndrome early after reduced-intensity cord blood transplantation. The 35th annual meeting of the Japan Society for Hematopoietic Cell Transplantation, Kanazawa. 2013.
Konuma T, Kohara C, Watanabe E, Mizukami M, Nagai E, Oiwa-Monna M, et al. Cytokine profiles of pre-engraftment syndrome after single-unit cord blood transplantation for adult patients. Biol Blood Marrow Transplant. 2017;23(11):1932–8.
Ogata M, Satou T, Kawano R, Takakura S, Goto K, Ikewaki J, et al. Correlations of HHV-6 viral load and plasma IL-6 concentration with HHV-6 encephalitis in allogeneic stem cell transplant recipients. Bone Marrow Transplant. 2010;45(1):129–36.
Matsuno N, Yamamoto H, Watanabe N, Uchida N, Ota H, Nishida A, et al. Rapid T-cell chimerism switch and memory T cell expansion are associated with pre-engraftment immune reaction early after cord blood transplantation. Br J Haematol. 2013;160(2):255–8.
Gutman JA, Turtle CJ, Manley TJ, Heimfeld S, Bernstein ID, Riddell SR, et al. Single-unit dominance after double-unit umbilical cord blood transplantation coincides with a specific CD8+ T cell response against the nonengrafted unit. Blood. 2010;115(4):757–65.
Barker JN, Kurtzberg J, Ballen K, Boo M, Brunstein C, Cutler C, et al. Optimal practices in unrelated donor cord blood transplantation for hematologic malignancies. Biol Blood Marrow Transplant. 2017;23(6):882–96.
Arai Y, Kondo T, Kitano T, Hishizawa M, Yamashita K, Kadowaki N, et al. Monitoring mycophenolate mofetil is necessary for the effective prophylaxis of acute GVHD after cord blood transplantation. Bone Marrow Transplant. 2015;50(2):312–4.
Terakura S, Kuwatsuka Y, Yamasaki S, Wake A, Kanda J, Inamoto Y, et al. GvHD prophylaxis after single-unit reduced intensity conditioning cord blood transplantation in adults with acute leukemia. Bone Marrow Transplant. 2017;52(9):1261–7.
Saito B, Hattori N, Yamamoto K, Arai N, Kawaguchi Y, Fujiwara S, et al. Umbilical cord blood transplantation for adults using tacrolimus with two-day very-short-term methotrexate for graft-versus-host disease prophylaxis. Leuk Res. 2016;47:161–5.
Ponce DM, Eapen M, Sparapani R, O’Brien TA, Chan KW, Chen J, et al. In vivo T cell depletion with myeloablative regimens on outcomes after cord blood transplantation for acute lymphoblastic leukemia in children. Biol Blood Marrow Transplant. 2015;21(12):2173–9.
Brunstein CG, Weisdorf DJ, DeFor T, Barker JN, Tolar J, van Burik JA, et al. Marked increased risk of Epstein–Barr virus-related complications with the addition of antithymocyte globulin to a nonmyeloablative conditioning prior to unrelated umbilical cord blood transplantation. Blood. 2006;108(8):2874–80.
Pascal L, Mohty M, Ruggeri A, Tucunduva L, Milpied N, Chevallier P, et al. Impact of rabbit ATG-containing myeloablative conditioning regimens on the outcome of patients undergoing unrelated single-unit cord blood transplantation for hematological malignancies. Bone Marrow Transplant. 2015;50(1):45–50.
Pascal L, Tucunduva L, Ruggeri A, Blaise D, Ceballos P, Chevallier P, et al. Impact of ATG-containing reduced-intensity conditioning after single- or double-unit allogeneic cord blood transplantation. Blood. 2015;126(8):1027–32.
Zheng C, Luan Z, Fang J, Sun X, Chen J, Li CK, et al. Comparison of conditioning regimens with or without antithymocyte globulin for unrelated cord blood transplantation in children with high-risk or advanced hematological malignancies. Biol Blood Marrow Transplant. 2015;21(4):707–12.
Brunstein CG, Gutman JA, Weisdorf DJ, Woolfrey AE, Defor TE, Gooley TA, et al. Allogeneic hematopoietic cell transplantation for hematologic malignancy: relative risks and benefits of double umbilical cord blood. Blood. 2010;116(22):4693–9.
Kanda J, Morishima Y, Terakura S, Wake A, Uchida N, Takahashi S, et al. Impact of graft-versus-host disease on outcomes after unrelated cord blood transplantation. Leukemia. 2017;31(3):663–8.
Yabe T, Azuma F, Kashiwase K, Matsumoto K, Orihara T, Yabe H, et al. HLA-DPB1 mismatch induces a graft-versus-leukemia effect without severe acute GVHD after single-unit umbilical cord blood transplantation. Leukemia. 2018;32(1):168–75.
Konuma T, Kato S, Ooi J, Oiwa-Monna M, Ebihara Y, Mochizuki S, et al. Single-unit cord blood transplantation after granulocyte colony-stimulating factor-combined myeloablative conditioning for myeloid malignancies not in remission. Biol Blood Marrow Transplant. 2014;20(3):396–401.
Sanz J, Boluda JC, Martin C, Gonzalez M, Ferra C, Serrano D, et al. Single-unit umbilical cord blood transplantation from unrelated donors in patients with hematological malignancy using busulfan, thiotepa, fludarabine and ATG as myeloablative conditioning regimen. Bone Marrow Transplant. 2012;47(10):1287–93.
Yao W, Zheng CC, Liu HL, Geng LQ, Tang BL, Tong J, et al. Salvaged single-unit cord blood transplantation for 26 patients with hematologic malignancies not in remission. Braz J Med Biol Res. 2015;48(10):871–6.
Shaw BE, Veys P, Pagliuca A, Addada J, Cook G, Craddock CF, et al. Recommendations for a standard UK approach to incorporating umbilical cord blood into clinical transplantation practice: conditioning protocols and donor selection algorithms. Bone Marrow Transplant. 2009;44(1):7–12.
Oran B, Wagner JE, DeFor TE, Weisdorf DJ, Brunstein CG. Effect of conditioning regimen intensity on acute myeloid leukemia outcomes after umbilical cord blood transplantation. Biol Blood Marrow Transplant. 2011;17(9):1327–34.
Ponce DM, Sauter C, Devlin S, Lubin M, Gonzales AM, Kernan NA, et al. A novel reduced-intensity conditioning regimen induces a high incidence of sustained donor-derived neutrophil and platelet engraftment after double-unit cord blood transplantation. Biol Blood Marrow Transplant. 2013;19(5):799–803.
Acknowledgements
The valuable contributions of Naoyuki Uchida (Toranomon Hospital) and Shuichi Taniguchi (Toranomon Hospital) are sincerely appreciated.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors have no conflicts of interest to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
About this article

Cite this article
Yamamoto, H. Single cord blood transplantation in Japan; expanding the possibilities of CBT. Int J Hematol 110, 39–49 (2019). https://doi.org/10.1007/s12185-019-02672-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12185-019-02672-4