
Abstract
Purpose
Soluble Fas Ligand (sFasL) is one of the main ligands that activates the apoptosis extrinsic pathway. Higher expression of FasL in brain samples and higher cerebrospinal fluid FasL concentrations in traumatic brain injury (TBI) patients than in controls have been found. However, the potential association between blood sFasL concentrations and TBI mortality has not been reported. Therefore, the objective of this study was to determine whether that association exists.
Methods
We included patients with a severe isolated TBI, defined as < 9 points in Glasgow Coma Scale (GCS) and < 10 non-cranial aspects points in Injury Severity Score in this observational and prospective study performed in 5 Intensive Care Units. We measured serum sFasL concentrations on day 1 of TBI.
Results
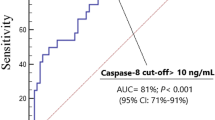
We found that 30-day survivor (n = 59) in comparison to non-survivor patients (n = 24) had higher GCS (p = 0.001), lower age (p = 0.004), lower APACHE-II score (p < 0.001), lower intracranial pressure (ICP) (p = 0.01), lower computer tomography (CT) findings of high risk of death (p = 0.02) and lower serum sFasL concentrations (p < 0.001). The area under the curve for mortality prediction by serum sFasL levels was of 75% (95% CI = 63%–87%; p < 0.001). In Kaplan–Meier analysis was found that patients with serum sFasL levels > 29.2 pg/mL had a higher mortality rate (Hazard ratio = 6.2; 95% CI = 2.6–14.8; p < 0.001). Multiple logistic regression analysis found an association between serum sFasL levels and mortality after controlling for GCS, age and CT findings (OR = 1.055; 95% CI = 1.018–1.094; p = 0.004), and after controlling for APACHE-II, ICP and CT findings (OR = 1.048; 95% CI = 1.017–1.080; p = 0.002).
Conclusions
The association between serum sFasL levels and 30-day mortality in TBI patients was the major novel finding of our study; however, future validation could be interesting to confirm those results.


Similar content being viewed by others


Abbreviations
- TBI:
-
Traumatic brain injury
- GCS:
-
Glasgow Coma Scale
- ISS:
-
Injury Severity Score
- PaO2 :
-
Pressure of arterial oxygen/fraction inspired oxygen
- FIO2 :
-
Pressure of arterial oxygen/fraction inspired oxygen
- aPTT:
-
Activated partial thromboplastin time
- APACHE II:
-
Acute Physiology and Chronic Health Evaluation
References
Brain Trauma Foundation, American Association of Neurological Surgeons, Congress of Neurological Surgeons. Guidelines for the management of severe traumatic brain injury. J Neurotrauma. 2007;24:S1-106.
Zhang X, Chen Y, Jenkins LW, Kochanek PM, Clark RS. Bench-to-bedside review: apoptosis/programmed cell death triggered by traumatic brain injury. Crit Care. 2005;9:66–75.
Kunz A, Dirnagl U, Mergenthaler P. Acute pathophysiological processes after ischaemic and traumatic brain injury. Best Pract Res Clin Anaesthesiol. 2010;24:495–509.
Cavallucci V, D’Amelio M. Matter of life and death: the pharmacological approaches targeting apoptosis in brain diseases. Curr Pharm Des. 2011;17:215–29.
Wang K, Liu B, Ma J. Research progress in traumatic brain penumbra. Chin Med J (Engl). 2014;127:1964–8.
Rovegno M, Soto PA, Sáez JC, von Bernhardi R. Biological mechanisms involved in the spread of traumatic brain damage. Med Intensiva. 2012;36:37–44.
Glushakova OY, Glushakov AA, Wijesinghe DS, Valadka AB, Hayes RL, Glushakov AV. Prospective clinical biomarkers of caspase-mediated apoptosis associated with neuronal and neurovascular damage following stroke and other severe brain injuries: Implications for chronic neurodegeneration. Brain Circ. 2017;3:87–108.
Zhang X, Graham SH, Kochanek PM, Marion DW, Nathaniel PD, Watkins SC, Clark RSB. Caspase-8 expression and proteolysis in human brain after severe head injury. FASEB J. 2003;17:1367–9.
Miñambres E, Ballesteros MA, Mayorga M, Marin MJ, Muñoz P, Figols J, López-Hoyos M. Cerebral apoptosis in severe traumatic brain injury patients: an in vitro, in vivo, and postmortem study. J Neurotrauma. 2008;25:581–91.
Jiang W, Jin P, Wei W, Jiang W. Apoptosis in cerebrospinal fluid as outcome predictors in severe traumatic brain injury: an observational study. Med (Baltimore). 2020;99:e20922.
Uzan M, Erman H, Tanriverdi T, Sanus GZ, Kafadar A, Uzun H. Evaluation of apoptosis in cerebrospinal fluid of patients with severe head injury. Acta Neurochir (Wien). 2006;148:157–64.
Lenzlinger PM, Marx A, Trentz O, Kossmann T, Morganti-Kossmann MC. Prolonged intrathecal release of soluble Fas following severe traumatic brain injury in humans. J Neuroimmunol. 2002;122:167–74.
Crespo AR, Da Rocha AB, Jotz GP, Schneider RF, Grivicich I, Pinheiro K, Zanoni C, Regner A. Increased serum sFas and TNFalpha following isolated severe head injury in males. Brain Inj. 2007;21:441–7.
Qiu J, Whalen MJ, Lowenstein P, Fiskum G, Fahy B, Darwish R, Aarabi B, Yuan J, Moskowitz MA, MA, . Upregulation of the Fas receptor death-inducing signaling complex after traumatic brain injury in mice and humans. J Neurosci. 2002;22:3504–11.
Ertel W, Keel M, Stocker R, Imhof HG, Leist M, Steckholzer U, Tanaka M, Trentz O, Nagata S. Detectable concentrations of Fas ligand in cerebrospinal fluid after severe head injury. J Neuroimmunol. 1997;80:93–6.
Baker SP, O’Neill B, Haddon W Jr, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14:187–96.
Teasdale G, Jennett B. Assessement of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–4.
Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985;13:818–29.
Marshall LF, Marshall SB, Klauber MR, Van Berkum CM, Eisenberg H, Jane JA, Luerssen TG, Marmarou A, Foulkes MA. The diagnosis of head injury requires a classification based on computed axial tomography. J Neurotrauma. 1992;9(Suppl 1):S287-292.
Kleinbaum DG, Kupper LL, Muller KE, Nizam A. Polynomial regression. In: Kleinbaum DG, Kupper LL, Muller KE, Nizam A, editors. Applied regression analysis and other multivarible methods. California: Duxbury Press; 1998. p. 281–316.
Youden WJ. Index for rating diagnostic tests. Cancer. 1950;3:32–5.
Yin XH, Yan JZ, Yang G, Chen L, Xu XF, Hong XP, Wu SL, Hou XY, Zhang GY. PDZ1 inhibitor peptide protects neurons against ischemia via inhibiting GluK2-PSD-95-module-mediated Fas signaling pathway. Brain Res. 2016;1637:64–70.
Yin XH, Han YL, Zhuang Y, Yan JZ, Li C. Geldanamycin inhibits Fas signaling pathway and protects neurons against ischemia. Neurosci Res. 2017;124:33–9.
Ullah I, Chung K, Oh J, Beloor J, Bae S, Lee SC, Lee M, Kumar P, Lee SK. Intranasal delivery of a Fas-blocking peptide attenuates Fas-mediated apoptosis in brain ischemia. Sci Rep. 2018;8:15041.
Acknowledgments
This study was supported by a grant from Instituto de Salud Carlos III (PI-18-00500) (Madrid, Spain) and co-financed with Fondo Europeo de Desarrollo Regional (FEDER). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Funding
This study was supported by a grant from Instituto de Salud Carlos III (PI-18–00500) (Madrid, Spain) and co-financed with Fondo Europeo de Desarrollo Regional (FEDER).
Author information
Authors and Affiliations
Contributions
LL conceived, designed and coordinated the study, participated in acquisition of data, and drafted the manuscript; MMM, LRG, JSV, JJC, JC and AAC participated in acquisition of data and provided useful suggestions; APC, AFGR and CFM carried out serum sFasL levels determinations and provided useful suggestions; AJ interpreted the data and provided useful suggestions; all authors read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no competing interests.
Informed Consent
This study was carried after the approval of Institutional Review Board of all participating hospitals and with the written informed consent from legal guardians of patients.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Lorente, L., Martín, M.M., Pérez-Cejas, A. et al. High Serum Soluble Fas Ligand Levels in Non-survivor Traumatic Brain Injury Patients. Neurocrit Care 35, 249–254 (2021). https://doi.org/10.1007/s12028-020-01158-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12028-020-01158-0