
Abstract
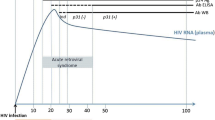
Primary HIV infection refers to the events surrounding acquisition of HIV infection. It is associated with a nonspecific clinical syndrome that occurs 2 to 4 weeks after exposure in 40% to 90% of individuals acquiring HIV. Patients identified before seroconversion often have very high plasma HIV RNA titers that, without treatment, gradually decrease to reach a set point. Treatment of primary HIV infection with highly active antiretroviral therapy does not prevent establishment of chronic infection. However, very early therapy could potentially decrease the viral set point, prevent viral diversification, preserve immune function, improve clinical outcomes, and decrease secondary transmission. These benefits have not yet been definitely demonstrated. Transmission of viral strains with decreased susceptibility to antiviral drugs has led to recommendations for resistance testing in primary infection before initiation of therapy. Immunomodulators and vaccines are also under study as adjuvant therapy for treatment of primary HIV infection.
Similar content being viewed by others


References and Recommended Reading
Joint UN Programme on HIV/AIDS: AIDS epidemic update. http://www.unaids.org.
Schacker T, Collier AC, Hughes J, et al.: Clinical and epidemiologic features of primary HIV infection. Ann Intern Med 1996, 125:257–264.
Kahn JO, Walker BD: Acute human immunodeficiency virus type 1 infection. N Engl J Med 1998, 339:33–39.
Vanhems P, Hughes J, Collier AC, et al.: Comparison of clinical features, CD4+ and CD8+ responses among patients with acute HIV-1 infection. AIDS 2000, 14:375–381.
Schacker TW, Hughes JP, Shea T, et al.: Biological and virologic characteristics of primary HIV infection. Ann Intern Med 1998, 128:613–260.
Keet IP, Krijnen P, Koot M, et al.: Predictors of rapid progression to AIDS in HIV-1 seroconverters. AIDS 1993, 7:51–58.
Pantaleo G, Cohen OJ, Schacker T, et al.: Evolutionary pattern of human immunodeficiency virus (HIV) replication and distribution in lymph nodes following primary infection: implications for antiviral therapy. Nat Med 1998, 4:341–345.
Chun TW, Engel D, Berrey MM, et al.: Early establishment of a pool of latently infected, resting CD4+ T cells during primary HIV-1 infection. Proc Natl Acad Sci USA 1998, 95:8869–8873.
Spira AI, Marx PA, Patterson BK, et al.: Cellular targets of infection and route of viral dissemination after an intravaginal inoculation of simian immunodeficiency virus into rhesus macaques. J Exp Med 1996, 183:215–225.
Pedersen C, Katzenstein T, Nielsen C, et al.: Prognostic value of serum HIV-RNA levels at virologic steady state after seroconversion: relation to CD4 cell count and clinical course of primary infection. J Acquir Immune Defic Syndr Hum Retrovirol 1997, 16:93–99.
Mellors JW, Muñoz A, Giorgi JV, et al.: Plasma viral load and CD4+ lymphocytes as prognostic markers of HIV-1 infection. Ann Intern Med 1997, 126:946–954.
Zhu T, Mo H, Wang N, et al.: Genotypic and phenotypic characterization of HIV-1 in patients with primary infection. Science 1993, 261:1179–1181.
Shankarappa R, Margolick JB, Gange SJ, et al.: Consistent viral evolutionary changes associated with the progression of human immunodeficiency virus type 1 infection. J Virol 1999, 73:10489–10502.
Hogan CM, Hammer SM: Host determinants in HIV infection and disease. Part 1: cellular and humoral immune responses. Ann Intern Med 2001, 134:761–776.
Hogan CM, Hammer SM: Host determinants in HIV infection and disease. Part 2: genetic factors and implications of antiretroviral therapeutics. Ann Inter Med 2001, 134:978–996.
Musey LK, Krieger JN, Hughes JP, et al.: Early and persistent human immunodeficiency virus type 1 (HIV-1)-specific T helper dysfunction in blood and lymph nodes following acute HIV-1 infection. J Infect Dis 1999, 180:278–284.
Musey L, Hughes J, Schacker T, et al.: Cytotoxic-T-cell responses, viral load, and disease progression in early human immunodeficiency virus type 1 infection. N Engl J Med 1997, 337:1267–1274.
Ogg GS, Jin X, Bonhoeffer S, et al.: Quantitation of HIV-1-specific cytotoxic T lymphocytes and plasma viral RNA load. Science 1998, 279:2103–2106.
Montefiori DC, Altfeld M, Lee PK, et al.: Viremia control despite escape from a rapid and potent autologous neutralizing antibody response after therapy cessation in an HIV-infected individual. J Immunol 2003, 170:3906–3914.
Richman DD, Wrin T, Little SJ, Petropoulos CJ: Rapid evolution of the neutralizing antibody response to HIV type 1 infection. Proc Natl Acad Sci U S A 2003, 100:4144–4149.
Altfeld M, Addo MM, Rosenberg ES, et al.: Influence of HLA-B57 on clinical presentation and viral control during acute HIV infection. AIDS 2003, 17:2581–2591.
Huang Y, Paxton WA, Wolinsky SM, et al.: The role of a mutant CCR5 allele in HIV-1 transmission and disease progression. Nat Med 1996, 2:1240–1243.
Palella FJ Jr, Delaney KM, Moorman AC, et al.: Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med 1998, 338:853–860.
Case-control study of HIV seroconversion in health-care workers after percutaneous exposures to HIV-infected blood: France, United Kingdom, and United States, January 1988–August 1994. MMWR Morb Mortal Wkly Rep 1995, 44:929–933.
Schacker T, Little S, Connick E, et al.: Rapid accumulation of human immunodeficiency virus (HIV) in lymphatic tissue reservoirs during acute and early HIV infection: implications for timing of antiretroviral therapy. J Infect Dis 2000, 181:354–357.
Pilcher CD, Shugars DC, Fiscus SA, et al.: HIV in body fluids during primary HIV infection: implications for pathogenesis, treatment and public health. AIDS 2001, 15:837–845.
Hecht FM, Wang L, Collier A, et al.: Is HAART for primary/early HIV infection associated with improved outcomes after treatment discontinuation? Paper presented at the 10th Conference on Retroviruses and Opportunistic Infections. Boston, MA; February 10–14, 2003.
Mansky LM, Temin HM: Lower in vivo mutation rate of human immunodeficiency virus type 1 than that predicted from the fidelity of purified reverse transcriptase. J Virol 1995, 69:5087–5094.
Berrey MM, Schacker T, Collier AC, et al.: Treatment of primary human immunodeficiency virus type 1 infection with potent antiretroviral therapy reduces frequency of rapid progression to AIDS. J Infect Dis 2001, 183:1466–1475. This study showed a clinical benefit of HAART initiated during primary infection. Patients who were treated during primary infection had significantly less opportunistic infections, mucocutaneous disorders, and respiratory disorders, and less frequent progression to AIDS compared to a group of historic controls.
Smith D, Berrey MM, Robertson M, et al.: Virological and immunological effects of combination antiretroviral therapy during primary HIV-1 infection. J Infect Dis 2000, 182:950–954.
Karlsson AC, Birk M, Lindback S, et al.: Initiation of therapy during primary HIV type 1 infection results in a continuous decay of proviral DNA and a highly restricted viral evolution. AIDS Res Hum Retroviruses 2001, 17:409–416.
Malhotra U, Berrey MM, Huang Y, et al.: Effect of combination antiretroviral therapy on T-cell immunity in acute human immunodeficiency virus type 1 infection. J Infect Dis 2000, 181:121–131.
Rosenberg ES, Altfeld M, Poon SH, et al.: Immune control of HIV-1 after early treatment of acute infection. Nature 2000, 407:523–526.
Altfeld M, Rosenberg ES, Shankarappa R, et al.: Cellular immune responses and viral diversity in individuals treated during acute and early HIV-1 infection. J Exp Med 2001, 193:169–180.
Lisziewicz J, Rosenberg E, Lieberman J, et al.: Control of HIV despite the discontinuation of antiretroviral therapy. N Engl J Med 1999, 340:1683–1684.
Kaufmann D, Lichterfeld M, Altfeld M, et al.: Limited durability of immune control following treated acute HIV infection [abstract]. Paper presented at the 11th Conference on Retroviruses and Opportunistic Infections. San Francisco, CA; February 8–11, 2004. This report is diminished enthusiasm for STI after HAART initiated during acute infection. Although 11 of 14 (79%) subjects were initially able to control viremia, only three of 14 (21%) had sustained control of HIV viremia without HAART for 2 years after the last treatment interruption.
Lafeuillade A, Counillon E, Poggi C, et al.: Predictors of plasma HIV RNA control after discontinuation of HAART initiated at acute infection [abstract]. Paper presented at the 10th Conference on Retroviruses and Opportunistic Infections. Boston, MA; February 10–14, 2003.
Tremblay CL, Hicks JL, Sutton L, et al.: Antiretroviral resistance associated with supervised treatment interruptions in treated acute HIV infection. AIDS 2003, 17:1086–1089.
Altfeld M, Allen TM, Yu XG, et al.: HIV superinfection despite broad CD8+ T-cell responses containing replication of the primary virus. Nature 2002, 420:434–439.
Pilcher CD, Erons JJ, Vernazza PL, et al.: Sexual transmission during the incubation period of primary HIV infection. JAMA 2001, 286:1713–1714.
Yerly S, Vora S, Rizzardi P, et al.: Acute HIV infection: impact on the spread of HIV and transmission of drug resistance. AIDS 2001, 15:2287–2292.
Koopman JS, Jacquez JA, Welch GW, et al.: The role of early HIV infection in the spread of HIV through populations. J Acquir Immune Defic Syndr 1997, 14:249–258.
Miller J, Carr A, Smith D, et al.: Lipodystrophy following antiretroviral therapy of primary HIV infection. AIDS 2000, 14:2406–2407.
Little SJ, Holte S, Routy JP, et al.: Antiretroviral-drug resistance among patients recently infected with HIV. N Engl J Med 2002, 347:385–394. This is the largest study (377 subjects) of antiretroviral resistance among viral isolates of subjects with primary HIV infection. It showed an increasing prevalence of resistance in the United States (22.7% in 88 subjects from 1999–2000 compared to 8% in 213 subjects from 1995–1998) and supports the need for resistance testing before initiating therapy in areas with a high prevalence of resistance.
Boden D, Hurley A, Zhang L, et al.: HIV-1 drug resistance in newly infected individuals. JAMA 1999, 282:1135–1141.
Salomon H, Wainberg MA, Brenner B, et al.: Prevalence of HIV-1 resistant to antiretroviral drugs in 81 individuals newly infected by sexual contact or injecting drug use. AIDS 2000, 14:F17-F23.
Tamalet C, Pasquier C, Yahi N, et al.: Prevalence of drug resistant mutants and virological response to combination therapy in patients with primary HIV-1 infection. J Med Virol 2000, 61:181–186.
Porter K, Pilloy D, Cane P, et al.: Analysis of prevalence of HIV-1 drug resistance in primary infections in the United Kingdom. BMJ 2001, 322:1087–1088.
Grant RM, Hecht FM, Warmerdam M, et al.: Time trends in primary HIV-1 drug resistance among recently infected persons. JAMA 2002, 288:181–188.
Chaix ML, Descamps D, Harzic M, et al.: Stable prevalence of genotypic drug resistance mutations but increase in non-B virus among patients with primary HIV-1 infection in France. AIDS 2003, 17:2635–2643.
Yerly S, Kaiser L, Bru JP, et al.: Transmission of antiretroviral drug-resistant HIV-1 variants. Lancet 1999, 354:729–733.
DHHS guidelines for use of antiretroviral agents in HIVinfected adults and adolescents. http://aidsinfo.nih.gov/ guidelines. Accessed March 1, 2004.
Rizzardi GP, Harari A, Capiluppi B, et al.: Treatment of primary HIV infection with cyclosporin A coupled with highly active antiretroviral therapy. J Clin Invest 2002, 109:681–688.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Stekler, J., Collier, A.C. Primary HIV infection. Curr HIV/AIDS Rep 1, 68–73 (2004). https://doi.org/10.1007/s11904-004-0010-2
Issue Date:
DOI: https://doi.org/10.1007/s11904-004-0010-2