
Background
We studied whether weight loss by intragastric balloon would predict the outcome of subsequent gastric banding with regard to weight loss and BMI reduction.
Methods
A prospective cohort of patients with a body mass index (BMI) >40 kg/m2 received an intragastric balloon for 6 months followed by laparoscopic adjustable gastric banding (LAGB). Successful ballooninduced weight loss was defined as ≥10% weight loss after 6 months. Successful surgical weight loss was defined as an additional 15% weight loss in the following 12 months. Patients were divided in group A, losing ≥10% of their initial weight with 6 months’ balloon treatment, and group B, losing <10% of their initial weight.
Results
In 40 patients (32 female, 8 male; age 36.6 yr, range 26–54), the mean BMI decreased from 46.5 to 40.5 kg/m2 (P<0.001) after 6 months of balloon treatment and to 35.2 kg/m2 (P<0.001) 12 months after LAGB. Group A (25 patients) and group B (15 patients) had a significant difference in BMI decrease, 12.4 vs 9.0 kg/m2 (P<0.05), after the total study duration of 18 months. However, there was no difference in BMI reduction (4.7 kg/m2 vs 5.8 kg/m2) in the 12 months after LAGB. 6 patients in group A lost ≥10% of their starting weight during 6 months balloon treatment as well as ≥15% 12 months following LAGB. 6 patients in group B lost <10% of their starting weight after 6 months of BIB, but also lost ≥5% 12 months following LAGB.
Conclusion
Intragastric balloon did not predict the success of subsequent LAGB.
Similar content being viewed by others
Introduction
The modern lifestyle of increased food consumption and sedentary activities has resulted in a global epidemic of obesity. Morbid obesity is associated with serious health problems, including cardiovascular disease, hypertension, diabetes type 2, hyperlipidemia, sleep apnea syndrome, osteoarthritis, certain neoplasms, psychosocial disabilities and impaired quality of life. Conservative treatments with diets and medication are successful in the short term, but during long-term follow-up, the relapse rate is high after the treatment is discontinued; >90% of the patients are back to their starting weights within 5 years.1,2
In the 1980s, intragastric balloon treatment was introduced, with satisfactory short-term effects at 6 months, but with balloon removal, patients relapsed to their original weight or even higher — the weight cycling effect.3,4 Morbid obesity (body mass index >40 kg/m2 or >35 kg/m2 with co-morbidity) seems to be very treatment-resistant by conservative therapy, but long-term results are achieved with bariatric surgery,5 including restrictive procedures resulting in decreased oral intake and malabsorptive procedures resulting in decreased intestinal absorption.
Laparoscopic adjustable gastric banding (LAGB) has been proven to be safe, easily reversible and is adjustable; this restrictive procedure generally has a low morbidity and results in satisfactory weight loss, at least in short-term follow-up.6–9 Yet, a substantial number of patients fail to respond in the long-term, which is why laparoscopic gastric bypass is gaining interest.10,11 Therefore, a selection instrument that may be used to determine which patient would respond to gastric restrictive or malabsorptive surgery, is needed. Some authors have applied the “balloon-test”, because it was suggested that patients who demonstrate good short-term weight loss after balloon treatment may continue weight loss after LAGB.12 In the super-obese, some surgeons perform a long-limb gastric bypass or biliopancreatic diversion at the outset. This signifies a major operation in a group of patients in whom some might have benefit from gastric banding, even if a malabsorptive procedure may later be needed. They then could have a lower weight to undergo the second intervention.13–15
Therefore we decided to investigate prospectively if and to what extent the preoperative placement of a gastric balloon could be used to better select morbidly obese patients for bariatric operations.
Patients and Methods
Patients
Consecutive patients referred for bariatric surgery were asked to participate in a prospective study, consisting of 6 months of intragastric balloon treatment followed by gastric banding. Patients were screened by a multidisciplinary team consisting of a surgeon, dietician, gastroenterologist and psychologist. The inclusion criteria of the NIH16 were followed (Table 1) and patients signed informed consent. The study was approved by the Medical Ethics Committee of the Isala clinics.
After balloon placement, patients were followed monthly for the first 6 months. They were admitted after 6 months for balloon removal under general anesthesia, and during the same general anesthetic, laparoscopic gastric banding was performed. Then patients were followed on an outpatient basis by the investigator and the dietician every 3 months for the first year. Successful weight loss with the balloon was defined as 10% weight loss in the first 6 months. Successful weight loss with the subsequent gastric banding was defined as a 15% weight loss in the ensuing 12 months.
Patients were divided in two groups; group A consisted of patients who lost ≥10% of their starting weight in 6 months with the intragastric balloon; group B had a more limited success with the balloon, a loss of <10% of their starting weight. All patients were analyzed 18 months after the entire treatment protocol.
Technique
Balloon Procedure
The procedure has been described in detail before.3,4,12,17,18 The BioEnterics Intragastric balloon (BIB® Allergan, Santa Barbara, CA, USA) was inserted under fluoroscopic control and with the patient sitting on a table, conscious and cooperating. The BIB was filled with 500 ml of saline stained with methylene blue. Methylene blue served as a marker for balloon rupture by subsequent blue coloring of the urine. Six months later, the patient was admitted to the hospital and under general anesthesia the balloon was removed endoscopically by puncturing and grasping with a forceps. After a repeat endoscopy to deflate the stomach and to rule out balloon-induced mucosal injury, gastric banding surgery was performed.
In the 6 months of balloon treatment, no adjustments of balloon volume, albeit feasible, were done. However, when patients complained of blue color in the urine, a plain abdominal X-ray was done to check if the balloon was still fully filled and in the stomach. When in doubt, a repeat endoscopy was performed to check the balloon and, if necessary, to replace the balloon by a new one.
Laparoscopic Surgical Procedure
The procedure of the LAGB has been described previously, 6,19,20 with subsequent changes in the technique to prevent pouch formation.21 The patient was placed in lithotomy position with the knees and hips slightly flexed. Using 4 trocars, the band (Lap-band® 9.75 or 11 cm, Allergan, Santa Barbara, CA, USA) was placed around the stomach through the pars flaccida approach from the base of the right crus along the left crus to the angle of His.21 At least four ventral gastrogastric stitches were placed over the band to prevent slippage of the distal stomach upwards through the band. Through the xiphoid trocar-site, the tube was pulled out and tunnelled subcutaneously to the sternum where the port was implanted. The band was left empty for at least 6 weeks, and the patient followed a fluid diet to prevent slippage of the stomach. After 6 weeks, the patient was allowed to eat everything, guided by the dietician as to energy intake.
If weight loss levelled off, the band was inflated by puncture of the port and injection of saline. The first attempt was always done under fluoroscopic control. All but one patient had the balloon removed and the band placed, under the same general anesthetic.
Endpoints
The primary end-points were weight loss and BMI 1 year after gastric banding, including the weight loss during the balloon treatment in all patients and separately in group A and B patients. Secondary end-points were complications related to balloon placement and events related to LAGB such as periand postoperative complications, hospital stay, long-term complications, additional procedures, readmissions, band adjustments, and weight loss and BMI reduction 1 year after gastric banding alone.
Statistical Analysis
Based on previous studies in our hospital with BIB17 starting from a hypothetical 75% success rate of a balloon (success defined as ≥10% initial weight loss) and thus a 25% balloon failure rate, and a 50% success or failure rate of LAGB (with each a 75% success rate and 25% failure rate in the balloon arm), a power analysis (α of <0.05, power (1 − β) 0.80) resulted in a number to treat of 38 patients in order to detect a significant difference in weight loss in patients who had 6 months of preoperative treatment with the BIB followed by 12 months of LAGB. Descriptive data are given as means ± standard deviation (SD). Student t-test (and Mann-Whitney U test for non-Gaussian data) was used to compare group A and B patients. Weight loss and BMI were studied with logistic regression for “success” or “non-success”.
Results
Patients
From March 1999 until February 2002, 46 consecutive patients (9M/37F) fulfilled the inclusion criteria. Six patients (1M/5F) had to be excluded from the study because of balloon-related problems and subsequent refusal of the gastric banding procedure. In the remaining 40 patients, there were eight men and 32 women with mean age 36.6 yr (range 26–54 yr), mean weight 142.4 kg (range 111–204 kg) and mean BMI 46.5 kg/m2 (range 38.9–61.7 kg/m2). Mean excess weight (EW) was 65.8% (range 42.9 to 110.4%) (Table 2). Co-morbidities consisted of cardiovascular problems (7.5%), pulmonary problems (30%), diabetes type 2 (10%), hypertension (27.5%) and osteoarthritis (70%).
Intragastric Balloon and Gastric Band
Removal of the BIB took on average 25 minutes (mean 35.8 ± 19.2 SD minutes) (Table 3). In one patient, the band was placed 3 days later because the removal of the balloon took too long (135 minutes). In four patients, no balloon was discovered upon endoscopy, and none of these patients reported having seen blue coloring of the urine. In one patient, a second balloon was placed because of suspected leakage and passage into the small intestine. When this balloon was removed, the first balloon appeared to be still present in the stomach.
The positioning of the gastric band took 104 minutes ± 50.2 minutes, with no mortality. Hospital stay averaged 5.1 days (range 3–10 days).
Major complications requiring re-operation were seen in five patients (12.5%). In three patients, gastric slippage occurred, which required re-operation to reposition the band. Two patients developed pouch dilatation, 14 and 20 months, after the operation, respectively. One band was repositioned via laparotomy. The second band was removed due to a severe metabolic derangement in a patient with alcohol abuse and doubtful cooperation.
Minor complications occurred in 12 patients (26%): an abdominal hematoma at the left trocar site, treated conservatively; conversion to a laparotomy, because of left liver lobe hypertrophy in three patients; one persistent postoperative vomiting due to edema of the stomach, treated conservatively; one infection from the saline used to fill the band, resolved with local antibiotics; twice an endoscopy because of food retention above the band; three times a symptomatic cholelithiasis, treated with an uneventful laparoscopic cholecystectomy; and once a myocardial infarction treated with a coronary angioplasty. Because of successful weight reduction, three patients underwent an abdominoplasty.
Outcome
In the entire group, the mean BMI during balloon treatment declined from 46.5 kg/m2 to 40.5 kg/m2 (P<0.001) after a mean treatment of 194 days ± 12 days, with an excess weight loss (EWL) of 28.7%. The mean BMI declined further from 40.5 kg/m2 to 35.2 kg/m2 (P<0.001) 12 months after LAGB with a EWL of 57.1% (Table 4).
Group A consisted of 25 patients with 10% initial weight loss after 6 months balloon treatment. Group B consisted of 15 patients with <10% initial weight loss. Patient characteristics of groups A and B were not different at the start for age (35.8 vs 36.3 yr), weight (141.2 vs 144.4 kg), BMI (47.0 vs 45.6 kg/m2) and excess weight (66.0 vs 65.6%). However, significantly more subjects in group B suffered from diabetes type 2 (P=0.02) (Table 2).
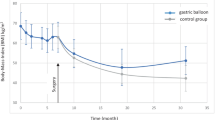
After 6 months of BIB treatment and 12 months of LAGB, there was a significant difference (P<0.05) in BMI reduction between group A (12.4 kg/m2) and group B (9.0 kg/m2) (Table 4). Weight loss had a trend (P=0.07) in favor of group A (A 37.3 kg vs B 28.7 kg). The 12-month period of gastric banding resulted in a BMI reduction of 4.7 kg/m2 in group A vs 5.8 kg/m2 in group B, and a weight loss of 13.8 kg in group A vs 18.6 kg in group B (not different between group A and B, P=0.35 and 0.22, respectively). This was also true for the mean EWL of 32.9% vs 33.8 % (P=0.91). There was no significant difference between the two groups with respect to the period of the gastric band (Figure 1 and 2). The overall difference in BMI appears to be related to the initial weight-reducing effect of the BIB.

Total weight loss after 6 months BIB plus 12 months LAGB (SD) of the total group, group A (≥10% WL) and group B (<10% WL) after 6 months BIB.

Total BMI reduction after 6 months BIB plus 12 months LAGB (SD) of the total group, group A (≥10% WL) and group B (<10% WL) after 6 months BIB.
Balloon complications and surgical complications peri- and postoperatively were not statistically different in both groups (P=0.40, 0.60 and 0.30, respectively) (Table 4).
In group A (25 patients), there were 6 patients who not only lost ≥10% of their initial weight during the balloon treatment, but also lost ≥15% of their starting weight in the following 12 months; however, 19 patients did not lose the 15% in the 12 months of LAGB. In group B (15 patients), 9 patients were unsuccessful in both treatment periods; 6 patients were unsuccessful in the balloon period, but lost ≥15% of their starting weight in the following 12 months (Table 5a). The positive predictive value of the balloon was 32% and the negative predictive value of the balloon was 60%.
When we added the required ≥10% weight loss for a successful BIB outcome to the 15% required for a successful bariatric surgery outcome (thus, resulting in successful weight loss of 25% for the study duration), there were 14 successful patients vs 4 unsuccessful ones in group A. In group B, 11 patients were successful and 11 were not. This improved the positive predictive value of the balloon to 56% and the negative predictive value of the balloon to 73% (Table 5b).
Discussion
This study found that both BIB and LAGB can be performed safely, without mortality and with an acceptable rate of complications. The weight reduction (30% EWL/ 6 months, 57% EWL/ 18 months) is in accordance with other large series of balloon and band treatment.3,17,18,22,23
However, the hypothesis of the BIB being predictive for successful LAGB had to be rejected, when defining a weight loss of 10% in the first 6 months of balloon treatment as successful and requiring a weight loss of an additional 15% in the 12 months following LAGB surgery. A problem with our definition could be that we did not take into account that losing ≥10% during the first 6 months may make it more difficult to lose another 15% after banding. That this might be the case is reflected by the fact that there is a difference in the loss of weight, BMI and % excess weight after 18 months compared to the loss in weight, BMI and % excess weight after 12 months treatment with the band alone (Table 4).
The weight loss difference between the two groups after 6 months treatment with the balloon was preserved in time, because this difference did not diverge any further after the LAGB procedure (Figures 1 and 2). Thus, if a patient is unsuccessful with the balloon, he/she can still be successful in losing weight after banding. Longer follow-up is needed to see whether the weight difference will persist or diminish.14 A criticism may be that the less successful group had more diabetic patients who may have more difficulty losing weight. When we compare our study with large series, there tends to be a higher percentage of patients with diabetes (33–75%)24 and a much lower number with osteoarthritis (12%).25
The intolerance to the BIB (11%) is relatively high compared to the literature (6%),4,22 but adjustments to reduce the balloon volume were not performed.
LAGB appeared to be a safe method, and no major complications occurred in this study. Operative time decreased with increasing experience. Length of hospital stay was 5 days and compared favorably to other bariatric operations.
Conclusion
Changes in BMI and weight in patients who underwent LAGB after a 6-month preoperative placement of a gastric balloon, appeared not to be predicted by the results obtained with the balloon. The greater loss of BMI in the successful balloon-treated group was maintained through the 1st year after surgery. Pre-treatment with BIB could be more relevant for super-obese patients anesthesiologically.
References
Mathus-Vliegen EM. [Overweight. II. Determinants of overweight and strategies for prevention]. Ned Tijdschr Geneeskd 1998; 142: 1989–95.
Mathus-Vliegen EM. [Overweight. I. Prevalence and trends]. Ned Tijdschr Geneeskd 1998; 142: 1982–9.
Mathus-Vliegen EM, Tytgat GN, Veldhuyzen-Offermans EA. Intragastric balloon in the treatment of super-morbid obesity. Double-blind, sham-controlled, crossover evaluation of 500-milliliter balloon. Gastroenterology 1990; 99: 362–9.
Mathus-Vliegen EM, Tytgat GN. Intragastric balloons for morbid obesity: results, patient tolerance and balloon life span. Br J Surg 1990; 77: 76–9.
Buchwald H, Williams SE. Obesity surgery worldwide 2003. Obes Surg 2004; 14: 1157–64.
Belachew M, Belva PH, Desaive C. Long-term results of laparoscopic adjustable gastric banding for the treatment of morbid obesity. Obes Surg 2002; 12: 564–8.
O’Brien PE, McPhail T, Chaston TB et al. Systematic review of medium-term weight loss after bariatric operations. Obes Surg 2006; 16: 1032–40.
Ponce J, Haynes B, Paynter S et al. Effect of Lap-Bandinduced weight loss on type 2 diabets mellitus and hypertension. Obes Surg 2004; 14: 1335–42.
Chevallier J-M, Zinzindohoue F, Douard R et al. Complications after laparoscopic adjustable gastric banding for morbid obesity: experience with 1,000 patients over 7 years. Obes Surg 2004; 14: 407–14.
Mognol P, Chosidow D, Marmuse J-P. Laparoscopic conversion of laparoscopic gastric banding to Roux-en- Y gastric bypass: a review of 70 patients. Obes Surg 2004; 14: 1349–53.
van Wageningen B, Berends FJ, van Ramshorst B et al. Revision of failed laparoscopic adjustable gastric banding to Roux-en-Y gastric bypass. Obes Surg 2006; 16: 137–41.
Loffredo A, Cappuccio M, Naddeo M et al. Three years experience with the new intragastric balloon, and a preoperative test for success with restrictive surgery. Obes Surg 2001; 11: 330–3.
Weiner R, Gutberlet H, Bockhorn H. Preparation of extremely obese patients for laparoscopic gastric banding by gastric-balloon therapy. Obes Surg 1999; 9: 261–4.
Busetto L, Segato G, Magon A et al. Preoperative weight loss by intragastric balloon in super-obese patients treated with laparoscopic gastric banding: a case-control study. Obes Surg 2004; 14: 671–6.
Alfalah H, Philippe B, Ghazal F et al. Intragastric balloon for preoperative weight loss in candidate for laparoscopic gastric bypass with massive obesity. Obes Surg 2006; 16: 16: 147–50.
Gastrointestinal surgery for severe obesity. National Institutes of Health Consensus Development Conference Panel Draft Statement. Obes Surg 1991; 1: 257–65.
Mathus-Vliegen EM, Tytgat GN. Intragastric balloon for treatment-resistant obesity: safety, tolerance, and efficacy of 1-year balloon treatment followed by a 1-year balloon-free follow-up. Gastrointest Endosc 2005; 61: 19–27.
Sallet JA, Marchesini JB, Paiva DS et al. Brazilian multicenter study of the intragastric balloon. Obes Surg 2004; 14: 991–8.
de Wit LT, Mathus-Vliegen L, Obertop H et al. Open versus laparoscopic adjustable silicone gastric banding: a prospective randomized trial for treatment of morbid obesity. Ann Surg 1999; 230: 800–5.
Rubenstein RB. Laparoscopic adjustable gastric banding at a U.S. center with up to 3-year follow-up. Obes Surg 2002; 12: 380–4.
O’Brien PE, Dixon JB, Laurie C et al. A prospective randomized trial of placement of the laparoscoic adjustable gastric band: comparison of the perigastric and pars flaccida pathways. Obes Surg 2005; 15: 820–6.
Doldi SB, Micheletto G, Rella S et al. Treatment of morbid obesity with intragastric balloon in association with diet. Obes Surg 2002; 12: 583–7.
Al-Momen A, El-Mogy I. Intragastric balloon for obesity: a retrospective evaluation of tolerance and efficacy. Obes Surg 2005; 15: 101–5.
Pories WJ, Swanson MS, Brown BM et al. Who would have thought it? An operation proves to be the most effective therapy for adult-onset diabetes mellitus. Ann Surg 1995; 222: 339–50.
Rosenbaum M, Leibel RL, Hirsch J. Obesity. N Engl J Med 1997; 337: 396–407.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
de Goederen-van der Meij, S., Pierik, R.G.J.M., Pool, M.O. et al. Six Months of Balloon Treatment does Not Predict the Success of Gastric Banding. OBES SURG 17, 88–94 (2007). https://doi.org/10.1007/s11695-007-9011-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-007-9011-8