
Abstract
Purpose of Review
To review the current evidence regarding the impact of the coronavirus disease 2019 (COVID-19) pandemic on cardiometabolic health, with a focus on strategies to help mitigate adverse effects on population health.
Recent Findings
Individuals with cardiometabolic disease are particularly vulnerable to worse outcomes with COVID-19 infection. In addition, the pandemic itself has had significant deleterious impact on the cardiometabolic health of the population, including declines in physical activity, increases in smoking and alcohol use, worsening blood pressure and glycemic control, and detrimental effects on mental health. Targeted interventions at the patient and community level will be needed to mitigate the long-term consequences of the COVID-19 pandemic on population cardiometabolic health.
Summary
The COVID-19 pandemic has worsened cardiometabolic health, but there are several opportunities and enhanced tools available to counteract these changes.
Similar content being viewed by others


Introduction
Individuals with cardiometabolic disease are at increased risk of morbidity and mortality from coronavirus disease 2019 (COVID-19) [1,2,3,4]. Beyond this direct consequence, changes in lifestyle in response to lockdown, social distancing, and the stress of the pandemic have led to worsening control of multiple risk factors among those with and at risk for cardiometabolic disease. Across the population, deleterious changes in physical activity, dietary patterns, alcohol intake, and smoking are also increasing the population-level risk of cardiometabolic disease. In this review, we summarize the evidence regarding changes in cardiometabolic risk due to the COVID-19 pandemic, with recommendations for how practitioners and policy makers may develop interventions to mitigate the potential consequences of these developments.
COVID-19 Has Disproportionately Impacted People with Cardiometabolic Disease
People with cardiometabolic disease, including those with obesity, diabetes, atherosclerotic cardiovascular disease, hypertension, and heart failure, are all at increased risk of COVID-19-related morbidity and mortality [1,2,3,4,5]. In a cohort of 7606 patients with COVID-19 from 88 hospitals in the USA enrolled in the American Heart Association (AHA) COVID-19 cardiovascular disease (CVD) registry, obese patients were more likely to be hospitalized with COVID-19, had increased risk for venous thromboembolism and mechanical ventilation, and overall higher mortality [1]. Individuals with other comorbidities are at similarly increased risk of mortality from COVID-19 including diabetes mellitus (nearly a two-fold increase in the odds of death) and heart failure (two- to three-fold increase in the odds of mortality) [6,7,8]. Other groups at increased risk include those with established cardiovascular disease. In one propensity-matched cohort of patients with COVID-19, the relative incidence of myocardial infarction among those with pre-existing atherosclerotic cardiovascular disease (ASCVD) was over five times that of those without ASCVD (annualized incidence density rate of 10.7% vs. 1.8%, p < 0.0002) [9].
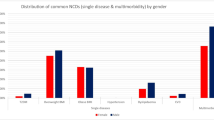
Given the high prevalence of hypertension, diabetes, obesity, and cardiovascular disease, in the USA, cardiometabolic disease has dramatically influenced the population-level consequences of the COVID-19 pandemic. In one estimate based on a national analysis of over 900,000 COVID-19 hospitalizations in the USA, an estimated 63.5% of hospitalizations were attributable to hypertension, diabetes mellitus, obesity, and heart failure (Fig. 1) [10•].

Attributable percentage of adult COVID-19 hospitalizations due to specific cardiometabolic risk factors [10•]. CKD, chronic kidney disease
COVID-19 Effects on Cardiometabolic Health
At the population level, the relationship between COVID-19 and cardiometabolic health is not a one-way street. As much as those with cardiometabolic disease have been disproportionately impacted by COVID-19, the COVID-19 pandemic itself has caused major adverse repercussions on the cardiometabolic health of the population.
Physical Activity
Physical activity dropped dramatically during the pandemic due to stay at home orders, closure of gyms and exercise facilities, increases in working from home, and social distancing with fear of contracting the virus [11,12,13]. One survey of 2140 adults in Brazil from June 2020 found dramatic declines in physical activity. Prior to the COVID-19 pandemic, 69% of the participants were self-reported as very active, which dipped to 39% during the social distancing period [14]. In another large, nationally representative sample of people in England, substantial reductions in the population-level activity were noted; among 74,430 respondents during the lockdown period in 2020, there was a 30% reduction in the odds of reporting any physical activity [15]. Decreases in physical activity have also been shown in pediatric cohorts based on survey data from parents [16].
Decreases in physical activity appear to be greatest among those already at highest risk, causing a cycle of negative consequences (Fig. 2). In an online survey of 7753 participants, the reported decline in physical activity seen during the pandemic was greater among individuals with underlying obesity (27.5% in total sample vs. 33.4% in participants with obesity) [11].

Key drivers and consequences of the detrimental effects of the COVID-19 pandemic on cardiometabolic health, along with opportunities to mitigate these effects. DM, diabetes mellitus; BP, blood pressure. Images from www.freepik.com
Beyond decreases in exercise, sedentary behavior also increased as daily activity dropped while people stayed at home. The impact of such sedentary lifestyles has significant cardiometabolic health consequences, including induction of insulin resistance, fat deposition, and decreased aerobic capacity [17]. The decline in physical activity during the lockdown period may also increase the risk of COVID-19 complications. In a study of 48,440 adult patients with COVID-19, those with consistent physical inactivity had a higher risk of hospitalization, ICU admission, and mortality due to COVID-19 compared with those meeting physical activity guideline recommendations [18].
Dietary Patterns and Weight
Another major impact of the COVID-19 pandemic on cardiometabolic health is through adverse changes in dietary behavior. One review of 12 studies looking at trajectories in dietary behaviors during the COVID-19 pandemic unveiled a notable rise in the consumption of carbohydrates, particularly ones with a high glycemic index (such as pizza, bread, and pastries) by up to 70% [19]. Multiple studies also found increases in snacking and numbers of meals during the pandemic, as well as increases in sweets, fried, and processed foods [20]. Mixed results were found regarding changes in consumption of fresh produce with some studies reporting increases, while others found decrease in fresh produce consumption during the pandemic [20].
Multiple studies have reported population-level weight gains during COVID-19 lockdowns across the globe, from the USA to Africa, Asia, and Europe [19,20,21,22,23,24]. In a cross-sectional survey of 10,545 adults in China, more than half reported weight gain during the COVID-19 pandemic, with about 19% of men and 16% of women noting a weight gain of over 2.5 kg [21]. Another study in Turkey (n = 1630 participants across the country) reported an average weight gain of 1.15 ± 6.10 kg over the first year of the pandemic. In this study, the strongest predictor of weight gain was self-reported increased amount of food compared to before the pandemic, demonstrating early impacts of changes in dietary patterns on cardiometabolic risk [23]. These changes in weight have affected individuals across the lifespan. In Korea, one study found that in the pediatric population, the proportion of overweight and obese children increased from 24.5% to 38.1% (p < 0.001) over only 1 year during the pandemic [25].
Control of Diabetes and Blood Pressure
Control of chronic cardiometabolic disease such as diabetes and hypertension also appears to have worsened during the pandemic [26,27,28]. A study from Italy demonstrated poor glycemic control after the lockdown period, evident by worsened HbA1c levels (mean 7.0% ± 0.8 to 7.3 ± 0.9) [27]. Similar findings were observed in a cohort of patients with diabetes in Turkey, with increased HbA1c levels more in diabetic than in sex-matched non-diabetic individuals (0.71% ± 1.38 vs. 0.02% ± 0.19) [28]. Notably, glucose control was also adversely impacted during the pandemic even in countries without national lockdown orders, such as Japan [29].
Similar observations were found for blood pressure control as demonstrated by a national study of 464,585 adults in the USA from an employer-sponsored wellness program. Compared to the pre-pandemic period (January 2019–March 2020), systolic blood pressure rose 1.1–2.5 mmHg during the pandemic period (April–December 2020) [30•]. In another study, there were modest increases in home blood pressure values in a population-based analysis of 72,706 participants enrolled in a digital hypertension control program [31]. While at an individual level, BP increases of 2–3 mmHg may be small, at a population level, even small changes in average SBP translate into meaningful increases in the total numbers of stroke and myocardial infarction [30•].
The reasons for worsening blood pressure and glycemic control are likely multifactorial and include decreased physical activity, dietary changes, increased alcohol intake, and decreased access to healthcare and medications. Whether, and how quickly, this improves post-pandemic remains to be seen.
Alcohol and Tobacco Use
The stress of the pandemic and adverse mental health consequences also led to increases in alcohol use, which both directly and indirectly impact cardiometabolic health [32,33,34,35]. One study evaluated changes in sales of alcohol during the pandemic using the Nielson National Consumer Panel, a longitudinal cohort comprising retail and purchase data in US households. Between the months of April and June, weighted alcohol sales surged from $7.10 billion in 2019 to $9.55 billion in 2020 (corresponding to a relative increase of 34.4%) [34]. This population-level increase in alcohol sales has been mirrored by studies showing individual-level increases in alcohol intake. In one survey of 1540 adults, increased frequency in alcohol consumption was shown for men and women across age groups, with an average increase of 14% from baseline [33]. Increases in alcohol intake worsens cardiometabolic health in a number of ways, from higher caloric intake and negative consequences on weight, to increases in blood pressure, to direct detrimental effects of excessive alcohol consumption on cardiovascular risk [36].
Along with alcohol use, smoking also increased during the pandemic. In the same Nielson National Consumer Panel that showed increases in alcohol use, cigarette sales increased by 13% from 2020 to 2021 [34, 37]. National spending data from the Alcohol and Tobacco Tax and Trade Bureau of the USA estimated that the pandemic-related increase in cigarette sales translates into an increase of four packs of cigarettes per person per year across the USA [37]. Beyond this increase in smoking, the pandemic has also witnessed fewer people attempting to quit smoking; the North American Quitline received 27% fewer calls in 2020 compared to 2019 [38].
The increases in alcohol and smoking behaviors during the pandemic may be some of the most challenging to combat. Given that both alcohol and smoking are habit forming, individuals’ alcohol and smoking levels may be more recalcitrant to change once the pandemic is behind us.
Access to Preventive Care and Care Utilization
COVID-19 lockdown and stay at home orders, combined with at times an over-stretched medical system, and patient fears of in-person medical visits have resulted in many people deferring or delaying routine medical care during the pandemic. In particular, preventive care visits significantly declined during the early period [39]. While telehealth has increased dramatically [40, 41], this has not fully offset the drop in in-person preventive visits. Furthermore, telehealth may not be optimal for cardiovascular health as labs are unavailable (e.g., lipid measurements and HbA1c) and many do not have access to a blood pressure cuff at home [42]. Finally, relying on telehealth may exacerbate disparities given inequity in access to broadband internet or telehealth-enabled health systems [43]. In one study, significant racial differences were seen in those with access to telehealth visits, with Black individuals being less likely to receive telehealth visits than other groups [44]. Care utilization issues also became evident in cardiac rehabilitation visits, as a reported 71% of on-site cardiac rehab programs in the USA halted their services during the pandemic [45].
In addition to delays in seeking routine medical care, a more alarming phenomenon was the delay in seeking care for acute conditions in need of emergent care, such as myocardial infarction and stroke. An analysis of Medicare beneficiaries showed that hospitalizations for myocardial infarction and stroke declined by 14% in 2020 compared to 2018 and 2019 with an even greater decline early in the pandemic (March and April 2020) [46]. Another systematic review found similar results with a decline in other acute cardiac conditions, including acute coronary syndromes by as much as 50% [47]. The repercussions of these delays and declines are an increase in out of hospital death and more advanced presentations of cardiovascular disease [48, 49]. The long-term sequelae of these advanced cardiovascular disease cases may be realized in the years to come.
Stress and Mental Health
Another consequence of the pandemic with pervasive health impact is the effect on mental health. This includes substantial increases in the rate of depression, particularly among those suffering job losses or other socioeconomic strain [50]. In one a global survey of 678 individuals, over 50% exhibited traits of anxiety, close to 60% suffered from signs of stress, and over half had features of depression [51]. A systematic review and meta-analysis estimated the prevalence of stress, anxiety, and depression during the pandemic to be ~ 30%, ~ 32%, and ~ 34%, respectively [52].
A pre-post pandemic study from the USA involving the National Health and Nutrition Examination Survey and a comparator cohort provides enhanced estimates of the impact of COVID-19 on mental health. Comparing data pre and post the pandemic onset, researchers found a threefold increase in the prevalence of depression symptoms during the pandemic [50]. The underlying reason for this increase is likely multifactorial and includes uncertainty and isolation associated with the pandemic, lockdowns, economic and job instability, loss of family and friends, personal illnesses, and pandemic-related fear. The consequences of stress, depression, and anxiety may worsen cardiometabolic health through decreased medication adherence, lower physical activity, poorer dietary patterns, and less engagement with cardiometabolic health behaviors [53,54,55,56,57,58,59,60].
Loss of Loved Ones, Wages, and Health Insurance
COVID-19 has resulted in over 900,000 deaths in the USA to date, with an estimated 7.2 million people affected by the loss of a family member as of December 2021 [61]. Loss of family members negatively impacts physical and mental health through bereavement and grief as well as loss of financial security [62]. As those at lower socioeconomic status are at increased risk for death from COVID-19, this further contributes to healthcare disparities by disproportionately impacting already vulnerable populations [63].
Beyond these deaths, high rates of job losses have also occurred during the pandemic. There were five million less jobs in September 2021 compared to February 2020, and the unemployment rate increased to 4.8% from 3.5% over the same interval. Among other repercussions, job loss directly impacts population health via loss of health insurance and an estimated 3.1 million people lost employer-sponsored health insurance between March and September 2020 [64]. With job loss also comes increased food insecurity, and a Vermont population survey noted a 33% increase in food insecurity with the pandemic onset [65]. The impacts of unemployment-related financial insecurity may also exacerbated health disparities. In one survey, Hispanic adults were at the greatest risk of food and housing insecurity and reported more psychosocial stress compared to other racial groups as a result [66].
Mitigating the Long-term Cardiovascular Consequences of the Pandemic
The declines in cardiometabolic health during the pandemic have the potential to cause long-term increases in cardiovascular disease at the population level. Concerningly, many of those who were impacted the most from the pandemic come from groups that are already suffering from disparities in cardiovascular health, including Black and Hispanic communities, those at low socioeconomic status, and those with the least access to healthcare including the un- and under-insured. Fortunately, numerous tools exist to address the changes in cardiometabolic health that resulted from the pandemic. Furthermore, technology and innovation that has been catalyzed by the pandemic (e.g., expansion in telemedicine) can also be leveraged to combat its consequences. Finally, policy changes are needed to help protect vulnerable populations both now and in the future.
Addressing Physical Inactivity and Declines in Exercise
Physicians should routinely ask their patients about their current activity levels and exercise habits, and remind patients of current guideline-recommended exercise targets. Recent American College of Cardiology (ACC)/AHA guidelines recommend adults participate in at least 150–300 min of moderate-intensity activity or 75–150 min of vigorous-intensity aerobic activity weekly [67]. For those who have gained weight during the pandemic, high-intensity exercise combined with high-load resistance can be effective to help with weight loss [68].
Beyond emphasizing recommendations, physicians can help patients recognize the personal benefits of physical activity, identify modifiable barriers to exercise, and set small, achievable goals to help patients change exercise habits [69]. Other strategies that physicians can implement include writing patients an exercise prescription using a FITT template—frequency, intensity, time, and type [70].
Many people do not have access to safe spaces for exercise or cannot afford expenses gym memberships. Fortunately, the pandemic did lead to an increase in resources to facilitate exercise at home, many of which are available at low cost or for free. One multinational survey noted a significant increase in online home exercise classes and an increase in walking and running [71]. Nevertheless, many exercise programs still require a membership fee and are therefore not available to those at highest risk. Whether offering free exercise facility membership or equipment improves physical activity or overall health remains unclear [72].
Weight Loss Strategies and Nutrition
Obesity is increasingly appreciated as a medical condition that requires multidisciplinary treatment approaches to support sustained changes in diet and lifestyle. Healthy weight loss and maintenance includes reduced dietary intake, regular physical activity, and behavior changes such as self-monitoring [73]. Both in-person and electronically delivered lifestyle intervention programs have been shown to lead to sustained weight loss after a year, including those delivered in-person with individual or group sessions. Lifestyle intervention programs include counseling for behavior changes on self-monitoring of food intake, goal-setting, and food environment stimulus control [74]. Nutritionists/registered dieticians can also be critical team members to help evaluate dietary patterns and provide evidence-based recommendations to patients. By necessity, there has been expanded use of telehealth-based nutrition counseling by dieticians, with generally favorable response [75]. Further expansion of telehealth nutrition services may fill a needed gap by increasing nutrition services accessibility to those with cardiometabolic risk factors.
For individuals with severe obesity, diet and lifestyle changes alone are often insufficient to lead to sustained, optimal weight loss. In these cases, surgery and medical therapies can be effective [76]. Only 3% of patients trying to lose weight from 2013 to 2016 reported using medications to assist with weight loss in one study [77]. However, new therapies have emerged for weight loss including the use of the glucagon-like peptide-1 receptor agonists (GLP-1RA) liraglutide and semaglutide. Both are FDA approved for weight loss, with or without T2DM. The recent Semaglutide Treatment Effect in People with Obesity (STEP) trials have demonstrated an impressive ~ 15% weight loss with the use of weekly injectable semaglutide [78]. Access to these medications is limited by both provider under-utilization of these therapies and lack of insurance coverage.
Enhancing Blood Pressure Control
The current paradigm of frequent in-office visits for blood pressure management and medication titration has failed to lead to adequate population-level blood pressure control. Even prior to the COVID-19 pandemic, only ~ 20% of those with hypertension achieved target blood pressure control [79]. Improving this and addressing pandemic-related increases in blood pressure will require innovation in the current treatment paradigm. One such strategy is a model that utilizes more in-home blood pressure measurement and less resource-intensive blood pressure management visits [80]. Fortunately, increases in telemedicine provide an opportunity to jumpstart this transition. Smartphone-enabled blood pressure monitoring has demonstrated similar blood pressure control success as regular in-office follow-up [81]. A shift to a multidisciplinary team-based monitoring at home with initial intensive monitoring may help improve blood pressure management. Finally, in the face of worsening dietary patterns during COVID-19, physicians should redouble efforts to remind patients about the importance of dietary interventions to lower blood pressure, including a low-sodium, high-potassium diet [82].
Smoking Cessation
Given the increase in tobacco use during the COVID-19 pandemic, it is imperative to inquire at every healthcare visit about tobacco use status as a “vital sign” per the AHA/ACC prevention guidelines [67], particularly noting new smokers and recidivism of those who quit. All current tobacco users should be strongly encouraged to quit and should be offered both behavioral and pharmacologic interventions [83]. Provider resources are available to increase providers’ comfort with prescribing these therapies, and are available at https://millionhearts.hhs.gov/files/Tobacco-Cessation-Action-Guide.pdf. Every individual in the USA have access to free national counseling services to assist with smoking cessation at 1–800-QUIT-NOW, which is also available in Spanish at 1–855-DÉJELO-YA (1–855-335–3569).
Technology and Adaptions in Care
Despite limitations of telehealth, there are numerous opportunities to leverage its strengths and to enhance telehealth practices [84]. The lack of ability to engage with care teams early in the pandemic likely exacerbated cardiometabolic decline, as there were missed opportunities for discussions around exercise, nutrition, and smoking. However, the rapid and almost unprecedented uptake of telehealth was understandably accompanied by shortcomings in standardization, assessment of laboratory and biometric data, and an understanding of best practices. In addition, telehealth could also exacerbate disparities in cardiometabolic health due to the digital divide in broadband access [85].
Nevertheless, the COVID-19 pandemic has been a catalyst for rapid advances in telehealth opportunities. Several groups have developed innovative ways to accommodate for the lack of in person assessment, such as describing creative ways to capture the physical examination [86]. Further, remote monitoring may assess vital signs and cardiac rhythms. Patients may involve family members in care and decrease time away from work. Finally, there are well-known disparities in rural health compared with urban areas, with lack of access to outpatient providers being one contributor [87]. In fact, only 9% of US physicians are currently in rural practice although 20% of the population lives in these areas [85]. Expansion of telehealth has the opportunity to partially fill this gap. Increased broadband access is an imperative to realize this potential for rural communities as well as for other disadvantaged populations. The CARES act did include $200 million to enhance telehealth access and the Federal Communications Commission also announced over $20 billion in funding to broadband access in rural communities.
Cardiac rehabilitation is grossly underutilized, with less than 20% of patients experiencing a myocardial infarction participating in these programs [88]. The lack of access to center-based cardiac rehabilitation during the pandemic accelerated the impetus for home-based programs. In fact, a Cochrane review of 23 randomized trials demonstrated similar outcomes including subsequent events, exercise capacity, and health-related quality of life with home- vs. center-based programs [89]. There is renewed momentum to harness the advances during COVID-19 to provide home-based cardiac rehabilitation as a viable option to expand its use among patients with CVD.
Health Policy and Communication
At the policy level, improving health insurance coverage can enhance prevention efforts, improve risk factor control, and narrow disparities in cardiometabolic health [90, 91]. Health insurance coverage for gig workers and the working poor with expansion of Medicaid, creation of another public healthcare option, or expansion of marketplace premium subsidies would allow for a significant proportion of Americans to access healthcare for preventive services. Insurance coverage of telehealth and telemonitoring facilitates care for those with difficulty commuting to appointments and expands sub-specialty care in rural areas [92,93,94]. As mentioned above, the CARES act efforts to enhance telehealth were a good start to promote telehealth and should continue to be prioritized in Congress. Focus should also remain on equitable access to telehealth through expansion of broadband internet access to all localities and individuals throughout the nation.
While well-intended, stay at home orders early in the pandemic likely contributed to delayed and deferred care for CVD prevention and cardiovascular emergencies. One study demonstrated rapid decline and rebound of myocardial infarction and heart failure hospitalizations mirroring State of Emergency and Reopening orders in a large health care network [95]. Patient surveys also revealed exaggerated fear about infection risk of hospitals and desire for guidance from their providers about when to go the emergency department [96]. These observations provide opportunities for the future where public declarations or emergency orders must be accompanied clear communication regarding the imperative for continuity of urgent and emergent care. Further, physicians should proactively discuss at each visit symptoms of concern, necessity to seek care for urgent medical conditions, and safety procedures in medical facilities [97••].
Conclusions: What About the Next Wave?
While we hope there will not be another pandemic, society and healthcare must prepare for one. We may take lessons learned from this pandemic and optimize our innovations in care, lifestyle approaches, and communication strategies for public health emergencies. Most importantly, we must work diligently to improve the cardiometabolic health of the population to create a more resilient and robust population to be able to withstand the challenges of future infectious waves. This work is even more prescient given the setbacks in cardiometabolic health during the COVID-19 pandemic and the adverse consequences of disparities in health laid bare by this wave.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Hendren NS, de Lemos JA, Ayers C, Das SR, Rao A, Carter S, Rosenblatt A, Walchok J, Omar W, Khera R, Hegde AA, Drazner MH, Neeland IJ, Grodin JL. Association of body mass index and age with morbidity and mortality in patients hospitalized with COVID-19: results from the American Heart Association COVID-19 Cardiovascular Disease Registry. Circulation. 2021;143:135–44.
Tartof SY, Qian L, Hong V, Wei R, Nadjafi RF, Fischer H, Li Z, Shaw SF, Caparosa SL, Nau CL, Saxena T, Rieg GK, Ackerson BK, Sharp AL, Skarbinski J, Naik TK, Murali SB. Obesity and mortality among patients diagnosed with COVID-19: results from an integrated health care organization. Ann Intern Med. 2020;173:773–81.
Lighter J, Phillips M, Hochman S, Sterling S, Johnson D, Francois F, Stachel A. Obesity in patients younger than 60 years is a risk factor for COVID-19 hospital admission. Clin Infect Dis. 2020;71:896–7.
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE, Curtis HJ, Mehrkar A, Evans D, Inglesby P, Cockburn J, McDonald HI, MacKenna B, Tomlinson L, Douglas IJ, Rentsch CT, Mathur R, Wong AYS, Grieve R, Harrison D, Forbes H, Schultze A, Croker R, Parry J, Hester F, Harper S, Perera R, Evans SJW, Smeeth L, Goldacre B. Factors associated with COVID-19-related death using OpenSAFELY. Nature. 2020;584:430–6.
Svensson P, Hofmann R, Häbel H, Jernberg T, Nordberg P. Association between cardiometabolic disease and severe COVID-19: a nationwide case-control study of patients requiring invasive mechanical ventilation. BMJ Open. 2021;11: e044486.
Lim S, Bae JH, Kwon HS, Nauck MA. COVID-19 and diabetes mellitus: from pathophysiology to clinical management. Nat Rev Endocrinol. 2021;17:11–30.
Barron E, Bakhai C, Kar P, Weaver A, Bradley D, Ismail H, Knighton P, Holman N, Khunti K, Sattar N, Wareham NJ, Young B, Valabhji J. Associations of type 1 and type 2 diabetes with COVID-19-related mortality in England: a whole-population study. Lancet Diabetes Endocrinol. 2020;8:813–22.
Sokolski M, Trenson S, Sokolska JM, D’Amario D, Meyer P, Poku NK, Biering-Sørensen T, Højbjerg Lassen MC, Skaarup KG, Barge-Caballero E, Pouleur AC, Stolfo D, Sinagra G, Ablasser K, Muster V, Rainer PP, Wallner M, Chiodini A, Heiniger PS, Mikulicic F, Schwaiger J, Winnik S, Cakmak HA, Gaudenzi M, Mapelli M, Mattavelli I, Paul M, Cabac-Pogorevici I, Bouleti C, Lilliu M, Minoia C, Dauw J, Costa J, Celik A, Mewton N, Montenegro CEL, Matsue Y, Loncar G, Marchel M, Bechlioulis A, Michalis L, Dörr M, Prihadi E, Schoenrath F, Messroghli DR, Mullens W, Lund LH, Rosano GMC, Ponikowski P, Ruschitzka F, Flammer AJ. Heart failure in COVID-19: the multicentre, multinational PCHF-COVICAV registry. ESC Heart Failure. 2021;8:4955–67.
Myers KD, Wilemon K, McGowan MP, Howard W, Staszak D, Rader DJ. COVID-19 associated risks of myocardial infarction in persons with familial hypercholesterolemia with or without ASCVD. Am J Prev Cardiol. 2021;7: 100197.
O’Hearn M, Liu J, Cudhea F, Micha R, Mozaffarian D. Coronavirus disease 2019 hospitalizations attributable to cardiometabolic conditions in the United States: a comparative risk assessment analysis. J Am Heart Assoc. 2021;10:e019259 Findings from this study indicate that major cardiometabolic conditions were key drivers leading to COVID-19 hospitalizations. This highlights the importance of continued public health prevention strategies at such times as the COVID-19 pandemic.
Flanagan EW, Beyl RA, Fearnbach SN, Altazan AD, Martin CK, Redman LM. The impact of COVID-19 stay-at-home orders on health behaviors in adults. Obesity (Silver Spring, Md). 2021;29:438–45.
Barr-Anderson DJ, Hazzard VM, Hahn SL, Folk AL, Wagner BE and Neumark-Sztainer D. Stay-at-home orders during COVID-19: the influence on physical activity and recreational screen time change among diverse emerging adults and future implications for health promotion and the prevention of widening health disparities. Int J Environ Res Public Health. 2021;18.
Rapisarda V, Loreto C, De Angelis L, Simoncelli G, Lombardo C, Resina R, Mucci N, Matarazzo A, Vimercati L, Ledda C. Home working and physical activity during SARS-CoV-2 pandemic: a longitudinal cohort study. Int J Environ Res Public Health 2021;18.
Puccinelli PJ, da Costa TS, Seffrin A, de Lira CAB, Vancini RL, Nikolaidis PT, Knechtle B, Rosemann T, Hill L, Andrade MS. Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: an internet-based survey. BMC Public Health. 2021;21:425.
Strain T, Sharp SJ, Spiers A, Price H, Williams C, Fraser C, Brage S, Wijndaele K, Kelly P. Population level physical activity before and during the first national COVID-19 lockdown: a nationally representative repeat cross-sectional study of 5 years of Active Lives data in England. Lancet Reg Health Eur. 2022;12: 100265.
Dunton GF, Do B, Wang SD. Early effects of the COVID-19 pandemic on physical activity and sedentary behavior in children living in the U.S. BMC Public Health. 2020;20:1351.
Narici M, Vito G, Franchi M, Paoli A, Moro T, Marcolin G, Grassi B, Baldassarre G, Zuccarelli L, Biolo G, di Girolamo FG, Fiotti N, Dela F, Greenhaff P, Maganaris C. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur J Sport Sci. 2021;21:614–35.
Sallis R, Young DR, Tartof SY, Sallis JF, Sall J, Li Q, Smith GN, Cohen DA. Physical inactivity is associated with a higher risk for severe COVID-19 outcomes: a study in 48 440 adult patients. Br J Sports Med. 2021;55:1099–105.
Zupo R, Castellana F, Sardone R, Sila A, Giagulli VA, Triggiani V, Cincione RI, Giannelli G and De Pergola G. Preliminary trajectories in dietary behaviors during the COVID-19 pandemic: a public health call to action to face obesity. Int J Environ Res Public Health 2020;17.
Bennett G, Young E, Butler I, Coe S. The impact of lockdown during the COVID-19 outbreak on dietary habits in various population groups: a scoping review. Front Nutr. 2021;8: 626432.
Xu X, Yan AF, Wang Y, Shi Z. Dietary patterns and changes in weight status among Chinese men and women during the COVID-19 pandemic. Front Public Health. 2021;9: 709535.
Cena H, Fiechtner L, Vincenti A, Magenes VC, De Giuseppe R, Manuelli M, Zuccotti GV and Calcaterra V. COVID-19 pandemic as risk factors for excessive weight gain in pediatrics: the role of changes in nutrition behavior. A narrative review. Nutrients. 2021;13.
Onal HY, Bayram B, Yuksel A. Factors associated with the weight change trend in the first year of the COVID-19 pandemic: the case of Turkey. Nurs Res Pract. 2021;15:S53-s69.
Madalı B, Alkan ŞB, Örs ED, Ayrancı M, Taşkın H, Kara HH. Emotional eating behaviors during the COVID-19 pandemic: a cross-sectional study. Clin Nutr ESPEN. 2021;46:264–70.
Gwag SH, Oh YR, Ha JW, Kang E, Nam HK, Lee Y, Rhie YJ and Lee KH. Weight changes of children in 1 year during COVID-19 pandemic. J Pediatr Endocrinol Metab: JPEM. 2021.
Endo K, Miki T, Itoh T, Kubo H, Ito R, Ohno K, Hotta H, Kato N, Matsumoto T, Kitamura A, Tamayama M, Wataya T, Yamaya A, Ishikawa R, Ooiwa H. Impact of the COVID-19 pandemic on glycemic control and blood pressure control in patients with diabetes in Japan. Intern Med (Tokyo, Japan). 2022;61:37–48.
Biamonte E, Pegoraro F, Carrone F, Facchi I, Favacchio G, Lania AG, Mazziotti G, Mirani M. Weight change and glycemic control in type 2 diabetes patients during COVID-19 pandemic: the lockdown effect. Endocrine. 2021;72:604–10.
Karatas S, Yesim T, Beysel S. Impact of lockdown COVID-19 on metabolic control in type 2 diabetes mellitus and healthy people. Prim Care Diabetes. 2021;15:424–7.
Tanji Y, Sawada S, Watanabe T, Mita T, Kobayashi Y, Murakami T, Metoki H, Akai H. Impact of COVID-19 pandemic on glycemic control among outpatients with type 2 diabetes in Japan: a hospital-based survey from a country without lockdown. Diabetes Res Clin Pract. 2021;176: 108840.
Laffin LJ, Kaufman HW, Chen Z, Niles JK, Arellano AR, Bare LA, Hazen SL. Rise in blood pressure observed among US adults during the COVID-19 pandemic. Circulation. 2022;145:235–7 This study highlights a modest population-level increase in blood pressure during the COVID-19 pandemic. This underscores the continued need for public health interventions during a pandemic to avoid long-term detrimental health effects.
Shah NP, Clare RM, Chiswell K, Navar AM, Shah BR and Peterson ED. Trends of blood pressure control in the U.S. during the COVID-19 pandemic. Am Heart J. 2021.
Dogan-Sander E, Kohls E, Baldofski S, Rummel-Kluge C. More depressive symptoms, alcohol and drug consumption: increase in mental health symptoms among university students after one year of the COVID-19 pandemic. Front Psych. 2021;12: 790974.
Pollard MS, Tucker JS, Green HD Jr. Changes in adult alcohol use and consequences during the COVID-19 pandemic in the US. JAMA Netw Open. 2020;3: e2022942.
Lee BP, Dodge JL, Leventhal A, Terrault NA. Retail alcohol and tobacco sales during COVID-19. Ann Intern Med. 2021;174:1027–9.
MacKillop J, Cooper A, Costello J. National retail sales of alcohol and cannabis during the COVID-19 pandemic in Canada. JAMA Netw Open. 2021;4: e2133076.
Bermúdez V, Martínez MS, Chávez-Castillo M, Olivar LC, Morillo J, Mejías JC, Rojas M, Salazar J, Rojas J, Añez R, Cabrera M. Relationship between alcohol consumption and components of the metabolic syndrome in adult population from Maracaibo City Venezuela. Adv Prev Med. 2015;2015: 352547.
Asare S, Majmundar A, Islami F, Bandi P, Fedewa S, Westmaas LJ and Nargis N. Changes in cigarette sales in the United States during the COVID-19 pandemic. Ann Internal Med. 2021.
The Lancet Respiratory M. Pandemic fans the flames of smoking and health inequity. Lancet Respir Med. 2021;9:435.
Cortez C, Mansour O, Qato DM, Stafford RS, Alexander GC. Changes in short-term, long-term, and preventive care delivery in US office-based and telemedicine visits during the COVID-19 pandemic. JAMA Health Forum. 2021;2:e211529–e211529.
Rossano A, Crijns T, Ring D and Reichenberg J. Clinician preferences for current and planned future use of telemedicine. Telemed J E-Health. 2022.
Balut MD, Wyte-Lake T, Steers WN, Chu K, Dobalian A, Ziaeian B, Heyworth L, Der-Martirosian C. Expansion of telemedicine during COVID-19 at a VA specialty clinic. Healthcare (Amsterdam, Netherlands). 2021;10: 100599.
Ismail H, Marshall VD, Patel M, Tariq M and Mohammad RA. The impact of the COVID-19 pandemic on medical conditions and medication adherence in people with chronic diseases. J Am Pharm Assoc. 2021.
Ng BP, Park C, Silverman CL, Eckhoff DO, Guest JC and Díaz DA. Accessibility and utilisation of telehealth services among older adults during COVID-19 pandemic in the United States. Health & social care in the community. 2022.
Eberly LA, Khatana SAM, Nathan AS, Snider C, Julien HM, Deleener ME, Adusumalli S. Telemedicine outpatient cardiovascular care during the COVID-19 pandemic: bridging or opening the digital divide? Circulation. 2020;142:510–2.
Khanna S and Harzand A. Preventive cardiology in the digital and COVID-19 era: a brave new world within the Veterans Health Administration. Healthcare (Basel, Switzerland). 2021;9.
Stewart KA, Blue L, Kranker K, Nelson S, McCall N, Markovich P, Peterson GG. Hospital use for myocardial infarction and stroke among Medicare beneficiaries from March to December 2020. JAMA Cardiol. 2021;6:1340–2.
Kiss P, Carcel C, Hockham C, Peters SAE. The impact of the COVID-19 pandemic on the care and management of patients with acute cardiovascular disease: a systematic review. Eur Heart J Qual Care Clin Outcomes. 2021;7:18–27.
Evans MC, Steinberg DH, Rhodes JF, Tedford RJ. Ventricular septal defect complicating delayed presentation of acute myocardial infarction during COVID-19 lockdown: a case report. Eur Heart J Case Rep. 2021;5:ytab027.
Chhetry M, Bhatt R, Tehrani NH, Avgerinos DV, Mack CA, Lang SJ and Dai X. Delayed treatment of acute myocardial infarction with ventricular septal rupture due to patient fear during the COVID-19 pandemic. Texas Heart Inst J. 2021;48.
Ettman CK, Abdalla SM, Cohen GH, Sampson L, Vivier PM, Galea S. Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Netw Open. 2020;3: e2019686.
Shah SMA, Mohammad D, Qureshi MFH, Abbas MZ, Aleem S. Prevalence, psychological responses and associated correlates of depression, anxiety and stress in a global population, during the coronavirus disease (COVID-19) pandemic. Community Ment Health J. 2021;57:101–10.
Salari N, Hosseinian-Far A, Jalali R, Vaisi-Raygani A, Rasoulpoor S, Mohammadi M, Rasoulpoor S, Khaledi-Paveh B. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Glob Health. 2020;16:57.
Pearsall R, Shaw RJ, McLean G, Connolly M, Hughes KA, Boyle JG, Park J, Smith DJ, Mackay D. Health screening, cardiometabolic disease and adverse health outcomes in individuals with severe mental illness. BJPsych Open. 2019;5: e97.
Ringen PA, Faerden A, Antonsen B, Falk RS, Mamen A, Rognli EB, Solberg DK, Andreassen OA, Martinsen EW. Cardiometabolic risk factors, physical activity and psychiatric status in patients in long-term psychiatric inpatient departments. Nord J Psychiatry. 2018;72:296–302.
Hare DL, Toukhsati SR, Johansson P, Jaarsma T. Depression and cardiovascular disease: a clinical review. Eur Heart J. 2014;35:1365–72.
Nicholson A, Kuper H, Hemingway H. Depression as an aetiologic and prognostic factor in coronary heart disease: a meta-analysis of 6362 events among 146 538 participants in 54 observational studies. Eur Heart J. 2006;27:2763–74.
Barefoot JC, Schroll M. Symptoms of depression, acute myocardial infarction, and total mortality in a community sample. Circulation. 1996;93:1976–80.
Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet (London, England). 2004;364:937–52.
Lespérance F, Frasure-Smith N, Talajic M, Bourassa MG. Five-year risk of cardiac mortality in relation to initial severity and one-year changes in depression symptoms after myocardial infarction. Circulation. 2002;105:1049–53.
Rosengren A, Hawken S, Ounpuu S, Sliwa K, Zubaid M, Almahmeed WA, Blackett KN, Sitthi-amorn C, Sato H, Yusuf S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11119 cases and 13648 controls from 52 countries (the INTERHEART study): case-control study. Lancet (London, England). 2004;364:953–62.
Verdery AM, Smith-Greenaway E, Margolis R, Daw J. Tracking the reach of COVID-19 kin loss with a bereavement multiplier applied to the United States. Proc Natl Acad Sci USA. 2020;117:17695–701.
Ott CH. The impact of complicated grief on mental and physical health at various points in the bereavement process. Death Stud. 2003;27:249–72.
Ellis J, Dowrick C, Lloyd-Williams M. The long-term impact of early parental death: lessons from a narrative study. J R Soc Med. 2013;106:57–67.
Woodbury PFaSA. "Update: how many Americans have lost jobs with employer health coverage during the pandemic?" To the Point (blog), Commonwealth Fund, Jan 11, 2021.
Niles MT, Bertmann F, Belarmino EH, Wentworth T, Biehl E and Neff R. The early food insecurity impacts of COVID-19. Nutrients. 2020;12.
McKnight-Eily LR, Okoro CA, Strine TW, Verlenden J, Hollis ND, Njai R, Mitchell EW, Board A, Puddy R, Thomas C. Racial and ethnic disparities in the prevalence of stress and worry, mental health conditions, and increased substance use among adults during the COVID-19 pandemic - United States, April and May 2020. MMWR Morb Mortal Wkly Rep. 2021;70:162–6.
Arnett DK, Blumenthal RS, Albert MA, Buroker AB, Goldberger ZD, Hahn EJ, Himmelfarb CD, Khera A, Lloyd-Jones D, McEvoy JW, Michos ED, Miedema MD, Muñoz D, Smith SC Jr, Virani SS, Williams KA Sr, Yeboah J, Ziaeian B. 2019 ACC/AHA guideline on the primary prevention of cardiovascular disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2019;140:e596–646.
O’Donoghue G, Blake C, Cunningham C, Lennon O, Perrotta C. What exercise prescription is optimal to improve body composition and cardiorespiratory fitness in adults living with obesity? A network meta-analysis. Obes Rev. 2021;22: e13137.
Hooker S, Punjabi A, Justesen K, Boyle L, Sherman MD. Encouraging health behavior change: eight evidence-based strategies. Fam Pract Manag. 2018;25:31–6.
Phillips EM, Kennedy MA. The exercise prescription: a tool to improve physical activity. PM R. 2012;4:818–25.
Faulkner J, O’Brien WJ, McGrane B, Wadsworth D, Batten J, Askew CD, Badenhorst C, Byrd E, Coulter M, Draper N, Elliot C, Fryer S, Hamlin MJ, Jakeman J, Mackintosh KA, McNarry MA, Mitchelmore A, Murphy J, Ryan-Stewart H, Saynor Z, Schaumberg M, Stone K, Stoner L, Stuart B, Lambrick D. Physical activity, mental health and well-being of adults during initial COVID-19 containment strategies: a multi-country cross-sectional analysis. J Sci Med Sport. 2021;24:320–6.
King HA, Gierisch JM, Williams JW Jr, Maciejewski ML. VA evidence-based synthesis program reports. Effects of health plan-sponsored fitness center benefits on physical activity, health outcomes, and health care costs and utilization: a systematic review. Washington (DC): Department of Veterans Affairs (US); 2012.
Ramage S, Farmer A, Eccles KA, McCargar L. Healthy strategies for successful weight loss and weight maintenance: a systematic review. Appl Physiol Nutr Metab. 2014;39:1–20.
Bray GA, Ryan DH. Evidence-based weight loss interventions: individualized treatment options to maximize patient outcomes. Diabetes Obes Metab. 2021;23(Suppl 1):50–62.
Brunton C, Arensberg MB, Drawert S, Badaracco C, Everett W and McCauley SM. Perspectives of registered dietitian nutritionists on adoption of telehealth for nutrition care during the COVID-19 pandemic. Healthcare (Basel, Switzerland). 2021;9.
Cohen JB, Gadde KM. Weight loss medications in the treatment of obesity and hypertension. Curr Hypertens Rep. 2019;21:16.
Gadde KM, Atkins KD. The limits and challenges of antiobesity pharmacotherapy. Expert Opin Pharmacother. 2020;21:1319–28.
Wilding JPH, Batterham RL, Calanna S, Davies M, Van Gaal LF, Lingvay I, McGowan BM, Rosenstock J, Tran MTD, Wadden TA, Wharton S, Yokote K, Zeuthen N, Kushner RF. Once-weekly semaglutide in adults with overweight or obesity. N Engl J Med. 2021;384:989.
Tsao CW, Aday AW, Almarzooq ZI, Alonso A, Beaton AZ, Bittencourt MS, Boehme AK, Buxton AE, Carson AP, Commodore-Mensah Y, Elkind MSV, Evenson KR, Eze-Nliam C, Ferguson JF, Generoso G, Ho JE, Kalani R, Khan SS, Kissela BM, Knutson KL, Levine DA, Lewis TT, Liu J, Loop MS, Ma J, Mussolino ME, Navaneethan SD, Perak AM, Poudel R, Rezk-Hanna M, Roth GA, Schroeder EB, Shah SH, Thacker EL, VanWagner LB, Virani SS, Voecks JH, Wang NY, Yaffe K, Martin SS. Heart disease and stroke statistics-2022 update: a report from the American Heart Association. Circulation. 2022:Cir0000000000001052.
Ho PM, Rumsfeld JS. Beyond inpatient and outpatient care: alternative model for hypertension management. BMC Public Health. 2006;6:257.
Treskes RW, van Winden LAM, van Keulen N, van der Velde ET, Beeres S, Atsma DE, Schalij MJ. Effect of smartphone-enabled health monitoring devices vs regular follow-up on blood pressure control among patients after myocardial infarction: a randomized clinical trial. JAMA Netw Open. 2020;3: e202165.
Juraschek SP, Miller ER 3rd, Weaver CM, Appel LJ. Effects of sodium reduction and the DASH diet in relation to baseline blood pressure. J Am Coll Cardiol. 2017;70:2841–8.
Barua RS, Rigotti NA, Benowitz NL, Cummings KM, Jazayeri M-A, Morris PB, Ratchford EV, Sarna L, Stecker EC, Wiggins BS. 2018 ACC expert consensus decision pathway on tobacco cessation treatment. J Am Coll Cardiol. 2018;72:3332–65.
Patel P, Dhindsa D, Eapen DJ, Khera A, Gulati M, Stone NJ, Yancy CW, Rumsfeld JS, Sperling LS. Optimizing the potential for telehealth in cardiovascular care (in the era of COVID-19): time will tell. Am J Med. 2021;134:945–51.
Al Rifai M, Shapiro MD, Sayani S, Gulati M, Levine G, Rodriguez F, Mahtta D, Khera A, Petersen LA, Virani SS. Racial and geographic disparities in internet use in the United States among patients with atherosclerotic cardiovascular disease. Am J Cardiol. 2020;134:146–7.
Kelly SA, Schesing KB, Thibodeau JT, Ayers CR, Drazner MH. Feasibility of remote video assessment of jugular venous pressure and implications for telehealth. JAMA Cardiol. 2020;5:1194–5.
Harrington RA, Califf RM, Balamurugan A, Brown N, Benjamin RM, Braund WE, Hipp J, Konig M, Sanchez E, Joynt Maddox KE. Call to action: rural health: a presidential advisory from the American Heart Association and American Stroke Association. Circulation. 2020;141:e615–44.
Thomas RJ, Beatty AL, Beckie TM, Brewer LC, Brown TM, Forman DE, Franklin BA, Keteyian SJ, Kitzman DW, Regensteiner JG, Sanderson BK, Whooley MA. Home-based cardiac rehabilitation: a scientific statement from the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. Circulation. 2019;140:e69–89.
Anderson L, Sharp GA, Norton RJ, Dalal H, Dean SG, Jolly K, Cowie A, Zawada A, Taylor RS. Home-based versus centre-based cardiac rehabilitation. Cochrane Database Syst Rev. 2017;6:Cd007130.
Brooks EL, Preis SR, Hwang SJ, Murabito JM, Benjamin EJ, Kelly-Hayes M, Sorlie P, Levy D. Health insurance and cardiovascular disease risk factors. Am J Med. 2010;123:741–7.
Li S, Bruen BK, Lantz PM, Mendez D. Impact of health insurance expansions on nonelderly adults with hypertension. Prev Chronic Dis. 2015;12:E105.
De Simone V, Guarise P, Guardalben S, Padovani N, Tondelli S, Sandrini D, Visentin E, Zanotto G. Telecardiology during the COVID-19 pandemic: past mistakes and future hopes. Am J Cardiovasc Dis. 2020;10:34–47.
Hincapié MA, Gallego JC, Gempeler A, Piñeros JA, Nasner D, Escobar MF. Implementation and usefulness of telemedicine during the COVID-19 pandemic: a scoping review. J Prim Care Commun Health. 2020;11:2150132720980612.
Zachrison KS, Boggs KM, Hayden EM, Espinola JA, Camargo CA Jr. Understanding barriers to telemedicine implementation in rural emergency departments. Ann Emerg Med. 2020;75:392–9.
Arora S, Hendrickson MJ, Mazzella AJ, Vaduganathan M, Chang PP, Rossi JS, Qamar A, Pandey A, Vavalle JP, Weickert TT, Strassle PD, Yeung M, Stouffer GA. Effect of government-issued state of emergency and reopening orders on cardiovascular hospitalizations during the COVID-19 pandemic. Am J Prevent Cardiol 2021;6
Wong LE HJ, Langness S, Murrell KL, Iris P, Sammann A. Where are all the patients? Addressing COVID-19 fear to encourage sick patients to seek emergency care. NEJM catalyst - Innovations in Care Delivery May 2020
Khera A, Baum SJ, Gluckman TJ, Gulati M, Martin SS, Michos ED, Navar AM, Taub PR, Toth PP, Virani SS, Wong ND, Shapiro MD. Continuity of care and outpatient management for patients with and at high risk for cardiovascular disease during the COVID-19 pandemic: a scientific statement from the American Society for Preventive Cardiology. Am J Prevent Cardiol. 2020;1:100009 This scientific statement from the American Society of Preventive Cardiology proposes several important strategies to ensure continuity of care during the COVID-19 pandemic, particularly for patients with or at high risk for cardiovascular disease.
Acknowledgements
Dr. Kolkailah was supported by the National Heart, Lung, and Blood Institute of the National Institutes of Health under Award Number T32HL125247. The content is solely the responsibility of the authors and does not necessarily represent the official view of the National Institutes of Health.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Navar reports grant support from BMS, Esperion, and Janssen; and consulting for Amarin, Amgen, AstraZeneca, BI, Bayer, CSL, Esperion, Janssen, Lilly, Sanofi, Regeneron, NovoNordisk, Novartis, The Medicines Company, New Amsterdam, Cerner, 80Bio, and Pfizer. Dr. Navar also reports leadership or fiduciary role in the American Society for Preventive Cardiology, the National Forum, and JAMA Cardiology. Dr. Khera reports leadership or fiduciary role in the American Society for Preventive Cardiology Board. The other authors declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
This article is part of the Topical Collection on Coronary Heart Disease
Rights and permissions
About this article

Cite this article
Kolkailah, A.A., Riggs, K., Navar, A.M. et al. COVID-19 and Cardiometabolic Health: Lessons Gleaned from the Pandemic and Insights for the Next Wave. Curr Atheroscler Rep 24, 607–617 (2022). https://doi.org/10.1007/s11883-022-01033-7
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11883-022-01033-7