
Abstract
The aim of this review was to summarize the latest evidence on image-guided thermal ablation therapies for lung metastases. PubMed was used to search for relevant articles that reported the oncological outcomes of thermal ablation for metastatic lung tumors, and those published in 2010 or later were selected for review. Ablative therapies were applied for lung metastases from various types of primary tumors, but most commonly colorectal ones. Radiofrequency ablation (RFA) was the most evaluated technique, followed by microwave ablation (MWA). The local control rates of ablative therapies were generally favorable, approximately 80–90% in many studies. Representative studies demonstrated promising overall survival rates of approximately 50% or higher 5 years after ablation for lung metastases from colorectal cancer or mixed types of primary tumors. Nevertheless, the survival outcomes varied depending on the type of primary tumor and background factors of patients such as other metastases and comorbidities. Several studies had aimed to compare the outcomes of various ablative therapies such as RFA, MWA, and cryoablation; however, conclusive data are not yet available to determine the most appropriate ablation modality for lung metastases. Further data accumulation is needed, especially for long-term outcomes and comparisons with other therapies.
Similar content being viewed by others


Introduction
The lung is a frequent site for various types of malignant tumors to metastasize [1, 2]. Local therapies such as surgery, radiotherapy, and thermal ablation may be beneficial for patients with lung metastases, especially when complete eradication of all metastases is anticipated [3]. Because of their minimal invasiveness and repeatable nature, image-guided thermal ablation therapies such as radiofrequency ablation (RFA), microwave ablation (MWA), and cryoablation (CA) have been used to treat lung tumors, particularly in patients with contraindications to surgery. The Society of Interventional Radiology deems image-guided ablation an acceptable treatment option for patients with metastatic lung disease in their multidisciplinary position statement [4]. The Cardiovascular and Interventional Radiological Society of Europe also describes the role of thermal ablation for lung metastases in their Standards of Practice document [3]. The present article provides an overview of the latest evidence on the oncological outcomes of image-guided thermal ablation therapies for lung metastases by reviewing the literature published since 2010.
Literature search
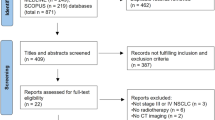
PubMed was used on April 19, 2022 to search for articles that included the following terms in their titles: ("lung” OR "pulmonary") AND ("metastasis" OR "metastases" OR "metastatic") AND ("ablation” OR "ablative"). The initial search identified 247 articles, of which 188 published since 2010 (considered the most recent articles) were selected. Articles were further screened based on their titles, abstracts, and text for the following criteria: (i) English language articles, (ii) original clinical studies or meta-analyses, and (iii) studies focusing on the oncological outcomes of thermal ablation for metastatic lung tumors that reported specific survival data such as overall survival (OS). We excluded small series with fewer than 10 patients and studies in which lung ablation was used for palliative purposes. Furthermore, studies with mixed study populations of primary and metastatic lung tumors, which precluded the evaluation of discrete data on lung metastases, were excluded. When multiple studies in the same institution had considerable overlapping in terms of subjects, the study with a larger sample size was selected for review. Screened articles were scrutinized further to include relevant articles from their reference lists in the final review.
Ablative therapies for lung metastases: an overview of recent literature
Among the reviewed studies, large-scale ones tended to include patients with mixed types of primary tumors. In the studies that included each individual type of primary tumor, lung metastasis from colorectal cancer (CRC) was focused on the most, followed by that from sarcoma. RFA was the most commonly used technique, followed by MWA. Long-term outcomes were mainly available for RFA. Most studies on MWA, CA, and laser interstitial thermal therapy (LITT) were published from 2016 onward. Some studies aimed to compare the outcomes of multiple types of thermal ablation therapies, as described below.
Outcomes in studies that included mixed types of primary tumors
Table 1 shows the results of studies that included mixed types of primary tumors [5,6,7,8,9,10,11,12,13,14,15,16]. Although those studies included various primary tumors, most predominantly included CRC, with only one focusing on non-CRC lung metastases [9]. The largest study was a meta-analysis recently published by Nguyenhuy et al. that analyzed, from 23 studies, 1804 patients who underwent RFA, MWA, or CA; notably, this meta-analysis included eight Japanese studies [5]. The 1-, 2-, 3-, 4-, and 5-year OS/progression-free survival (PFS) rates in the meta-analysis were 92.3%/53.1%, 80.0%/34.8%, 67.9%/25.4%, 58.8%/22.2%, and 50.7%/19.5%, respectively [5]. Among the studies that evaluated each type of ablation modality, the largest was conducted for RFA by de Baère et al. using their prospective database, which included 566 patients with 1037 tumors [12]. In their study, the 1-, 2-, 3-, 4- and 5-year OS/PFS rates after RFA were 92.4%/40.2%, 79.4%/23.3%, 67.7%/16.4%, 58.9%/13.1%, and 51.5% (the 5-year PFS was not available), respectively [12]. Other prospective or retrospective studies on RFA demonstrated comparable 3-year OS rates of approximately 50–75% [6, 10, 11, 15, 16], except for one prospective study by Wang et al., which showed a 3-year OS rate of 14% [13]. Wang et al. attributed the poor OS to a high proportion of patients with multiple lung metastases and extrathoracic diseases in their study cohort [13]. Vogl et al. conducted a prospective study on MWA that included 80 patients with 130 tumors and reported the 1- and 2-year OS rates to be 91.3% and 75.0%, respectively [14]. Callstrom et al. recently reported the results of their prospective study on CA, which included 128 patients with 224 tumors; the 1- and 2-year OS rates after CA were 97.6% and 86.6%, respectively [8]. Furthermore, de Baère et al. prospectively evaluated the long-term outcomes of CA in 40 patients with 60 tumors [7, 17]; the 3- and 5-year local tumor control rates were 87.9% and 79.2%, respectively, and the 3- and 5-year OS rates were 63.2% and 46.7%, respectively [7].
The above-mentioned studies tended to have relatively large study populations because they included a variety of primary tumors, allowing an overview of the general outcomes of thermal ablation therapies for lung metastases. However, survival outcomes might be affected by the proportion of each type of primary tumor included in each study. Indeed, the type of primary tumor is significantly correlated with survival in several studies [11,12,13]. Consequently, it is necessary to review the outcomes of ablative therapies for each type of tumor separately. Reportedly, prognostic factors other than the type of primary tumor include the presence of extrathoracic metastases [6], the size and number of lung metastases [6, 12], the response to treatment [14, 16], and the disease-free interval [12, 16]. Thus, the discrepancy between outcomes in each study might be caused by different patient conditions, including pre-ablation tumor burden.
Outcomes by each type of primary tumor
Colorectal cancer
Table 2 shows the outcomes of ablative therapies for lung metastases from CRC [12, 18,19,20,21,22,23,24,25,26,27,28,29,30,31]. RFA was the most frequently used treatment in the listed studies. Although most studies had a retrospective design, Hasegawa et al. recently conducted a multicenter prospective trial in Japan [18]. In this trial, RFA was performed in 70 patients with 100 surgically resectable lung metastases (≤ 5 in number per patient and ≤ 3 cm in size) and an excellent 3-year OS rate of 84% was achieved [18]. Some studies reported the long-term outcomes of RFA based on relatively long follow-up periods. Zhong et al. retrospectively evaluated the outcomes of RFA in patients with histologically confirmed CRC lung metastases [19]. The 1-, 3-, 5-, 7-, and 9-years OS/PFS rates were 96.7%/66.7%, 74.7%/31.2%, 44.1%/25.9%, 27.5%/21.2%, and 16.3%/5.9%, respectively, with a median follow-up duration of 45.5 months [19]. Fonck et al. and Matsui et al. showed similar 5-year survival rates of 54.7% and 51.6%, respectively, in their retrospective studies [23, 27]. In a study on RFA for lung metastases from various primary tumors, de Baère et al. performed subgroup analyses for each group of patients with colon and rectal cancer and reported 5-year OS rates of 56.0% and 49.6% in the colon and rectum groups, respectively [12]. In the other studies, the 3- and 5-year OS rates after ablative therapies for lung metastases from CRC were 44–61% and 20–30%, respectively [21, 22, 24, 26, 28,29,30,31]. Local tumor control rates by ablative therapies were approximately 80–90% in most studies; notably, several studies published from 2018 onward achieved local control rates of 90% or higher [18, 19, 21, 23]. Because these studies included tumors of relatively small sizes (mean or median, 10–14 mm), their favorable local control rates might be attributable to appropriate tumor selection based on the knowledge that tumors of large sizes are a risk factor for local tumor progression [12]. To select candidates likely to receive survival benefits from lung ablation, it is necessary to determine the prognostic factors after ablation. In several studies, a high pre-ablation carcinoembryonic antigen (CEA) value was a negative prognostic factor after ablative therapies [18, 21, 27]. In addition, Huo et al. found that CEA density, i.e., pre-ablation CEA per volume of all lung metastases, was associated with OS [24]. In contrast, Ferguson et al. identified post-RFA CEA values as a significant prognostic factor as opposed to pre-RFA values [26]. The presence of extrapulmonary metastases was also a significant prognostic factor in several studies and was associated with poor OS [20, 27, 31] or chemotherapy-free survival [23]. Regarding the association between systemic chemotherapy and post-ablation survival, Hasegawa et al. revealed that the absence of chemotherapy before RFA was significantly associated with poor OS [18]. Chua et al. demonstrated that patients who received adjunct chemotherapy before or after RFA showed better OS than those who did not [31]. Kurilova et al. showed that three or more lines of pre-ablation chemotherapy with or without targeted therapy was a negative prognostic factor after MWA [21]. Other negative prognostic factors in the previous studies included a larger number of lung metastases [12, 19, 29], a larger tumor size [12, 20, 22], rectal rather than colon cancer [18], a shorter progression-free interval [19], a worse response to RFA [31], and a lack of repeated RFA [33].
Considering the favorable outcomes seen in several studies, image-guided ablation is a valid treatment for lung metastases from CRC [3]. The current National Comprehensive Cancer Network guidelines for colon cancer state that ablative therapies may be considered alone or in conjunction with surgical resection for resectable lung metastases [32].
Sarcoma
The main series of ablative therapies for lung metastases from sarcoma are summarized in Table 3 [12, 33,34,35,36]. RFA was always performed in the listed studies, except for the most recent one by Bourgouin et al., in which MWA and CA were used [33]. A relatively wide range of survival rates was demonstrated; the 1- and 3-year OS rates were 81–100% and 47–85%, respectively [12, 33,34,35,36]. The primary sites of sarcoma in those studies varied and included the bone, soft tissue, and parenchymal organs. Therefore, the difference in survival outcomes might be attributed to different patient backgrounds in each study. The local efficacy was consistent and favorable across studies: local control rates of 85–95% were achieved for tumors with a mean or median size of 9–14 mm [12, 33,34,35,36]. Regarding prognostic factors, Koelblinger et al. reported that a short disease-free interval (≤ 24 months) between the diagnosis of the primary lesion and lung metastases was significantly associated with inferior OS [35]. Sato et al. found that extrapulmonary metastasis, noncurative ablation, and a short disease-free interval (≤ 12 months) after ablation were negative prognostic factors [34]. The treatment of lung metastases from sarcoma by a combination of thermal ablation and surgery has also been investigated; Nakamura et al. treated 92 patients with soft tissue sarcoma with lung metastasectomy (n = 70), RFA (n = 13), or both (n = 9) and reported the 5-year post-metastatic disease-specific survival rate to be 52% [37]. Disease-specific survival rates at 3 years were 66%, 59.2%, and 66.7% in the surgery, RFA, and surgery + RFA groups, respectively [37].
Hepatocellular carcinoma
Table 4 shows the results of recent studies on ablative therapies for lung metastases from hepatocellular carcinoma (HCC) [38,39,40,41]. The 1-, 3-, and 5-year OS rates after lung ablation were reported to be 73–89%, 30–70%, and 26–31%, respectively, with most patients being treated with RFA [38,39,40,41]. A lower number of lung metastases was a favorable prognostic factor in several studies [38, 40]. Specifically, Yuan et al. showed that patients with ≤ 2 tumors and unilateral metastases had better OS rates than those with > 2 tumors and bilateral metastases, respectively [38]. Li et al. also found that ≤ 3 lung metastases were a favorable prognostic factor of OS [40]. In addition, studies by both Li et al. and Hiraki et al. demonstrated that lower serum α-fetoprotein levels and the absence of viable or uncontrolled intrahepatic tumors were associated with better OS [40, 41]. Other positive prognostic factors included a maximum tumor diameter of ≤ 3 cm, Child–Pugh class A disease, the absence of liver cirrhosis, and the absence of hepatitis C virus infection [40, 41]. All the above-mentioned studies had a retrospective design and a relatively small study population (< 40 patients). Thus, further investigation with a large population size is necessary to validate the usefulness of ablation therapies for lung metastases from HCC.
Renal cell carcinoma
Regarding lung metastases from renal cell carcinoma (RCC), Gonnet et al. retrospectively evaluated the outcomes of RFA in 53 patients with 100 tumors: a local efficacy of 91% and 1-, 3-, and 5-year OS rates of 94.0%, 74.5%, and 61.8%, respectively, were seen with a median follow-up of 60.8 months [42]. This was comparable to the outcome of the subgroup analysis in the study by de Baère et al., who demonstrated 1-, 3-, and 5-year OS rates of 95.5%, 73.5%, and 53.8%, respectively, after RFA in 68 patients with renal tumors [12]. Similarly, the RCC subgroup in a meta-analysis by Nguyenhuy et al. showed 1-, 3-, and 5-year OS rates of 93.0%, 71.7%, and 57.5%, respectively [5]. Concerning prognostic factors, Gonnet et al. found that the T3/T4 stage of primary RCC was associated with unfavorable survival [42].
Breast cancer
Thermal ablation for lung metastases from breast cancer was investigated by several researchers. Meng et al. reported the outcomes of MWA in 32 breast cancer patients with 46 tumors [43]. In their study, the 1-, 3-, and 5-year OS rates were 96.5%, 53.3%, and 17.8%, respectively, with local tumor progression observed in 10.9% of the ablated lesions [43]. Patients without extrapulmonary metastases showed a significantly longer median survival time (median of 24 months with extrapulmonary metastases vs. 36 months without, p = 0.005) [43]. Wang et al. investigated the outcomes of RFA for residual lung metastases from breast cancer after systemic chemotherapy [44]. Complete response was achieved in 59 of 67 lesions (88%) in 35 patients, and the 1-, 2-, and 3-year OS rates were 88.6%, 59.3%, and 42.8%, respectively [44]. Two or more lung metastases, a lesion diameter of > 2 cm, and coexisting liver metastases were associated with unfavorable OS [44].
Esophageal cancer
Two retrospective studies investigated RFA for lung metastases from esophageal cancer. Matsui et al. evaluated the outcomes of RFA in 21 patients: local tumor progression was observed in 8 of 31 tumors (25.8%), and the 1-, 2-, and 3-year OS rates after RFA were 85.7%, 54.8%, and 38.4%, respectively [45]. The presence of viable extrapulmonary recurrences was an unfavorable prognostic factor [45]. Baba et al. analyzed the outcomes of 10 patients who underwent RFA for 17 metastases [46]. In their study, the local control rate was 83% at 1 year and the 1- and 2-year OS rates were 77.8% and 62.2%, respectively [46].
Head and neck cancer
Bonichon et al. recently reported the results of a retrospective study on thermal ablation for lung metastases from thyroid cancer [47]. In their study, 47 patients with 107 tumors were treated with 56, 9, and 10 sessions of RFA, MWA, and CA, respectively, achieving a 5-year local control rate of 94.8% and 2- and 3-year OS rates of 93.0% and 79.0%, respectively [47]. The histological type of thyroid cancer was a prognostic factor [47]. Pan et al. retrospectively evaluated the outcomes of RFA for lung metastases from nasopharyngeal carcinoma: local tumor progression was found in 3 of 23 metastases (13%) in 10 patients [48]. A matched-pair analysis showed the median OS after the diagnosis of lung metastases was different between patients treated with and without lung RFA (77.1 months vs. 32.4 months, p = 0.009) [48].
Ablation for lung oligometastases
The role of ablative therapies for lung oligometastases, i.e., a limited number of metastases confined to the lung, has been of particular interest to researchers. Because the presence of extrathoracic metastases and the number of metastases affect survival outcomes, patients with oligometastatic lung disease are theoretically assumed to be favorable candidates for lung ablation. In a meta-analysis by Nguyenhuy et al., a subgroup analysis of patients with lung oligometastases showed 1-, 3-, and 5-year OS rates of 96%, 76.4%, and 54%, respectively [5]. Tselikas et al. retrospectively reviewed patients with lung oligometastases (up to five in number with a maximum diameter of 4 cm and without pleural invasion or mediastinal lymph node metastases) from various types of primary tumors and reported 1- and 3-year OS rates of 94% and 72%, respectively (Table 1) [6]. Omae et al. evaluated the survival of 123 patients after RFA for lung oligometastases from various primary lesions, defined as up to five metastases confined to the lung with the primary lesion and other metastases eradicated at the time of initial RFA, and showed favorable 1-, 3-, and 5-year OS rates of 95%, 76%, and 62%, respectively (Table 1) [11]. The results of these studies suggest that thermal ablation is a promising treatment option for oligometastatic lung disease. Ablative therapies were preferentially used on patients with five or fewer lung metastases; however, the maximum number of metastases to be ablated has not been clearly defined and may depend on the growth rate of the tumors [3].
Comparison of ablation modalities
In several studies, the treatment outcomes of different ablation modalities were compared. Nour-Eldin et al. reported that the local tumor progression rates after ablation for lung metastases from non-CRC were 7.7%, 20.4%, and 27.3% for MWA, RFA, and LITT, respectively (p = 0.012) (Table 1) [9]. MWA was beneficial for PFS (median 23.5, 19.9, and 16.7 months for MWA, LITT, and RFA, respectively, p = 0.048) [9]. Vogl et al. retrospectively compared the outcomes of MWA, RFA, and LITT for lung metastases from CRC (Table 2): MWA had the best local tumor control compared with RFA and LITT, although no difference in OS and PFS was observed between the three ablation methods [25]. They suggested MWA could create a wider ablation zone, thereby contributing to better local control [25]. However, the local control rate in their RFA cohort was 69%, which was low compared with other recent studies (Table 2). In a study on ablative therapies for lung metastases from HCC by Yuan et al., no difference in OS or local tumor PFS was found between ablation methods, including RFA, MWA, and CA [38]. Bourgouin et al. compared the local efficacy of MWA with that of CA for lung metastases from sarcoma (MWA for 34 tumors and CA for 27): no difference in local tumor control was detected [33]. In a meta-analysis that included primary and metastatic lung tumors, Yuan et al. performed subgroup analysis to compare the outcomes of RFA with that of MWA for metastatic lung tumors: RFA achieved a better median OS than did MWA (34.8 months vs. 18.7 months, p = 0.001) [49]. Nevertheless, they warned that this result should be interpreted with caution because the meta-analysis was conducted with only seven retrospective studies of RFA and one of MWA [49]. To date, RFA has been the most evaluated method among all thermal ablation therapies and is widely used to treat lung metastases. MWA has some theoretical advantages, such as a rapid temperature increase, a reduced heat-sink effect, and a larger ablation zone [3, 50]. Advantages of CA include preservation of collagenous architecture and less intraprocedural pain [3, 50]. However, compared with RFA, MWA and CA have less data on long-term outcomes available. Further data are needed to determine the most appropriate ablation modality.
Conclusion
The outcomes of thermal ablation for lung metastases have been investigated in a growing number of studies over the past decade, with ablation for lung metastases from CRC being primarily evaluated. The present review revealed favorable local control and survival outcomes after ablative therapy for lung metastases from various types of primary tumors. The type of primary tumor and other background factors in each patient affect the prognosis; therefore, it is mandatory to take these factors into consideration when determining the indication for ablation. RFA has been the most evaluated technique, and further studies investigating the effectiveness of MWA and CA are warranted to allow the different ablation modalities to be compared thoroughly. In addition, despite not being the subject of this review, comparative data on thermal ablation with surgery and radiation therapy should also be accumulated to define the role of thermal ablation in the management of lung metastases.
References
Gerull WD, Puri V, Kozower BD. The epidemiology and biology of pulmonary metastases. J Thorac Dis. 2021;13:2585–9. https://doi.org/10.21037/jtd.2020.04.28.
Chen H, Stoltzfus KC, Lehrer EJ, Horn SR, Siva S, Trifiletti DM, et al. The epidemiology of lung metastases. Front Med (Lausanne). 2021;8: 723396. https://doi.org/10.3389/fmed.2021.723396.
Venturini M, Cariati M, Marra P, Masala S, Pereira PL, Carrafiello G. CIRSE standards of practice on thermal ablation of primary and secondary lung tumours. Cardiovasc Intervent Radiol. 2020;43:667–83. https://doi.org/10.1007/s00270-020-02432-6.
Genshaft SJ, Suh RD, Abtin F, Baerlocher MO, Chang AJ, Dariushnia SR, et al. Society of interventional radiology multidisciplinary position statement on percutaneous ablation of non-small cell lung cancer and metastatic disease to the lungs: endorsed by the canadian association for interventional radiology, the cardiovascular and interventional radiological society of Europe, and the society of interventional oncology. J Vasc Interv Radiol. 2021;32:1241.e1-1241.e12. https://doi.org/10.1016/j.jvir.2021.04.024.
Nguyenhuy M, Xu Y, Maingard J, Barnett S, Kok HK, Brooks M, et al. A systematic review and meta-analysis of patient survival and disease recurrence following percutaneous ablation of pulmonary metastasis. Cardiovasc Intervent Radiol. 2022. https://doi.org/10.1007/s00270-022-03116-z.
Tselikas L, Garzelli L, Mercier O, Auperin A, Lamrani L, Deschamps F, et al. Radiofrequency ablation versus surgical resection for the treatment of oligometastatic lung disease. Diagn Interv Imaging. 2021;102:19–26. https://doi.org/10.1016/j.diii.2020.09.006.
de Baère T, Woodrum D, Tselikas L, Abtin F, Littrup P, Deschamps F, et al. The eclipse study: efficacy of cryoablation on metastatic lung tumors with a 5-year follow-up. J Thorac Oncol. 2021;16:1840–9.https://doi.org/10.1016/j.jtho.2021.07.021
Callstrom MR, Woodrum DA, Nichols FC, Palussiere J, Buy X, Suh RD, et al. Multicenter study of metastatic lung tumors targeted by interventional cryoablation evaluation (SOLSTICE). J Thorac Oncol. 2020;15:1200–9. https://doi.org/10.1016/j.jtho.2020.02.022.
Nour-Eldin NA, Exner S, Al-Subhi M, Naguib NNN, Kaltenbach B, Roman A, et al. Ablation therapy of non-colorectal cancer lung metastases: retrospective analysis of tumour response post-laser-induced interstitial thermotherapy (LITT), radiofrequency ablation (RFA) and microwave ablation (MWA). Int J Hyperthermia. 2017;33:820–9. https://doi.org/10.1080/02656736.2017.1306656.
Fanucchi O, Ambrogi MC, Aprile V, Cioni R, Cappelli C, Melfi F, et al. Long-term results of percutaneous radiofrequency ablation of pulmonary metastases: a single institution experience. Interact Cardiovasc Thorac Surg. 2016;23:57–64. https://doi.org/10.1093/icvts/ivw089.
Omae K, Hiraki T, Gobara H, Iguchi T, Fujiwara H, Matsui Y, et al. Long-term survival after radiofrequency ablation of lung oligometastases from five types of primary lesions: a retrospective evaluation. J Vasc Interv Radiol. 2016;27:1362–70. https://doi.org/10.1016/j.jvir.2016.05.017.
de Baère T, Aupérin A, Deschamps F, Chevallier P, Gaubert Y, Boige V, et al. Radiofrequency ablation is a valid treatment option for lung metastases: experience in 566 patients with 1037 metastases. Ann Oncol. 2015;26:987–91. https://doi.org/10.1093/annonc/mdv037.
Wang Y, Lu X, Wang Y, Li W, Li G, Zhou J. A prospective clinical trial of radiofrequency ablation for pulmonary metastases. Mol Clin Oncol. 2015;3:559–62. https://doi.org/10.3892/mco.2015.525.
Vogl TJ, Naguib NNN, Gruber-Rouh T, Koitka K, Lehnert T, Nour-Eldin NEA. Microwave ablation therapy: clinical utility in treatment of pulmonary metastases. Radiology. 2011;261:643–51. https://doi.org/10.1148/radiol.11101643.
Von Meyenfeldt EM, Prevoo W, Peyrot D, Fat LA, NLA, Burgers SJA, Wouters MW, et al. Local progression after radiofrequency ablation for pulmonary metastases. Cancer. 2011;117:3781–7. https://doi.org/10.1002/cncr.25958.
Chua TC, Sarkar A, Saxena A, Glenn D, Zhao J, Morris DL. Long-term outcome of image-guided percutaneous radiofrequency ablation of lung metastases: an open-labeled prospective trial of 148 patients. Ann Oncol. 2010;21:2017–22. https://doi.org/10.1093/annonc/mdq098.
de Baère T, Tselikas L, Woodrum D, Abtin F, Littrup P, Deschamps F, et al. Evaluating cryoablation of metastatic lung tumors in patients-safety and efficacy: the eclipse trial-interim analysis at 1 year. J Thorac Oncol. 2015;10:1468–74. https://doi.org/10.1097/JTO.0000000000000632.
Hasegawa T, Takaki H, Kodama H, Yamanaka T, Nakatsuka A, Sato Y, et al. Three-year survival rate after radiofrequency ablation for surgically resectable colorectal lung metastases: a prospective multicenter study. Radiology. 2020;294:686–95. https://doi.org/10.1148/radiol.2020191272.
Zhong J, Palkhi E, Ng H, Wang K, Milton R, Chaudhuri N, et al. Long-term outcomes in percutaneous radiofrequency ablation for histologically proven colorectal lung metastasis. Cardiovasc Intervent Radiol. 2020;43:1900–7. https://doi.org/10.1007/s00270-020-02623-1.
Hiyoshi Y, Miyamoto Y, Kiyozumi Y, Sawayama H, Eto K, Nagai Y, et al. CT-guided percutaneous radiofrequency ablation for lung metastases from colorectal cancer. Int J Clin Oncol. 2019;24:288–95. https://doi.org/10.1007/s10147-018-1357-5.
Kurilova I, Gonzalez-Aguirre A, Beets-Tan RG, Erinjeri J, Petre EN, Gonen M, et al. Microwave ablation in the management of colorectal cancer pulmonary metastases. Cardiovasc Intervent Radiol. 2018;41:1530–44. https://doi.org/10.1007/s00270-018-2000-6.
Cheng G, Shi L, Qiang W, Wu J, Ji M, Lu Q, et al. The safety and efficacy of microwave ablation for the treatment of CRC pulmonary metastases. Int J Hyperthermia. 2018;34:486–91. https://doi.org/10.1080/02656736.2017.1366553.
Fonck M, Perez JT, Catena V, Becouarn Y, Cany L, Brudieux E, et al. Pulmonary thermal ablation enables long chemotherapy-free survival in metastatic colorectal cancer patients. Cardiovasc Intervent Radiol. 2018;41:1727–34. https://doi.org/10.1007/s00270-018-1939-7.
Huo YR, Glenn D, Liauw W, Power M, Zhao J, Morris DL. Evaluation of carcinoembryonic antigen (CEA) density as a prognostic factor for percutaneous ablation of pulmonary colorectal metastases. Eur Radiol. 2017;27:128–37. https://doi.org/10.1007/s00330-016-4352-0.
Vogl TJ, Eckert R, Naguib NNN, Beeres M, Gruber-Rouh T, Nour-Eldin NA. Thermal ablation of colorectal lung metastases: retrospective comparison among laser-induced thermotherapy, radiofrequency ablation, and microwave ablation. AJR Am J Roentgenol. 2016;207:1340–9. https://doi.org/10.2214/AJR.15.14401.
Ferguson J, Alzahrani N, Zhao J, Glenn D, Power M, Liauw W, et al. Long term results of RFA to lung metastases from colorectal cancer in 157 patients. Eur J Surg Oncol. 2015;41:690–5. https://doi.org/10.1016/j.ejso.2015.01.024.
Matsui Y, Hiraki T, Gobara H, Iguchi T, Fujiwara H, Nagasaka T, et al. Long-term survival following percutaneous radiofrequency ablation of colorectal lung metastases. J Vasc Interv Radiol. 2015;26:303–10. https://doi.org/10.1016/j.jvir.2014.11.013.
Gillams A, Khan Z, Osborn P, Lees W. Survival after radiofrequency ablation in 122 patients with inoperable colorectal lung metastases. Cardiovasc Intervent Radiol. 2013;36:724–30. https://doi.org/10.1007/s00270-012-0500-3.
Petre EN, Jia X, Thornton RH, Sofocleous CT, Alago W, Kemeny NE, et al. Treatment of pulmonary colorectal metastases by radiofrequency ablation. Clin Colorectal Cancer. 2013;12:37–44. https://doi.org/10.1016/j.clcc.2012.07.003.
Yamauchi Y, Izumi Y, Kawamura M, Nakatsuka S, Yashiro H, Tsukada N, et al. Percutaneous cryoablation of pulmonary metastases from colorectal cancer. PLoS ONE. 2011;6: e27086. https://doi.org/10.1371/journal.pone.0027086.
Chua TC, Thornbury K, Saxena A, Liauw W, Glenn D, Zhao J, et al. Radiofrequency ablation as an adjunct to systemic chemotherapy for colorectal pulmonary metastases. Cancer. 2010;116:2106–14. https://doi.org/10.1002/cncr.24952.
National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. Colon Cancer. version 1.2022. 2022 Accessed 2022 May 5. https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf
Bourgouin PP, Wrobel MM, Mercaldo ND, Murphy MC, Leppelmann KS, Levesque VM, et al. Comparison of percutaneous image-guided microwave ablation and cryoablation for sarcoma lung metastases: a 10-year Experience. AJR Am J Roentgenol. 2022;218:494–504. https://doi.org/10.2214/AJR.21.26551.
Sato T, Iguchi T, Hiraki T, Gobara H, Fujiwara H, Sakurai J, et al. Radiofrequency ablation of pulmonary metastases from sarcoma: single-center retrospective evaluation of 46 patients. Jpn J Radiol. 2017;35:61–7. https://doi.org/10.1007/s11604-016-0601-z.
Koelblinger C, Strauss S, Gillams A. Outcome after radiofrequency ablation of sarcoma lung metastases. Cardiovasc Intervent Radiol. 2014;37:147–53. https://doi.org/10.1007/s00270-013-0644-9.
Palussière J, Italiano A, Descat E, Ferron S, Cornélis F, Avril A, et al. Sarcoma lung metastases treated with percutaneous radiofrequency ablation: results from 29 patients. Ann Surg Oncol. 2011;18:3771–7. https://doi.org/10.1245/s10434-011-1806-0.
Nakamura T, Asanuma K, Takao M, Yamanaka T, Koike H, Chen-Yoshikawa TFC, et al. Clinical outcome in soft tissue sarcoma patients with lung metastasis who received metastasectomy and/or radiofrequency ablation: Tokai musculoskeletal oncology consortium study. Cancer Manag Res. 2021;13:8473–80. https://doi.org/10.2147/CMAR.S333721.
Yuan Z, Liu B, Hu C, Li Z, Zheng J, Li W. Clinical outcomes of percutaneous thermal ablation for pulmonary metastases from hepatocellular carcinoma: a retrospective study. Int J Hyperthermia. 2020;37:651–9. https://doi.org/10.1080/02656736.2020.1775899.
Lassandro G, Picchi SG, Bianco A, Di Costanzo G, Coppola A, Ierardi AM, et al. Effectiveness and safety in radiofrequency ablation of pulmonary metastases from HCC: a five years study. Med Oncol. 2020;37:25. https://doi.org/10.1007/s12032-020-01352-2.
Li X, Wang J, Li W, Huang Z, Fan W, Chen Y, et al. Percutaneous CT-guided radiofrequency ablation for unresectable hepatocellular carcinoma pulmonary metastases. Int J Hyperthermia. 2012;28:721–8. https://doi.org/10.3109/02656736.2012.736669.
Hiraki T, Yamakado K, Ikeda O, Matsuoka T, Kaminou T, Yamagami T, et al. Percutaneous radiofrequency ablation for pulmonary metastases from hepatocellular carcinoma: results of a multicenter study in Japan. J Vasc Interv Radiol. 2011;22:741–8. https://doi.org/10.1016/j.jvir.2011.02.030.
Gonnet A, Salabert L, Roubaud G, Catena V, Brouste V, Buy X, et al. Renal cell carcinoma lung metastases treated by radiofrequency ablation integrated with systemic treatments: over 10 years of experience. BMC Cancer. 2019;19:1182. https://doi.org/10.1186/s12885-019-6345-2.
Meng M, Han X, Li W, Huang G, Ni Y, Wang J, et al. CT-guided microwave ablation in patients with lung metastases from breast cancer. Thorac Cancer. 2021;12:3380–6. https://doi.org/10.1111/1759-7714.14212.
Wang Y, Lu X, Wang Y, Zhou J. Clinical effect of percutaneous radiofrequency ablation for residual lung metastases from breast cancer after systemic chemotherapy. J Coll Physicians Surg Pak. 2015;25:602–5.
Matsui Y, Hiraki T, Gobara H, Fujiwara H, Iguchi T, Shirakawa Y, et al. Percutaneous radiofrequency ablation for pulmonary metastases from esophageal cancer: retrospective evaluation of 21 patients. J Vasc Interv Radiol. 2014;25:1566–72. https://doi.org/10.1016/j.jvir.2014.06.030.
Baba Y, Watanabe M, Kawanaka K, Iwagami S, Ishimoto T, Iwatsuki M, et al. Radiofrequency ablation for pulmonary metastases from esophageal squamous cell carcinoma. Dis Esophagus. 2014;27:36–41. https://doi.org/10.1111/dote.12034.
Bonichon F, de Baere T, Berdelou A, Leboulleux S, Giraudet AL, Cuinet M, et al. Percutaneous thermal ablation of lung metastases from thyroid carcinomas. A retrospective multicenter study of 107 nodules. On behalf of the TUTHYREF network. Endocrine. 2021;72:798–808. https://doi.org/10.1007/s12020-020-02580-2.
Pan CC, Wu PH, Yu JR, Li W, Huang ZL, Wang JP, et al. Comparative survival analysis in patients with pulmonary metastases from nasopharyngeal carcinoma treated with radiofrequency ablation. Eur J Radiol. 2012;81:e473–7. https://doi.org/10.1016/j.ejrad.2011.05.037.
Yuan Z, Wang Y, Zhang J, Zheng J, Li W. A meta-analysis of clinical outcomes after radiofrequency ablation and microwave ablation for lung cancer and pulmonary metastases. J Am Coll Radiol. 2019;16:302–14. https://doi.org/10.1016/j.jacr.2018.10.012.
Palussière J, Catena V, Buy X. Percutaneous thermal ablation of lung tumors – radiofrequency, microwave and cryotherapy: where are we going? Diagn Interv Imaging. 2017;98:619–25. https://doi.org/10.1016/j.diii.2017.07.003.
Acknowledgements
We would like to thank Editage (www.editage.com) for English language editing.
Funding
None.
Author information
Authors and Affiliations
Contributions
This review was conceptualized by Yusuke Matsui, Koji Tomita, and Takao Hiraki. Literature search and review were performed by Yusuke Matsui, Mayu Uka, Noriyuki Umakoshi, and Takahiro Kawabata. The first draft of the manuscript was written by Yusuke Matsui, and all authors contributed to revising the previous versions of the manuscript. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Matsui, Y., Tomita, K., Uka, M. et al. Up-to-date evidence on image-guided thermal ablation for metastatic lung tumors: a review. Jpn J Radiol 40, 1024–1034 (2022). https://doi.org/10.1007/s11604-022-01302-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11604-022-01302-0