
Abstract
Background
In acute brain injury (ABI), the effects of hypoxemia as a potential cause of secondary brain damage and poor outcome are well documented, whereas the impact of hyperoxemia is unclear. The primary aim of this study was to assess the episodes of hypoxemia and hyperoxemia in patients with ABI during the intensive care unit (ICU) stay and to determine their association with in-hospital mortality. The secondary aim was to identify the optimal thresholds of arterial partial pressure of oxygen (PaO2) predicting in-hospital mortality.
Methods
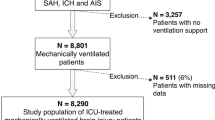
We conducted a secondary analysis of a prospective multicenter observational cohort study. Adult patients with ABI (traumatic brain injury, subarachnoid aneurysmal hemorrhage, intracranial hemorrhage, ischemic stroke) with available data on PaO2 during the ICU stay were included. Hypoxemia was defined as PaO2 < 80 mm Hg, normoxemia was defined as PaO2 between 80 and 120 mm Hg, mild/moderate hyperoxemia was defined as PaO2 between 121 and 299 mm Hg, and severe hyperoxemia was defined as PaO2 levels ≥ 300 mm Hg.
Results
A total of 1,407 patients were included in this study. The mean age was 52 (±18) years, and 929 (66%) were male. Over the ICU stay, the fractions of patients in the study cohort who had at least one episode of hypoxemia, mild/moderate hyperoxemia, and severe hyperoxemia were 31.3%, 53.0%, and 1.7%, respectively. PaO2 values below 92 mm Hg and above 156 mm Hg were associated with an increased probability of in-hospital mortality. Differences were observed among subgroups of patients with ABI, with consistent effects only seen in patients without traumatic brain injury.
Conclusions
In patients with ABI, hypoxemia and mild/moderate hyperoxemia were relatively frequent. Hypoxemia and hyperoxemia during ICU stay may influence in-hospital mortality. However, the small number of oxygen values collected represents a major limitation of the study.





Similar content being viewed by others


Data Availability
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Cumpstey AF, Oldman AH, Martin DS, Smith A, Grocott MPW. Oxygen targets during mechanical ventilation in the ICU: a systematic review and meta-analysis. Crit Care Explor. 2022;4: e0652.
Young PJ, Hodgson CL, Rasmussen BS. Oxygen targets. Intensive Care Med. 2022;48:732–5.
Lång M, Raj R, Skrifvars MB, Koivisto T, Lehto H, Kivisaari R, et al. Early moderate hyperoxemia does not predict outcome after aneurysmal subarachnoid hemorrhage. Neurosurgery. 2016;78:540–5.
Young P, Beasley R, Bailey M, Bellomo R, Eastwood GM, Nichol A, et al. The association between early arterial oxygenation and mortality in ventilated patients with acute ischaemic stroke. Crit Care Resusc. 2012;14:14–9.
ÓBriain D, Nickson C, Pilcher DV, Udy AA. Early hyperoxia in patients with traumatic brain injury admitted to intensive care in Australia and New Zealand: A retrospective multicenter cohort study. Neurocrit Care. 2018;29:443–51.
Weeden M, Bailey M, Gabbe B, Pilcher D, Bellomo R, Udy A. Functional outcomes in patients admitted to the intensive care unit with traumatic brain injury and exposed to hyperoxia: a retrospective multicentre cohort study. Neurocrit Care. 2021;34:441–8.
Barbateskovic M, Schjørring OL, Krauss SR, Meyhoff CS, Jakobsen JC, Rasmussen BS, et al. Higher vs lower oxygenation strategies in acutely Ill adults. Chest. 2021;159:154–73.
Raj R, Bendel S, Reinikainen M, Kivisaari R, Siironen J, Lång M, et al. Hyperoxemia and long-term outcome after traumatic brain injury. Crit Care. 2013;17:R177.
Brueckl C, Kaestle S, Kerem A, Habazettl H, Krombach F, Kuppe H, et al. Hyperoxia-induced reactive oxygen species formation in pulmonary capillary endothelial cells in situ. Am J Respir Cell Mol Biol. 2006;34:453–63.
Brugniaux JV, Coombs GB, Barak OF, Dujic Z, Sekhon MS, Ainslie PN. Highs and lows of hyperoxia: physiological, performance, and clinical aspects. Am J Physiol Regul Integrat Comp Physiol. 2018;315:R1-27.
Farquhar H, Weatherall M, Wijesinghe M, Perrin K, Ranchord A, Simmonds M, et al. Systematic review of studies of the effect of hyperoxia on coronary blood flow. Am Heart J. 2009;158:371–7.
Cornet AD, Kooter AJ, Peters MJ, Smulders YM. The potential harm of oxygen therapy in medical emergencies. Crit Care. 2013;17:313.
Damiani E, Donati A, Girardis M. Oxygen in the critically ill. Curr Opin Anaesthesiol. 2018;31:129–35.
Crawford P, Good PA, Gutierrez E, Feinberg JH, Boehmer JP, Silber DH, et al. Effects of supplemental oxygen on forearm vasodilation in humans. J Appl Physiol. 1997;82:1601–6.
Robba C, Siwicka-Gieroba D, Sikter A, Battaglini D, Dąbrowski W, Schultz MJ, et al. Pathophysiology and clinical consequences of arterial blood gases and pH after cardiac arrest. Intensive Care Med Exp. 2020;8:19.
Lång M, Skrifvars MB, Siironen J, Tanskanen P, Ala-Peijari M, Koivisto T, et al. A pilot study of hyperoxemia on neurological injury, inflammation and oxidative stress. Acta Anaesthesiol Scand. 2018;62:801–10.
Ebner F, Ullén S, Åneman A, Cronberg T, Mattsson N, Friberg H, et al. Associations between partial pressure of oxygen and neurological outcome in out-of-hospital cardiac arrest patients: an explorative analysis of a randomized trial. Crit Care. 2019;23:30.
Bellomo R, Bailey M, Eastwood GM, Nichol A, Pilcher D, Hart GK, et al. Arterial hyperoxia and in-hospital mortality after resuscitation from cardiac arrest. Crit Care. 2011;15:R90.
Wang C-H, Chang W-T, Huang C-H, Tsai M-S, Yu P-H, Wang A-Y, et al. The effect of hyperoxia on survival following adult cardiac arrest: A systematic review and meta-analysis of observational studies. Resuscitation. 2014;85:1142–8.
Vincent J-L, Taccone FS, He X. Harmful effects of hyperoxia in postcardiac arrest, sepsis, traumatic brain injury, or stroke: the importance of individualized oxygen therapy in critically Ill patients. Can Respir J. 2017;2017:1–7.
Singer M, Young PJ, Laffey JG, Asfar P, Taccone FS, Skrifvars MB, et al. Dangers of hyperoxia. Crit Care. 2021;25:440.
Chu DK, Kim LH-Y, Young PJ, Zamiri N, Almenawer SA, Jaeschke R, et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis. The Lancet. 2018;391:1693–705.
ICU-ROX Investigators and the Australian and New Zeland Intensive Care Society Clinical Trials Group. Conservative oxygen therapy during mechanical ventilation in the ICU. New England J. Med. 2020;382:989–98.
Young PJ, Bellomo R. The risk of hyperoxemia in ICU patients. much ado about O2. Am J Respir Crit Care Med. 2019;200:1333–5.
Gelissen H, de Grooth H-J, Smulders Y, Wils E-J, de Ruijter W, Vink R, et al. Effect of low-normal vs high-normal oxygenation targets on organ dysfunction in critically Ill patients. JAMA. 2021;326:940.
Barrot L, Asfar P, Mauny F, Winiszewski H, Montini F, Badie J, et al. Liberal or conservative oxygen therapy for acute respiratory distress syndrome. N Engl J Med. 2020;382:999–1008.
Schjørring OL, Klitgaard TL, Perner A, Wetterslev J, Lange T, Siegemund M, et al. Lower or higher oxygenation targets for acute hypoxemic respiratory failure. N Engl J Med. 2021;384:1301–11.
Madotto F, Rezoagli E, Pham T, Schmidt M, McNicholas B, Protti A, et al. Hyperoxemia and excess oxygen use in early acute respiratory distress syndrome: insights from the LUNG SAFE study. Crit Care. 2020;24:125.
Kilgannon JH. Association between arterial hyperoxia following resuscitation from cardiac arrest and in-hospital mortality. JAMA. 2010;303:2165.
Asfar P, Schortgen F, Boisramé-Helms J, Charpentier J, Guérot E, Megarbane B, et al. Hyperoxia and hypertonic saline in patients with septic shock (HYPERS2S): a two-by-two factorial, multicentre, randomised, clinical trial. Lancet Respir Med. 2017;5:180–90.
Demiselle J, Wepler M, Hartmann C, Radermacher P, Schortgen F, Meziani F, et al. Hyperoxia toxicity in septic shock patients according to the Sepsis-3 criteria: a post hoc analysis of the HYPER2S trial. Ann Intensiv Care. 2018;8:90.
Young P, Mackle D, Bellomo R, Bailey M, Beasley R, Deane A, et al. Conservative oxygen therapy for mechanically ventilated adults with sepsis: a post hoc analysis of data from the intensive care unit randomized trial comparing two approaches to oxygen therapy (ICU-ROX). Intensiv Care Med. 2020;46:17–26.
Alali AS, Temkin N, Vavilala MS, Lele AV, Barber J, Dikmen S, et al. Matching early arterial oxygenation to long-term outcome in severe traumatic brain injury: target values. J Neurosurg. 2020;132:537–44.
Rincon F, Kang J, Maltenfort M, Vibbert M, Urtecho J, Athar MK, et al. Association between hyperoxia and mortality after stroke. Crit Care Med. 2014;42:387–96.
López HV, Vivas MF, Ruiz RN, Martínez JR, Navaridas BG-V, Villa MG, et al. Association between post-procedural hyperoxia and poor functional outcome after mechanical thrombectomy for ischemic stroke: an observational study. Ann Intensive Care. 2019;9:59.
Fukuda S, Koga Y, Fujita M, Suehiro E, Kaneda K, Oda Y, et al. Hyperoxemia during the hyperacute phase of aneurysmal subarachnoid hemorrhage is associated with delayed cerebral ischemia and poor outcome: a retrospective observational study. J Neurosurg. 2021;134:25–32.
Reynolds RA, Amin SN, Jonathan SV, Tang AR, Lan M, Wang C, et al. Hyperoxemia and cerebral vasospasm in aneurysmal subarachnoid hemorrhage. Neurocrit Care. 2021;35:30–8.
Donnelly J, Czosnyka M, Adams H, Robba C, Steiner LA, Cardim D, et al. Individualizing thresholds of cerebral perfusion pressure using estimated limits of autoregulation. Crit Care Med. 2017;45:1464–71.
Cinotti R, Pelosi P, Schultz MJ, Aikaterini I, Alvarez P, Badenes R, et al. Extubation strategies in neuro-intensive care unit patients and associations with outcomes: the ENIO multicentre international observational study. Ann Transl Med. 2020;8:503–503.
General assembly of the World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. J Am Coll Dent. 2014;81:14–8.
von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int J Surg. 2014;12:1495–9.
European Medicine Agiencies. Guideline for Good Clinical Practice E6 (R1) [Internet]. Available from: https://www.ema.europa.eu/en/documents/scientific-guideline/ich-e6-r1-guideline-good-clinical-practice_en.pdf
Dixon JR. The International Conference on Harmonization Good Clinical Practice Guideline. Quality Assurance. 1999;6:65–74.
Cinotti R, Mijangos JC, Pelosi P, Haenggi M, Gurjar M, Schultz MJ, et al. Extubation in neurocritical care patients: the ENIO international prospective study. Intensive Care Med. 2022;
Robba C, Poole D, McNett M, Asehnoune K, Bösel J, Bruder N, et al. Mechanical ventilation in patients with acute brain injury: recommendations of the European Society of Intensive Care Medicine consensus. Intensive Care Med. 2020;46:2397–410.
Yokoyama S, Hifumi T, Kawakita K, Tamiya T, Minamino T, Kuroda Y. Early hyperoxia in the intensive care unit is significantly associated with unfavorable neurological outcomes in patients with mild-to-moderate aneurysmal subarachnoid hemorrhage. Shock. 2019;51:593–8.
Robba C, Badenes R, Battaglini D, Ball L, Sanfilippo F, Brunetti I, et al. Oxygen targets and 6-month outcome after out of hospital cardiac arrest: a pre-planned sub-analysis of the targeted hypothermia versus targeted normothermia after Out-of-Hospital Cardiac Arrest (TTM2) trial. Crit Care. 2022;26:323.
Roberts BW, Kilgannon JH, Hunter BR, Puskarich MA, Pierce L, Donnino M, et al. Association between early hyperoxia exposure after resuscitation from cardiac arrest and neurological disability. Circulation. 2018;137:2114–24.
Royston P, Sauerbrei W. Multivariable model-building: a pragmatic approach to regression analysis based on fractional polynomials for modelling continuous variables. Royston P, Sauerbrei W, editors. Wiley; 2008.
Jann B. Relative distribution analysis in Stata. Stata J. 2021;21:885–951.
Stata corp. Stata Statistical Software. College Station, TX: StataCorp LLC.; 2021.
Nelskylä A, Parr MJ, Skrifvars MB. Prevalence and factors correlating with hyperoxia exposure following cardiac arrest – an observational single centre study. Scand J Trauma Resusc Emerg Med. 2013;21:35.
O’Driscoll BR, Howard LS, Earis J, Mak V. British Thoracic Society Guideline for oxygen use in adults in healthcare and emergency settings. BMJ Open Respir Res. 2017;4: e000170.
Röttgering JG, de Man AME, Schuurs TC, Wils E-J, Daniels JM, van den Aardweg JG, et al. Determining a target SpO2 to maintain PaO2 within a physiological range. Zivkovic AR, editor. PLoS One. 2021;16:e0250740.
Rezoagli E, Petrosino M, Rebora P, Menon DK, Mondello S, Cooper DJ, et al. High arterial oxygen levels and supplemental oxygen administration in traumatic brain injury: insights from CENTER-TBI and OzENTER-TBI. Intensive Care Med. 2022;
Hawryluk GWJ, Rubiano AM, Totten AM, O’Reilly C, Ullman JS, Bratton SL, et al. Guidelines for the management of severe traumatic brain injury: 2020 update of the decompressive craniectomy recommendations. Neurosurgery. 2020;87:427–34.
Chesnut R, Aguilera S, Buki A, Bulger E, Citerio G, Cooper DJ, et al. A management algorithm for adult patients with both brain oxygen and intracranial pressure monitoring: the Seattle International Severe Traumatic Brain Injury Consensus Conference (SIBICC). Intensive Care Med. 2020;46:919–29.
Davis DP, Meade W, Sise MJ, Kennedy F, Simon F, Tominaga G, et al. Both hypoxemia and extreme hyperoxemia may be detrimental in patients with severe traumatic brain injury. J Neurotrauma. 2009;26:2217–23.
Giannì G, Taccone FS, Bogossian EG. The impact of short-term normobaric hyperoxia on brain metabolism: a pilot microdialysis study. Neurocrit Care. 2022;37:770–4.
Tisdall MM, Tachtsidis I, Leung TS, Elwell CE, Smith M. Increase in cerebral aerobic metabolism by normobaric hyperoxia after traumatic brain injury. J Neurosurg. 2008;109:424–32.
Jeon SB, Choi HA, Badjatia N, Schmidt JM, Lantigua H, Claassen J, et al. Hyperoxia may be related to delayed cerebral ischemia and poor outcome after subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. 2014;85:1301–7.
Fallenius M, Raj R, Reinikainen M, Bendel S, Skrifvars MB. Association between high arterial oxygen tension and long-term survival after spontaneous intracerebral hemorrhage. Crit Care Med. 2016;44:180–7.
Starke RM, Kassell NF. The link between hyperoxia, delayed cerebral ischaemia and poor outcome after aneurysmal SAH: association or therapeutic endeavour. J Neurol Neurosurg Psychiatry. 2014;85:1292–1292.
Hoffman WE, Wheeler P, Edelman G, Charbel FT, Torres NJ, Ausman JI. Hypoxic brain tissue following subarachnoid hemorrhage. Anesthesiology. 2000;92:442–442.
Vespa PM. Metabolic penumbra in intracerebral hemorrhage. Stroke. 2009;40:1547–8.
Acknowledgements
The ENIO Collaborators: Paër-sélim Abback1, Anaïs Codorniu1, Giuseppe Citerio2, Vittoria Ludovica Sala3, Marinella Astuto4, Eleonora Tringali4, Daniela Alampi5, Monica Rocco5, Jessica Giuseppina Maugeri6, Bellissima Agrippino6, Matteo Filippini7, Nicoletta Lazzeri7, Andrea Cortegiani8, Mariachiara Ippolito8, Chiara Robba9, Denise Battaglini9, Patrick Biston10, Mohamed Fathi Al-Gharyani11, Russell Chabanne12, Léo Astier12, Benjamin Soyer13, Samuel Gaugain13, Alice Zimmerli14, Urs Pietsch15, Miodrag Filipovic15, Giovanna Brandi16, Giulio Bicciato16, Ainhoa Serrano17, Berta Monleon17, Peter van Vliet18, Benjamin Marcel Gerretsen18, Iris Xochitl Ortiz-macias19, Jun Oto20, Noriya Enomoto21, Tomomichi Matsuda22, Nobutaka Masui22, Pierre Garçon23, Jonathan Zarka23, Wytze J. Vermeijden24, Alexander Daniel Cornet24, Sergio Reyes Inurrigarro25, Rafael Cirino Lara Domínguez25, Maria Mercedes Bellini26, Maria Milagros Gomez-Haedo26, Laura Lamot27, Jose Orquera28, Matthieu Biais29, Delphine Georges29, Arvind Baronia30, Roberto Carlos Miranda-Ackerman31, Francisco José Barbosa-Camacho31, John Porter32, Miguel Lopez-Morales32, Thomas Geeraerts33, Baptiste Compagnon33, David Pérez-Torres34, Estefanía Prol-Silva34, Hana Basheer Yahya35, Ala Khaled36, Mohamed Ghula36, Andrea Cracchiolo Neville37, Maria Daniela Palma37, Cristian Deana38, Luigi Vetrugno39, Manuel J. Rivera Chavez40, Rocio Mendoza Trujillo40, Vincent Legros41, Benjamin Brochet41, Olivier Huet42, Marie Geslain42, Mathieu van der Jagt43, Job van Steenkiste43, Hazem Ahmed44, Alexander Edward Coombs45, Jessie Welbourne45, Ana Alicia Velarde Pineda46, Víctor Hugo Nubert Castillo46, Mohammed A. Azab47, Ahmed Y. Azzam47, David Michael Paul van Meenen42, Gilberto Adrian Gascav49, Alfredo Arellano49, Forttino Galicia-Espinosa50, José Carlos García-Ramos50, Ghanshyam Yadav51, Amarendra Kumar Jha51, Vincent Robert-Edan52, Pierre-Andre Rodie-Talbere52, Gaurav Jain53, Sagarika Panda53, Sonika Agarwal54, Yashbir Deewan54, Gilberto Adrian Gasca49, Alfredo Arellano49, Syed Tariq Reza55, Md. Mozaffer Hossain55, Christos Papadas56, Vasiliki Chantziara57, Chrysanthi Sklavou57, Yannick Hourmant58, Nicolas Grillot58, Job van Steenkiste59, Mathieu van der Jagt59, Romain Pirracchio60, Abdelraouf Akkari61, Mohamed Abdelaty62, Ahmed Hashim62, Yoann Launey63, Elodie Masseret63, Sigismond Lasocki64, Soizic Gergaud64, Nicolas Mouclier65, Sulekha Saxena66, Avinash Agrawal66, Shakti Bedanta Mishra67, Samir Samal67, Julio Cesar Mijangos19, Mattias Haënggi14, Mohan Gurjar30, Mohan Gurjar30, Marcus J. Schultz68, Callum Kaye69, Daniela Agustin Godoy28, Pablo Alvarez26, Aikaterini Ioakeimidou56, Yoshitoyo Ueno20, Rafael Badenes70, Abdurrahmaan Ali Suei Elbuzidi61, Michaël Piagnerelli10, Muhammed Elhadi71, Syed Tariq Reza72, Mohammed Atef Azab47, Jean Catherine Digitale73, Nicholas Fong60, Ricardo Campos Cerda74, Norma de la Torre Peredo74. Affiliations: 1Department of Anesthesiology and Critical Care, Beaujon Hospital, DMU Parabol, AP-HP. Nord, 100 Boulevard du General Leclerc, Clichy, France. 2Neurointensive Care Unit, Ospedale San Gerardo, Azienda Socio-Sanitaria Territoriale di Monza, 23 Via Aliprandi, Monza, Italy. 3NeuroIntensive Care Unit, Monza, Italy. 4Anesthesia and Intensive Care Unit, A.O.U. Policlinico “G. Rodolico - S. Marco”, Via Santa Sofia 78, Catania, Italy. 5Sapienza Rome University, A.O.U. Sant'Andrea, Via di grottarossa, 1035/1039, Rome, Italy. 6Arnas garibaldi Catania, Piazza s.maria di gesu' 5, Catania, Italy. 7University Division of Anesthesiology and Critical Care Medicine, Piazzale Spedali Civili, 1, Brescia, Italy. 8Policlinico Paolo Giaccone, Università degli Studi di Palermo, Via del vespro 129, Palermo, Italy. 9San Martino Policlinico Hospital - IRCCS for Oncology and Neurosciences, 10 Largo Rosanna Benzi, Genova. Italy. 10CHU Charleroi- Hôpital Civil Marie-Curie, Université libre de Bruxelles, 140 Chaussée de Bruxelles, Charleroi, Belgium. 11Benghazi Medical Center, Eastern Selmain, Benghazi, Libya. 12Perioperative Medicine Department, Clermont-Ferrand University Hospital, Neurocritical Care Unit, 58 rue Montalembert, Clermont-Ferrand, France. 13Department of Anesthesia and Critical Care, AP-HP, Hôpital Lariboisière, DMU Parabol, Paris, France. 14Department of Intensive Care Medicine, Inselspital, Bern University Hospital, University of Bern, Freiburgstrasse, Bern, Switzerland. 15Department of Anaesthesiology and Intensive Care Medicine, Cantonal Hospital St Gallen, Rorschacher Strasse 95, St. Gallen, Switzerland. 16Institute for Intensive Care Medicine, University Hospital of Zurich, Rämistrasse 100, Zurich, Switzerland. 17Hospital Clinico Universitario Valencia, Avenida Blasco Ibañez, 17, Valencia, Spain. 18Haaglanden Medical Center, Lijnbaan 32, The Hague, Netherlands. 19Hospital Civil de Guadalajara "Fray Antonio Alcalde", Hospital No. 278, Col. El Retiro, Guadalajara, Mexico. 20Tokushima University Hospital, 2-50-1, Kuramoto-cho, Tokushima, Japan. 21Tokushima Prefectural Central Hospital, 1-10-3, Kuramoto-cho, Tokushima, Japan. 22Sapporo Higashi Tokushukai Hospital, 3-1, Kita 33-jo Higashi 14-chome, Higashi-ku, Sapporo, Japan. 23Service de reanimation, 2-4 Cours de la Gondoire, Jossigny, France. 24Department of intensive care, Medisch Spectrum Twente MST, Enschede, the Netherlands, Koningsplein 1, Enschede, The Netherlands, 25UMAE Hospital de Traumatologia y Ortopedia IMSS, Diagonal Defensores de la Republica esquin 6 poniente, Puebla, Mexico. 26Hospital Maciel, ASSE, 25 de Mayo 174, Montevideo, Uruguay. 27Hospital Municipal Leonidas Lucero, Bahia Blanca, Buenos Aires, Argentina.28Sanatorio Pasteur, Chacabuco 675, Catamarca, Argentina. 29Pellegrin SAR Tripode, Pellegrin SAR Tripode, Bordeaux, France. 30Department of Critical Care Medicine, Sanjay Gandhi Postgraduate Institute of Medical Sciences (SGPGIMS), Lucknow. 31Hospital San Javier, Av Pablo Casals 640, Prados Providencia, Guadalajara, Jalisco, Mexico. 32St George's Hospital, Blackshaw Road, London, UK. 33Toulouse University Hospital, Place du Dr Baylac, Toulouse, France. 34Servicio de Medicina Intensiva, Hospital Universitario Río Hortega, Calle Dulzaina, 2, Valladolid, Spain. 35Zliten Medical Centre, Zliten, Libya. 36Abo Selim Trauma Hospital, Tripoli, Libya. 37Terapia Intensiva Con Trauma Center Arnas Ospedale Civico Palermo, Piazza n Leotta 4, Palermo, Italy. 38Academic Hospital of Udine, Piazzale S.Maria della Misericordia, 15, Udine, Chieti, Italy. 39University of Chieti-Pescara, Chieti, Italy. 40Hospital de Alta Especialidad del Bajio, Blvd.Milenio #130 Col. San Carlos la Roncha, León Guanajuato, Mexico. 41Department of Anesthesiology and Critical Care, University Hospital of Reims, Hopital Maison Blanche, 45 Rue Cognacq Jay, Reims, France. 42Department of Anesthesiology and Critical Care, La Cavale Blanche, Boulevard Tanguy Prigent, Brest, France. 43Erasmus MC, Dr Molewaterplein 40, Rotterdam, Netherlands. 44Seoul Clinic, Tripoli, Libya. 45Department of Intensive Care Medicine, University Hospital Plymouth, Derriford Road, Plymouth, Devon, Plymouth, UK. 46Hospital General Regional # 180 IMSS, Carretera a San Sebastian # 1000 Col. Las cumbres 2 Tlajomulco de Zúñiga, Guadalajara, Mexico. 47Cairo University, Giza, Cairo, Egypt. 48Amsterdam UMC, Meibergdreef 9, Amsterdam, Netherlands. 49Hospital Regional de Alta Especialidad de Ixtapaluca, Carretera Federal Mexico -Puebla Km. 34.5, Pueblo de Zoquiapan, Ixtapaluca, Mexico. 50UMAE Hospital de Traumatología y Ortopedia No 21, IMSS Monterrey, Av. J.M. Pino Suárez S/N esq. 15 de Mayo, Monterrey, Mexico. 51Department of Anesthesia, IMS, BHU, Trauma ICU, Varanasi, India. 52Nantes-Laennec, Hopital Laennec CHU Nantes, 1 Bd Jacques Monod, Nantes, France. 53Critical Care Unit, Dept. Of Anaesthesiology and Critical Care, All India Institute of Medical Sciences, Rishikesh, India. 54HIMS, B18/8, HIMS Campus, Dehradun, India. 55Department of Anaesthesia, Analgesia, Palliative & Intensive Care, Dhaka Medical College Hospital, Dhaka, Bangladesh. 56ICU of ASKLEPIEIO G.H.A, V.PAULOU 1, Athens, Greece. 57Saint Savvas Hospital, 151 Alexandras Avenue, Athens, Greece . 58Department of Anesthesiology and Critical Care, Hôtel-Dieu, 1 place Alexis Ricordeau, Nantes, France. 59Erasmus Medical Centre, Doctor Molewaterplein 40, Rotterdam, Netherlands. 60Department of Anesthesia and Perioperative Care, University of California, UCSF, 1001 Potrero Ave, San Francisco, USA. 61Qatar-1, HMC-Doha-Qatar, Doha, Qatar. 62Qatar-2, HMC-Doha-Qatar, Doha, Qatar. 63Department of Anesthesiology and Critical Care, Hopital Pontchaillou, 2 rue Henri le Guilloux, Rennes, France. 64Department of Anesthesiology and Critical Care, 4 rue Larrey, Angers, France. 65Department of Anesthesiology and Critical Care, Hôtel-Dieu, 1 place Alexis Ricordeau , Nantes, France. 66Department of Critical Care Medicine, King George's Medical University, Lucknow, India. 67IMS and SUM Hospital, K8 Kalinga Nagar, Bhubaneswar, India. 68Department of Intensive Care, Amsterdam University Medical Centers, Amsterdam, Netherlands. 69Aberdeen Royal Infirmary, Foresthill, Aberdeen, UK. 70Hospital Clínico Universitario Valencia, Valencia, Spain. 71Faculty of Medicine, University of Tripoli, Furnaj, University road, Tripoli, Lybia. 72Dhaka Medical College Hospital, Dhaka, Bangladesh. 73University of California, UCSF, 550 16th St, San Francisco, USA. 74Critical Care Unit, Hospital General Regional no. 46, Instituto Mexicano del Seguro Social, 2063 Lazaro Cárdenas Av, Guadalajara , Mexico
Funding
The authors have not received any financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Consortia
Contributions
CR and PP: conception of the work, design. CR, DB, RB, and PP: data interpretation, drafting the manuscript, critical revision of the manuscript, final approval. RB and PP: supervision of the work. All authors: critical revision of the manuscript, final approval.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that the article content was composed in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical Approval/Informed Consent
Approval to conduct this subanalysis was not necessary. Approval to enroll patients in the ENIO main study was obtained from the institutional review board of the promoter center (Groupe Nantais d’Éthique dans le Domaine de la Santé, IRB No. 7/11/2017) and of each participating center. Informed consent was generally waived in accordance with the observational nature of the ENIO study but if necessary was collected in accordance with the local regulations of each involved institutional review board. Informed consent was obtained from the patient or from the patient’s next of kin in case the patient was unable to give the consent at the time of enrollment.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The ENIO Collaborators: Authors and affiliations are present in Acknowledgment section.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Robba, C., Battaglini, D., Cinotti, R. et al. Individualized Thresholds of Hypoxemia and Hyperoxemia and their Effect on Outcome in Acute Brain Injured Patients: A Secondary Analysis of the ENIO Study. Neurocrit Care 40, 515–528 (2024). https://doi.org/10.1007/s12028-023-01761-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-023-01761-x