
Abstract
Introduction
Single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) is a safe and effective technique with good short- and mid-term weight control and associated medical problems remission for patients with a body mass index (BMI) > 45 kg/m2. The aim of this study was to analyze patient-reported symptoms, specifically symptomatic gastroesophageal reflux disease symptoms (GERD), depositional habit, and quality of life (QOL) following SADI-S, using telemedicine and validated tests.
Methods
A prospective unicentric cross-sectional study was conducted including all patients submitted to SADI-S in the University Hospital of Bellvitge from May 2014 to September 2019. A baseline control group was composed of 67 patients who were planning to undergo SADI-S in the following 4 months. Patients were divided into four groups: pre-SADIS, < 2 years, 2–3 years, and > 3 years after surgery. The information gathered via a telematic questionnaire was analyzed and compared with its presence in patients’ clinical history derived from the last presential visit.
Results
The response rate to telematic tests was 86.9%. The mean BMI exhibited significant differences depending on the moment of evaluation: 50.8 kg/m2, 30.0 kg/m2, 31.1 kg/m2, and 32.7 kg/m2 at pre-SADIS, < 2, 2–3, and > 3 years follow-up, respectively (p < 0.001). The proportion of GERD symptoms increased over time (17.9%, 18.8%, 26.9%, and 30.2%, p = 0.320). After SADIS, the percentage of patients with loose stools was progressively higher (17.4% vs 25.4% vs 30.2%, p = 0.04).
Patients with < 2-year follow-up presented an improvement in both physical component (PCS) and mental component (MCS) summaries compared to the baseline group (PCS = 51.3, and MCS = 49.4). The mean BMI of patients with PCS ≥ 50 was 31.9 kg/m2, compared with 41.7 kg/m2 in the PCS < 50 group (p < 0.001). In the MCS ≥ 50 group, there were more patients with a BMI < 35 kg/m2 than the MCS < 50 group (66.7% vs 48.7%, p = 0.004).
Telematic follow-up offered a more systemic and detailed information: in the last presential visit only, 13.9% of patients had complete data regarding weight evolution, remission of associated medical problems, GERD symptoms, and depositional habit in comparison with the 82.9% of patients with telematic follow-up (p < 0.001).
Conclusion
Weight control is the main factor related to long-term QOL after SADI-S. The incidence of GERD symptoms and diarrhea was up to 30% in patients with > 3-year follow-up. Monitoring postoperative patient-related symptoms with validated objective tests seems a feasible and useful resource for the long-term follow-up of patients submitted to SADI-S.
Graphical Abstract

Similar content being viewed by others

Introduction
Single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) is a safe and effective technique that has shown good short- and mid-term weight control and associated medical problems remission for patients with a body mass index (BMI) > 45 kg/m2 minimizing the risk of insufficient weight loss or weight regain in the long term [1,2,3,4,5,6]. Classic complications of hypoabsorptive procedures like hypoproteinemia and persistent diarrhea have been described with the 200-cm common limb SADI-S; but their incidence dropped with the 250-cm and 300-cm SADI-S [6, 7]. The omega reconstruction of SADIS, despite the preserving of pylorus, leads to a hypothetical risk of biliary reflux which continues to be one of the main arguments against this technique. Most series report this complication as anecdotical or even absent [1,2,3,4,5,6,7]; however, most of these studies do not perform an objective and systematical evaluation of the incidence of biliary reflux symptoms and do not consider its influence on patients’ quality of life (QOL).
In our previous experience with SADI-S technique, a 6.5% rate of symptomatic gastroesophageal reflux disease (GERD) was found, with not a single case of persistent diarrhea or hypoalbuminemia [7,8,9]. However, data was retrospectively obtained from standard follow-up and not confirmed by validated tests. Besides, an objective information about QOL was not reported.
During the COVID-19 pandemic, most of the presential follow-up visits were replaced by telephone consultations. This inconvenience allowed the healthcare professionals to explore different strategies to improve the accuracy of patient’s evaluation. Telemedicine became a complementary and feasible help to obtain objective information about patients’ current state [10].
The aim of this study was to analyze patient-reported symptoms, specifically GERD symptoms, depositional habit, and QOL following SADI-S, using telemedicine and validated tests. As a secondary aim, the influence of factors such as weight loss, associated medical problems remission, GERD symptoms, or depositional habit on patients’ QOL was evaluated. Finally, we compared the information obtained by telematic tests with that reported in the medical history derived from patients’ last presential visit.
Material and Methods
Study Design, Patients, and Data Source
A prospective unicentric cross-sectional study was conducted including all patients submitted to SADI-S, either directly or as a two-step procedure, in the bariatric and metabolic surgical unit of the University Hospital of Bellvitge from May 2014 to September 2019. To obtain a baseline control group, we included 67 patients who fulfilled indication criteria and had previously signed the informed consent to undergo SADI-S in the following 4 months. Patients who were exitus or had needed a revisional surgery after SADI-S before the study had started were excluded. To evaluate the chronological evolution of study variables, patients were divided in four groups: pre-SADIS, < 2 years, 2–3 years, and > 3 years after surgery.
Patients were contacted by telephone and were informed about the study. Those who accepted to participate received an email with a link to a telematic questionnaire composed by validated tests. Patients who did not respond to the questionnaire after a month were sent another email as a reminder. Finally, in case they had not yet responded to the survey, patients were recontacted by phone.
Data obtained telematically were integrated into our prospectively maintained database. Besides, the information gathered telematically in patients submitted to SADI-S was compared with its presence in patients’ clinical history derived from last presential visit.
Study Outcomes and Definitions
Primary outcomes were SF-36 physical and mental component scores (PCS and MCS), percentage of patients with a GERD-Q score ≥ 8, daily depositional frequency, and stool constitution determined by Bristol stool chart.
The SF-36 test is a validated questionnaire that consists of 36 multiple choice questions included in eight dimensions of QOL that can be factor-analyzed and reduced in two summary components: Physical Component Summary (PCS) and Mental Component Summary (MCS) [11]. Using these results, a substudy dividing the whole cohort of patients in two different groups considering a cut-off point of 50 for both PCS and MCS was performed compared with the average Spanish population (mean = 50, standard deviation = 10) [12, 13]. The GERD-Q test was used to assess GERD symptoms [14]. A GERD-Q score > 8 has been established as the cut-off score with greater sensitivity and specificity for the diagnosis of esophagitis [15] and exclude functional pyrosis [16]. Bristol questionnaire was used to identify patients with altered bowel movements being Bristol ≤ 2 for constipation and Bristol ≥ 5 for diarrhea [17].
Secondary outcomes were adequate weight control, expressed as proportion of patients with excess weight lost (EWL%) ≥ 50%; and BMI < 35 kg/m2; and remission of associated medical problems, such as type 2 diabetes (T2D), hypertension (HTN), dyslipidemia (DLP), and obstructive sleep apnea (OSA). EWL% was calculated taking as reference an ideal BMI of 25 kg/m2. Remission of associated medical problems was defined as complete withdrawal of all specific treatment by the treating physician.
Statistical Analysis
Continuous variables were expressed as mean and standard deviation. Categorical variables were described as its absolute value and percentage. To evaluate differences between groups parametric tests as χ2 for categorical variables and analysis of variance or Student’s t for continuous variables depending on the number of comparison groups were used. McNemar’s test was used to compare the grade of information gathered telematically with the last report in patients’ history. A p-value < 0.05 was considered significant. Statistics were analyzed with Stata Statistics Version 16 computer software.
Results
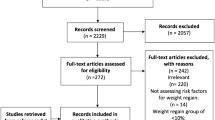
A total of 301 patients fulfilled the inclusion criteria: 234 submitted to SADI-S, and 67 recruited to undergo SADI-S in the following 4 months. After withdrawing 8 patients with exclusion criteria and 10 patients lost to follow-up, 283 patients were contacted telephonically in a two-step process that lasted 3 months. The number of patients who finally answered the telematic tests was 246 (86.9%) (Fig. 1).

Flowchart of patients’ selection
Baseline Characteristics
Table 1 shows preoperative demographic and clinical data of the study population, depending on the moment of evaluation before or after surgery. Patients’ age, gender, BMI, and obesity associated medical problems were similar between groups.
Weight Loss and Obesity Associated Medical Problems
Postoperative weight-related outcomes depending on moment of evaluation are described in Table 2.
Baseline mean BMI was 50.8 kg/m2 and 30.0 kg/m2, 31.1 kg/m2, and 32.7 kg/m2 at < 2-, 2–3-, and > 3-year follow-up, respectively (p < 0.001) (Figs. 2 and 3). Mean EWL% also exhibited significant differences depending on moment of follow-up: 82.0%, 75.5%, and 70.0% at < 2-, 2–3-, and > 3-year follow-up, respectively (p = 0.003). These weight control differences are illustrated in Fig. 4.

Weight control (BMI and EWL%) depending on moment of evaluation

Self-reported symptoms depending on moment of evaluation

Physical and mental quality of life depending on moment of evaluation
Patients with > 3-year follow-up presented remission of 84.6% T2D, 75.0% HTN, 76.9% DLP, and 88.9% OSA, with significant control of all associated medical problems. There were significant differences regarding supplementation needs between groups, with up to 67.4% of patients with > 3-year follow-up requiring oral supplementation.
Patient-Reported Outcomes
As shown in Fig. 2, 17.9% of patients in the baseline group had a GERD-Q score ≥ 8. After SADI-S, this percentage increased over time (18.8% vs 26.9% vs 30.2%, respectively), although no statistical difference was reached (p = 0.320).
As for depositional habit, 10.5% patients in the baseline group before surgery had a history of chronic diarrhea or loose stools (Bristol ≥ 5) and 6.0% constipation (Bristol ≤ 2). After SADIS, the percentage of patients with loose stools was progressively higher (17.4% vs 25.4% vs 30.2%, p = 0.043). The incidence of constipation remained steady over time (14.5% vs 13.4% vs 14.0.%, p = 0.386). The average number of bowel moments per day after SADI-S was 1.4, with no statistical differences between groups (1.3 vs 1.7 vs 1.3, p = 0.112).
Quality of Life
Figure 3 displays both physical and mental components of QOL before and after surgery. Baseline group of patients presented a PCS = 34.3 and MCS = 44.7, worse than the Spanish population mean (PCS and MCS = 50). Patients submitted to SADI-S with a follow-up of less than 2 years presented an improvement both in physical and mental condition compared to the baseline group (PCS = 51.3, and MCS = 49.4). Patients with 2–3-year follow-up showed a slight decrease of both PCS and a MCS (49.6 and 46.3, respectively). Following the trend, patients with > 3-year follow-up showed a PCS = 48.3 and MCS = 41.9, being these differences statistically significant (PCS p = 0.000; MCS p = 0.022).
As shown in Tables 3 and 4, there was a significant association between effective weight control and physical and mental QOL: in PCS ≥ 50 group, a higher proportion of patients had achieved a satisfactory weight loss, compared with the group of patients with PCS < 50 (BMI < 35 kg/m2 75.6% vs 38.3%, respectively, p < 0.001). The mean BMI of patients with PCS ≥ 50 was 31.9 kg/m2, compared with 41.7 kg/m2 in the PCS < 50 group (p < 0.001). Similarly, in the MCS ≥ 50 group, there were more patients with a BMI < 35 kg/m2 than the MCS < 50 group (66.7% vs 48.7%, p = 0.004). In the PCS < 50 group, 27.8% of patients had a score of GERD-Q ≥ 8 in comparison to 20.6% in the PCS ≥ 50 group, although no statistical significance was reached (p = 0.186). This non-significant association GERD symptoms and QOL could also be seen in the mental component (MCS < 50: 26.5% vs MCS ≥ 50: 21.7%; p = 0.380). No significant associations were found either between QOL and depositional habit or obesity associated medical problems, except for dyslipidemia (DLP) and mental health status: 28.2% of patients with MCS < 50 suffered from DLP in comparison with 16.3% in the MCS ≥ 50 group (p = 0.024).
Grade of Information Gathering
As shown in Table 5, response rate to the telematics tests was 82.9%, similar to the compliance rate of the cohort in its last presential visit (86.1%).
Telematic follow-up offered a more systemic and detailed information: in the last presential visit, only 13.9% of patients had complete data regarding weight evolution, remission of associated medical problems, GERD symptoms, and depositional habit in comparison with the 82.9% of patients with telematic follow-up (p < 0.001).
Discussion
This prospective cross-sectional study performed with telematic tests in a cohort of 246 patients with morbid obesity before and after SADI-S found a progressive increase in the rate of patients suffering from GERD symptoms and loose stools, up to 30% at 3 years. Besides, physical and mental QOL experienced a soft progressive decrease with follow-up, after an initial substantial postoperative amelioration, being the main conditioning of this factor the loss of efficacy of weight control.
Patient-Reported Outcomes
GERD Symptoms
Prevalence of GERD symptoms after SADI-S is a controverted topic with limited information, mainly due to the lack of reported data with objective and validated questionnaires such as GERD-Q. There are several methods to diagnose GERD symptoms in a bariatric patient: by the symptomatology deliberately referred by the patient or the prescriptions of proton pump inhibitors/antacids; by asking systematically through objective and validated questionnaires such as GERD-Q; and by endoscopic and/or impedance-pH monitoring. Even though endoscopic evaluation is the gold standard to diagnose GERD, the difficulty to perform a systematic evaluation to every patient often relegates it to a second step. GERD-Q test is an efficient method to monitor GERD symptoms with a sensibility of 65% and specificity of 71% in patients without acid-suppressive therapy (cut-off score ≥ 8) [14, 18, 19]. By answering the GERD-Q test, we were able to objectively evaluate the proportion of patients submitted to SADI-S with high probability of suffering symptom-defined GERD.
In our study, patients with a more extended follow-up presented a higher proportion of GERD-Q score ≥ 8 (30.2% in SADI-S > 3 years). The long-term follow-up study by Sánchez-Pernaute et al. [6] described 14% of cases with grade A esophagitis and 8.3% with grade C or D. However, no systematic GERD symptoms questionnaires were provided, and an upper gastrointestinal endoscopy was performed in only 22% of patients. The sleeve gastrectomy shape and high-pressure might be responsible for the presence of acid GERD [20,21,22]. However, the loop configuration of SADI-S could lead to an additional bile reflux risk, which has been associated with a carcinogenic effect [23,24,25]. As mentioned by Yashkov et al., both the distance of the duodenal transection from the pylorus and the initial pyloric insufficiency could potentially be correlated with bile reflux [26]. In a previous report of our group, 3 patients were found to have bile reflux confirmed by impedance-pH monitoring, 2 of them requiring revisional surgery to duodenal switch [8]. The meta-analysis of 2029 patients submitted to SADI-S conducted by Portela et al. concluded that bile reflux has not been demonstrated to have a negative impact after SADI-S [27]. However, the mean follow-up of patients in the study was 10.3 months. In the present study, GERD symptoms increased with time after surgery. Systematic surveillance with objective suggesting symptoms testing and esophagogastroduodenoscopy may be necessary to exclude bile reflux after SADI-S.
Depositional Habit
There is limited data about depositional habit and stool composition of patients submitted to SADI-S, being limited to no specific information or the average number of bowel movements per day in the majority of studies. We decided to incorporate Bristol stool chart as a form to assess bowel habit after bariatric procedures in order to establish a more objective evaluation [28]. Although we did not observe statistical differences in the number of stool frequency per day after SADI-S, we did find differences in consistency, according to the Bristol stool chart. The prevalence of patients with chronic diarrhea or loose stools (Bristol ≥ 5) was higher in the group of patients with longer follow-up.
Even though patients with a longer follow-up presented a higher need for oral supplementation, there were no cases of intractable diarrhea or hypoalbuminemia in the present study. Other series reported a higher average number of daily bowel movements (ranging from 2.1 to 4.2) and an incidence of revisional surgeries due to malabsortive complications up to 10% [6, 29, 30]. These results are probably due to the fact that these studies included patients submitted to SADI-S with a 200-cm or 250-cm common limb length, while the patients in the present cohort had a 300-cm common limb length.
Quality of Life
Obesity is associated with serious metabolic morbidities and a reduced QOL [31]. Patients with severe obesity present a significant improvement in QOL after bariatric surgery [32,33,34,35,36,37]. In our study, prior to SADI-S, patients exhibited poor results regarding their health status (PCS = 34.3, MCS = 44.7) with a significant improvement 2 years after surgery (PCS = 51.3, MCS = 49.4) that was maintained but not so evident in patients with > 3-year follow-up (PCS = 48.3, MCS = 41.9). These results consisted with a cross-sectional study by Marceau et al., which described an improvement of QOL in severely obese patients submitted to biliopancreatic diversion with duodenal switch (BPDDS) in comparison with a group of patients prior to the same surgical procedure [35]. Aasprang et al. found an early enhancement of both PCS and MCS after surgery but a significant decline at 5 years after BPDDS [36]. Canetti et al. reported that even though patients had a successful weight reduction after BPDDS, their mental health worsened significantly after 10-year follow-up [38]. This deterioration of mental health might be potentially related to patients’ unfulfilled expectations on their physical appearance after weight loss in some cases or to the weight regain that occurred in the long-term in other patients. Both physical and mental QOL were associated with weight control in the present study. Patients with lower QOL scores presented mainly after > 3 years follow-up, being this poorer result in relation with weight regain. Our findings are consistent with the Swedish Obese Subjects study, a 10 year follow-up study which concluded that deterioration of health-related QOL scores corresponded with weight regain after bariatric surgery [37].
In addition, the presence of GERD symptoms could also have a relevant impact in the postoperative QOL after SADI-S. GERD symptoms incidence after SADI-S is still unknown, but there is increasing interest in analyzing its role in the omega-reconstruction techniques. In the present study, we found a higher but not significant proportion of GERD-Q ≥ 8 in the group of patients with poorer QOL scores. These results are consisted with the conclusions of Choi et al., a large cross-sectional study which demonstrated that the levels of anxiety and depression were higher in subjects with GERD symptoms than in controls [39]. Furthermore, Yang et al. reported a lower QOL score, measured using the SF-36 questionnaire, in patients suffering from GERD symptoms in comparison with healthy controls [40].
Information Gathering
The present study detected a poorer registration of patient-reported symptoms in presential visits compared with telematic controls. Variables such as GERD symptoms, depositional habit, or QOL were not systematically reflected in patients’ medical history after a presential appointment and therefore may be underestimated. This fact could probably be explained by the elevated number of patients examined in a bariatric surgeon’s visit. Telematic questionnaires could allow a more objective and systematic evaluation of QOL and postoperative symptoms.
Strengths and Limitations
The main limitation of this observational study is the absence of a prospective individual follow-up of patients. However, it is accepted that a cross-sectional study can be an adequate design to interpret the health status and patient-reported symptomatology in different evolution moments [35, 41]. Besides, the homogeneous groups were a representative sample of the cohort of patients submitted to SADI-S which allowed to analyze a chronological evolution of symptoms and QOL before and after surgery [7, 8]. Moreover, the use of an endoscopic procedure for the diagnosis of GERD could have been a great complimentary tool to the GERD-Q test.
One of the strengths of this study is the number of patients (246) and the good response rate to our telematic tests (86.9%). The use of validated tests such as SF-36, GERD-Q, or Bristol stool chart allowed an objective evaluation of self-reported symptoms.
Conclusion
This single-institution cross-sectional study demonstrated that weight control is the main factor related to long-term QOL after SADI-S. Incidence of GERD symptoms and loose stools was up to 30% in patients with > 3 years follow-up. Monitoring postoperative patient-related symptoms with validated objective tests seems a feasible and useful resource for the long-term follow-up of patients submitted to SADI-S.
References
Sánchez-Pernaute A, Rubio-Herrera MA, Pérez-Aguirre ME, García-Pérez JC, Cabrerizo L, Diez-Valladares L, et al. Proximal duodenal-ileal end to side by-pass with sleeve gastrectomy: proposed technique. Obes Surg. 2007;17:1614–8.
Sánchez-Pernaute A, Rubio-Herrera MA, Pérez-Aguirre ME, Talavera P, Cabrerizo L, Matía P, et al. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). One to three-year follow-up Obes Surg. 2010;20(12):1720–6.
Pujol-Gebelli J, García-Ruizde-Gordejuela A, Ramos AC, Nora M, Pereira AM, Campos JM, et al. SADI-S with right gastric artery ligation: technical systematization and early results. Arq Bras Cir Dig. 2016;29(Suppl 1):85–90.
Sánchez-Pernaute A, Rubio MA, Cabrerizo L, Ramos-Levi A, Pérez-Aguirre E, Torres A. Single-anastomosis duodenoileal bypass with sleeve gastrectomy (SADI-S) for obese diabetic patients. Surg Obes Relat Dis. 2015;11(5):1092–8.
Shoar S, Poliakin L, Rubenstein R, Saber AA. Single anastomosis duodeno-Ileal switch (SADIS): a systematic review of efficacy and safety. Obes Surg. 2018; 28(1): 104–13.
Sánchez-Pernaute A, Rubio-Herrera MA, Ferré NP, Rodríguez CS, Marcuello C, Pañella C, et al. Long-term results of single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). Obes Surg. 2022;32(3):682–9.
Finno P, Osorio J, García-Ruiz-de-Gordejuela A, Casajoana A, Sorribas M, Admella V, et al. Single versus double anastomosis duodenal switch: single-site comparative cohort study in 440 consecutive patients. Obes Surg. 2020;30:3309–16.
Admella V, Osorio J, Sorribas M, Sobrino L, Casajoana A, Pujol-Gebellí J. Direct and two-step single anastomosis duodenal switch (SADI-S): unicentric comparative analysis of 232 cases. Cir Esp (Engl Ed). 2021;99(7):514–20.
Osorio J, Lazzara C, Admella V, Franci-León S, Pujol-Gebellí J. Revisional Laparoscopic SADI-S vs. Duodenal switch following failed primary sleeve gastrectomy: a single-center comparison of 101 consecutive cases. Obes Surg. 2021;31(8):3667–74.
Cremades M, Ferret G, Parés D, Navinés J, Espin F, Pardo F, et al. Telemedicine to follow patients in a general surgery department. A randomized controlled trial. Am J Surg. 2020;219(6):882–7.
Vilagut G, Ferrer M, Rajmil L, Rebollo P, Permanyer-Miralda G, Quintana JM, et al. El cuestionario de salud SF-36 español: una década de experiencia y nuevos desarrollos. Gac Sanit. 2005;19:135–50.
Alonso J, Regidor E, Barrio G, Prieto L, Rodríguez C, De La Fuente L. Valores poblacionales de referencia de la versión española del Cuestionario de Salud SF-36. Med Clin (Barc). 1998;111:410–6.
Vilagut G, Valderas JM, Ferrer M, Garin O, López-García E, Alonso J. Interpretación de los cuestionarios de salud SF-36 y SF-12 en España: componentes físico y mental. Med Clin (Barc). 2008;130(19):726–35.
Jones R, Junghard O, Dent J, Vakil N, Halling K, Wernersson B, et al. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Aliment Pharmacol Ther. 2009;30:1030–8.
Suzuki H, Matsuzaki J, Okada S, Hirata K, Fukuhara S, Hibi T. Validation of the GerdQ questionnaire for the management of gastro-esophageal reflux disease in Japan. United European Gastroenterol J. 2013;1:175–83.
Zavala-Gonzales MA, Azamar-Jacome AA, Meixueiro-Daza A, Ramos A, Reyes-Huerta J, Roesch-Dietlen F, et al. Validation and diagnostic usefulness of gastroesophageal reflux disease questionnaire in a primary care level in Mexico. J Neurogastroenterol Motil. 2014;20:475–82.
Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand J Gastroenterol. 1997;32:920–4.
Dent J, Vakil N, Jones R, Bytzer P, Schöning U, Halling K, et al. Accuracy of the diagnosis of GORD by questionnaire, physicians, and a trial of proton pump inhibitor treatment: the Diamond Study. Gut. 2010;59:714–21.
Ciriza-de-los-Ríos C. Questionnaires for the diagnosis of gastroesophageal reflux disease: are they really useful for a diagnostic goal? Rev Esp Enferm Dig. 2016;108(4):171–3.
Chiu S, Birch DW, Shi X, Sharma AM, Karmali S. Effect of sleeve gastrectomy on gastroesophageal reflux disease: a systematic review. Surg Obes Relat Dis Jul-Aug. 2011;7(4):510–5.
Peng BQ, Zhang GX, Chen G, Cheng Z, Hu JK, Du X. Gastroesophageal reflux disease complicating laparoscopic sleeve gastrectomy: current knowledge and surgical therapies. Surg Obes Relat Dis. 2020;16(8):1145–55.
Chiappetta S, Lainas P, Kassir R, Valizadeh R, Bosco A, Kermansaravi M. Gastroesophageal reflux disease as an indication of revisional bariatric surgery-indication and results-a systematic review and metanalysis. Obes Surg. 2022;32(9):3156–71.
Nemoto H, Tate G, Yokomizo K, Umemoto T, Matsubara T, Mizukami H, et al. Gastric mixed adenoneuroendocrine carcinoma occurring 50 years after a gastroenterostomy with Braun anastomosis. Case Rep Oncol. S Karger AG. 2014;7:330–6.
Sitarz R, Maciejewski R, Polkowski WP, Offerhaus GJ. Gastroenterostoma after Billroth antrectomy as a premalignant condition. World J Gastroenterol. 2012;18(25):3201-6.
Li D, Zhang J, Yao WZ, Zhang DL, Feng CC, He Q, et al. The relationship between gastric cancer, its precancerous lesions and bile reflux: a retrospective study. J Dig Dis. 2020;21(4):222–9.
Yashkov Y, Bordan N, Torres A, Malykhina A, Bekuzarov D. SADI-S 250 vs Roux-en-Y duodenal switch (RY-DS): results of 5-year observational study. Obes Surg. 2021;31(2):570–9.
Portela R, Marrerro K, Vahibe A, Galvani C, Billy H, Abu Dayyeh B, et al. Bile reflux after single anastomosis duodenal-ileal bypass with sleeve (SADI-S): a meta-analysis of 2,029 patients. Obes Surg. 2022;32(5):1516–22.
Afshar S, Kelly SB, Seymour K, Woodcock S, Werner AD, Mathers JC. The effects of bariatric procedures on bowel habit. Obes Surg. 2016;26(10):2348–54.
Surve A, Cottam D, Medlin W, Richards C, Belnap L, Horsley B, et al. Long-term outcomes of primary single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). Surg Obes Relat Dis. 2020;16(11):1638–46.
Balibrea JM, Vilallonga R, Hidalgo M, Ciudin A, González Ó, Caubet E, et al. Mid-term results and responsiveness predictors after two-step single-anastomosis duodeno-ileal bypass with sleeve gastrectomy. Obes Surg. 2017;27(5):1302–8.
Fontaine KR, Barofsky I. Obesity and health-related quality of life. Obes Rev. 2001;2(3):173–82.
Kolotkin RL, Davidson LE, Crosby RD, Hunt SC, Adams TD. Six-year changes in health-related quality of life in gastric bypass patients versus obese comparison groups. Surg Obes Relat Dis. 2012;8(5):625–33.
Lee WJ, Pok EH, Almulaifi A, Tsou JJ, Ser KH, Lee YC. Medium-term results of laparoscopic sleeve gastrectomy: a matched comparison with gastric bypass. Obes Surg. 2015;25(8):1431–8.
Canetti L, Elizur Y, Karni Y, Berry EM. Health-related quality of life changes and weight reduction after bariatric surgery vs. a weight-loss program. Isr J Psychiatry Relat Sci. 2013;50:194–201.
Marceau P, Hould FS, Simard S, Lebel S, Bourque RA, Potvin M, et al. Biliopancreatic diversion with duodenal switch. World J Surg. 1998;22(9):947–54.
Aasprang A, Andersen JR, Våge V, Kolotkin R, Natvig GK. Ten-year changes in health-related quality of life after biliopancreatic diversion with duodenal switch. Surg Obes Relat Dis. 2016;12(8):1594–600.
Karlsson J, Taft C, Rydén A, Sjöström L, Sullivan M. Ten-year trends in health-related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. Int J Obes (Lond). 2007;31(8):1248–61.
Canetti L, Bachar E, Bonne O. Deterioration of mental health in bariatric surgery after 10 years despite successful weight loss. Eur J Clin Nutr. 2016;70(1):17–22.
Choi JM, Yang JI, Kang SJ, Han YM, Lee J, Lee C, et al. Association between anxiety and depression and gastroesophageal reflux disease: results from a large cross-sectional study. J Neurogastroenterol Motil. 2018;24(4):593–602.
Yang XJ, Jiang HM, Hou XH, Song J. Anxiety and depression in patients with gastroesophageal reflux disease and their effect on quality of life. World J Gastroenterol. 2015;21(14):4302–9.
Christopher AN, Morris MP, Barrette LX, Patel V, Broach RB, Fischer JP. Longitudinal clinical and patient-reported outcomes after transversus abdominis release for complex hernia repair with a review of the literature. Am Surg. 2021;18:31348211038580.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
This article does not contain any studies with human participants or animals performed by any of the authors. For this type of study, formal consent is not required.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key Points
- Symptoms of GERD up to 30% at 3-year follow-up.
- Weight control is the main factor related to long-term QOL.
- Telemedicine is a resource in long-term follow-up patient-related symptoms.
Victor Admella and Claudio Lazzara have contributed equally to this study.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Admella, V., Lazzara, C., Sobrino, L. et al. Patient-Reported Outcomes and Quality of Life After Single-Anastomosis Duodeno-ileal Bypass with Sleeve Gastrectomy (SADI-S): a Cross-Sectional Study with 283 Patients from a Single Institution. OBES SURG 33, 1754–1763 (2023). https://doi.org/10.1007/s11695-023-06554-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-023-06554-x