
Abstract
Background
While the safety of many bariatric procedures has been previously studied in older patients, we examine the effect of advancing age on medical/surgical complications in laparoscopic sleeve gastrectomy, a relatively unstudied procedure but that is trending upwards in use.
Methods
Patients undergoing laparoscopic sleeve gastrectomy (LSG) and laparoscopic gastric bypass (RYGB) were extracted from the National Surgical Quality Improvement Program 2005–2012 database. Pre- and postoperative variables were analyzed using chi-square and student t test as appropriate to determine the comparative safety of LSG to RYGB in the elderly. Multivariate regression modeling was used to evaluate whether age is associated with adverse 30-day events following LSG.
Results
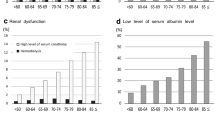
Of the patients that met the inclusion criteria, 56,664 (84 %) patients underwent RYGB and 10,835 (16 %) underwent LSG. In the LSG cohort, incidence of overall complications, medical complications, and death significantly increased with increasing age (p < 0.05). No statistically significant differences in rates of 30-day complications, return to the OR, and mortality exist between RYGB and LSG cohorts in patients older than 65 years. The age group of over 65 years independently predicted increased risk for overall and medical complications (OR, 1.748; OR, 2.027). Notably, age was not significantly associated with surgical complications in LSG.
Conclusion
In this large, multi-institutional study, advanced age was significantly associated with overall and medical complications but not surgical complications in LSG. Our findings suggest that the risk conferred by advancing age in LSG is predominantly for medical morbidity and advocate for improved perioperative management of medical complications. LSG may be the preferable option to RYGB for elderly patients as neither procedure is riskier with regards to 30-day morbidity while LSG has been shown to be safer with regards to long-term reoperation and readmission risk.
Similar content being viewed by others

References
Gupta PK et al. Development and validation of a bariatric surgery morbidity risk calculator using the prospective, multicenter NSQIP dataset. J Am Coll Surg. 2011;212(3):301–9.
Ramanan B et al. Development and validation of a bariatric surgery mortality risk calculator. J Am Coll Surg. 2012;214(6):892–900.
Dorman RB et al. Bariatric surgery outcomes in the elderly: an ACS NSQIP study. J Gastrointest Surg. 2012;16(1):35–44. discussion 44.
DeMaria EJ et al. Validation of the obesity surgery mortality risk score in a multicenter study proves it stratifies mortality risk in patients undergoing gastric bypass for morbid obesity. Ann Surg. 2007;246(4):578–82. discussion 583–4.
Varela JE, Wilson SE, Nguyen NT. Outcomes of bariatric surgery in the elderly. Am Surg. 2006;72(10):865–9.
Carlin AM et al. The comparative effectiveness of sleeve gastrectomy, gastric bypass, and adjustable gastric banding procedures for the treatment of morbid obesity. Ann Surg. 2013;257(5):791–7.
Trastulli S et al. Laparoscopic sleeve gastrectomy compared with other bariatric surgical procedures: a systematic review of randomized trials. Surg Obes Relat Dis. 2013;9(5):816–29.
Bellanger DE, Greenway FL. Laparoscopic sleeve gastrectomy, 529 cases without a leak: Short-term results and technical considerations. Obes Surg. 2011;21(2):146–50.
Hutter MM et al. First report from the American College of Surgeons Bariatric Surgery Center Network: laparoscopic sleeve gastrectomy has morbidity and effectiveness positioned between the band and the bypass. Ann Surg. 2011;254(3):410–20. discussion 420–2.
Birkmeyer NJ et al. Hospital complication rates with bariatric surgery in Michigan. JAMA. 2010;304(4):435–42.
Menenakos E et al. Laparoscopic sleeve gastrectomy performed with intent to treat morbid obesity: a prospective single-center study of 261 patients with a median follow-up of 1 year. Obes Surg. 2010;20(3):276–82.
Sanchez-Santos R et al. Short- and mid-term outcomes of sleeve gastrectomy for morbid obesity: the experience of the Spanish National Registry. Obes Surg. 2009;19(9):1203–10.
Helmio M et al. Comparison of short-term outcome of laparoscopic sleeve gastrectomy and gastric bypass in the treatment of morbid obesity: a prospective randomized controlled multicenter SLEEVEPASS study with 6-month follow-up. Scand J Surg. 2014;103(3):175–81.
Ritz P, et al. Benefits and risks of bariatric surgery in patients aged more than 60 years. Surg Obes Relat Dis. 2014.
Spaniolas K et al. Early morbidity and mortality of laparoscopic sleeve gastrectomy and gastric bypass in the elderly: a NSQIP analysis. Surg Obes Relat Dis. 2014;10(4):584–8.
Lynch J, Belgaumkar A. Bariatric surgery is effective and safe in patients over 55: a systematic review and meta-analysis. Obes Surg. 2012;22(9):1507–16.
Turrentine FE et al. Surgical risk factors, morbidity, and mortality in elderly patients. J Am Coll Surg. 2006;203(6):865–77.
Yanquez FJ et al. Synergistic effect of age and body mass index on mortality and morbidity in general surgery. J Surg Res. 2013;184(1):89–100.
Curiel-Balsera E et al. Mortality and complications in elderly patients undergoing cardiac surgery. J Crit Care. 2013;28(4):397–404.
Birkmeyer JD et al. Blueprint for a new American College of Surgeons: National Surgical Quality Improvement Program. J Am Coll Surg. 2008;207(5):777–82.
Henderson WG, Daley J. Design and statistical methodology of the National Surgical Quality Improvement Program: why is it what it is? Am J Surg. 2009;198(5 Suppl):S19–27.
Merkow RP et al. Relevance of the c-statistic when evaluating risk-adjustment models in surgery. J Am Coll Surg. 2012;214(5):822–30.
Paul P, Pennell ML, Lemeshow S. Standardizing the power of the Hosmer-Lemeshow goodness of fit test in large data sets. Stat Med. 2013;32(1):67–80.
Finks JF et al. Predicting risk for venous thromboembolism with bariatric surgery: results from the Michigan Bariatric Surgery Collaborative. Ann Surg. 2012;255(6):1100–4.
Lee WJ et al. Gastric bypass vs sleeve gastrectomy for type 2 diabetes mellitus: a randomized controlled trial. Arch Surg. 2011;146(2):143–8.
Karamanakos SN et al. Weight loss, appetite suppression, and changes in fasting and postprandial ghrelin and peptide-YY levels after Roux-en-Y gastric bypass and sleeve gastrectomy: a prospective, double blind study. Ann Surg. 2008;247(3):401–7.
Himpens J, Dapri G, Cadiere GB. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy: Results after 1 and 3 years. Obes Surg. 2006;16(11):1450–6.
Li JF et al. Comparison of laparoscopic Roux-en-Y gastric bypass with laparoscopic sleeve gastrectomy for morbid obesity or type 2 diabetes mellitus: a meta-analysis of randomized controlled trials. Can J Surg. 2013;56(6):E158–64.
Peterli R et al. Early results of the Swiss Multicentre Bypass or Sleeve Study (SM-BOSS): a prospective randomized trial comparing laparoscopic sleeve gastrectomy and Roux-en-Y gastric bypass. Ann Surg. 2013;258(5):690–4. discussion 695.
Flum DR et al. Early mortality among Medicare beneficiaries undergoing bariatric surgical procedures. JAMA. 2005;294(15):1903–8.
O'Keefe KL, Kemmeter PR, Kemmeter KD. Bariatric surgery outcomes in patients aged 65 years and older at an American Society for Metabolic and Bariatric Surgery Center of Excellence. Obes Surg. 2010;20(9):1199–205.
Livingston EH et al. Male gender is a predictor of morbidity and age a predictor of mortality for patients undergoing gastric bypass surgery. Ann Surg. 2002;236(5):576–82.
Sugerman HJ et al. Effects of bariatric surgery in older patients. Ann Surg. 2004;240(2):243–7.
Finks JF et al. Predicting risk for serious complications with bariatric surgery: Results from the Michigan Bariatric Surgery Collaborative. Ann Surg. 2011;254(4):633–40.
Financial Support
This particular research received no internal or external grant funding.
Ethical Approval
De-identified patient information is freely available to all institutional members who comply with the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) Data Use Agreement. The Data Use Agreement implements the protections afforded by the Health Insurance Portability and Accountability Act of 1996 and the ACS-NSQIP Hospital Participation Agreement, and conforms to the Declaration of Helsinki.
Disclaimer
The NSQIP and the hospitals participating in the NSQIP are the source of the data used herein; they have not been verified and are not responsible for the statistical validity of the data analysis, or the conclusions derived by the authors of this study.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Qin, C., Luo, B., Aggarwal, A. et al. Advanced Age as an Independent Predictor of Perioperative Risk after Laparoscopic Sleeve Gastrectomy (LSG). OBES SURG 25, 406–412 (2015). https://doi.org/10.1007/s11695-014-1462-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-014-1462-0