
Abstract
Summary
This study describes childhood fracture rates in Norway, a country known for high fracture rates in the adult population. Fracture rates correspond with other reports from Scandinavia, although with a slightly higher proportion in girls. Indications of increased vulnerability during stages of puberty require further exploration.
Introduction
Fractures are common injuries during childhood. Incidence rates and patterns vary, but population-based data are scarce. The aim of this study was to describe the sex-, age- and maturation-specific incidence of fractures in a representative population-based sample from a region in Norway.
Methods
All fractures in the population based convenient cohort Fit Futures, comprising 961 adolescents under 18 years, were recorded retrospectively from the local hospital. Details on individual’s age and fracture site were recorded. A radiologist confirmed all fractures.
Results
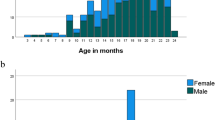
In the period from birth to cohort scanning, the register recorded 316 fractures in 253 individuals. Fractures were more common in boys (35%) than in girls (31%). The overall annual fracture incidence was 204 per 10,000 persons-year under the age of 18 and 205 under the age of 16. The majority of fractures involved the upper extremities and the most common site of fracture was the forearm with 24% of the fractures followed by phalanges with 23% of the fractures. Fractures peaked in girls at sexual maturation stage 3. Boys had a peak in stage 2. Timing of subsequent fractures was also consistent with stages of sexual maturation.
Conclusions
The overall incidence of fractures in childhood in Northern Norway corresponds with other reports from Scandinavia, although the proportion of fractures in girls is higher than in other studies. Both sexes seem especially vulnerable at stages related to sexual maturation. Whether this reflects bone vulnerability or other changes related to puberty requires further investigation.






Similar content being viewed by others


References
Landin LA (1983) Fracture patterns in children. Analysis of 8,682 fractures with special reference to incidence, etiology and secular changes in a Swedish urban population 1950-1979. Acta Orthop Scand Suppl 202:1–109
Mattila V et al (2004) Occurrence and risk factors of unintentional injuries among 12- to 18-year-old Finns—a survey of 8219 adolescents. Eur J Epidemiol 19(5):437–444
Jones G, Cooley HM (2002) Symptomatic fracture incidence in those under 50 years of age in southern Tasmania. J Paediatr Child Health 38(3):278–283
Sibert JR, Maddocks GB, Brown BM (1981) Childhood accidents—an endemic of epidemic proportion. Arch Dis Child 56(3):225–227
Lyons RA et al (1999) Children’s fractures: a population based study. Inj Prev 5(2):129–132
Cheng JC et al (1999) A 10-year study of the changes in the pattern and treatment of 6,493 fractures. J Pediatr Orthop 19(3):344–350
Brudvik C, Hove LM (2003) Childhood fractures in Bergen, Norway: identifying high-risk groups and activities. J Pediatr Orthop 23(5):629–634
Hedstrom EM et al (2010) Epidemiology of fractures in children and adolescents. Acta Orthop 81(1):148–153
Kopjar B, Wickizer TM (1998) Fractures among children: incidence and impact on daily activities. Inj Prev 4(3):194–197
Tiderius CJ, Landin L, Duppe H (1999) Decreasing incidence of fractures in children: an epidemiological analysis of 1,673 fractures in Malmo, Sweden, 1993-1994. Acta Orthop Scand 70(6):622–626
Rennie L et al (2007) The epidemiology of fractures in children. Injury 38(8):913–922
Mayranpaa MK, Makitie O, Kallio PE (2010) Decreasing incidence and changing pattern of childhood fractures: a population-based study. J Bone Miner Res 25(12):2752–2759
Cooper C et al (2004) Epidemiology of childhood fractures in Britain: a study using the general practice research database. J Bone Miner Res 19(12):1976–1981
Kanis JA et al (2012) A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int 23(9):2239–2256
Falch JA et al (1993) Secular increase and geographical differences in hip fracture incidence in Norway. Bone 14(4):643–645
Sogaard AJ et al (2014) Cohort profile: Norwegian Epidemiologic Osteoporosis Studies (NOREPOS). Scand J Public Health 42(8):804–813
Lyons RA et al (2000) Incidence and cause of fractures in European districts. Arch Dis Child 82(6):452–455
Amin S et al (2013) A distal forearm fracture in childhood is associated with an increased risk for future fragility fractures in adult men, but not women. J Bone Miner Res 28(8):1751–1759
Holloway KL et al (2015) Prior fracture as a risk factor for future fracture in an Australian cohort. Osteoporos Int 26(2):629–635
Ahmed LA et al (2013) Progressively increasing fracture risk with advancing age after initial incident fragility fracture: the Tromsø study. J Bone Miner Res 28(10):2214–2221
Coleman L, Coleman J (2002) The measurement of puberty: a review. J Adolesc 25(5):535–550
Duke PM, Litt IF, Gross RT (1980) Adolescents’ self-assessment of sexual maturation. Pediatrics 66(6):918–920
Gluckman PD, Hanson MA (2006) Changing times: the evolution of puberty. Mol Cell Endocrinol 254-255:26–31
Winther A et al (2014) The Tromsø Study: Fit Futures: a study of Norwegian adolescents’ lifestyle and bone health. Arch Osteoporos 9:185
Christoffersen T et al (2015) Does the frequency and intensity of physical activity in adolescence have an impact on bone? The Tromsø Study, Fit Futures. BMC Sports Sci Med Rehabil 7:26
Tanner JM, Davies PS (1985) Clinical longitudinal standards for height and height velocity for North American children. J Pediatr 107(3):317–329
Waaler PE (1983) Anthropometric studies in Norwegian children. Acta Paediatr Scand Suppl 308:1–41
Garn SM (1972) The course of bone gain and the phases of bone loss. Orthop Clin North Am 3(3):503–520
Schoenau E et al (2001) The development of bone strength at the proximal radius during childhood and adolescence. J Clin Endocrinol Metab 86(2):613–618
Spear LP (2000) The adolescent brain and age-related behavioral manifestations. Neurosci Biobehav Rev 24(4):417–463
Acknowledgements
We are grateful to the study participants, the staff at the Clinical Research Unit at University Hospital of North Norway (UNN HF), and the Fit Futures administration for conducting the study. We thank Robert Kechter at Finnmark Hospital Trust and The Garvan Institute of Medical Research for office and administration contribution. We also thank The Norwegian Osteoporosis Association for supporting pediatric software and the Northern Norway Regional Health Authorities for funding this work.
Authors contribution
Study design: TC, AW, LAA, and NE. Study conduct: A-SF, GG, and NE. Data collection: TC, A-SF, GG, NE, OAN, and AW. Data analysis: TC, JAE, JRC, LAA, and NE. Data interpretation: TC, JAE, JRC, LAA, and NE. Drafting manuscript: TC, JAE, JRC, LAA, and NE. Revising manuscript content: TC, JAE, JRC, AW, LAA, GG, OAN, ED, and NE. Approving final version of manuscript: TC, JAE, JRC, AW, LAA, GG, OAN, ED, and NE. TC, LAA, and NE take responsibility for the integrity of the data analysis.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was approved by The Norwegian Data Protection Authority (reference number 2009/1282) and by The Regional Committee of Medical and Health Research Ethics (reference number 2011/1702/REKnord).
Conflict of interest
None.
Electronic supplementary material
ESM 1
(DOCX 15 kb)
Rights and permissions
About this article

Cite this article
Christoffersen, T., Ahmed, L.A., Winther, A. et al. Fracture incidence rates in Norwegian children, The Tromsø Study, Fit Futures. Arch Osteoporos 11, 40 (2016). https://doi.org/10.1007/s11657-016-0294-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11657-016-0294-z