
Abstract
This study aims to identify the combined role of environmental pollutants and atmospheric variables at short term on the rate of incidence (TIC) and on the hospital admission rate (TIHC) due to COVID-19 disease in Spain. This study used information from 41 of the 52 provinces of Spain (from Feb. 1, 2021 to May 31, 2021). Using TIC and TIHC as dependent variables, and average daily concentrations of PM10 and NO2 as independent variables. Meteorological variables included maximum daily temperature (Tmax) and average daily absolute humidity (HA). Generalized linear models (GLM) with Poisson link were carried out for each provinces The GLM model controlled for trend, seasonalities, and the autoregressive character of the series. Days with lags were established. The relative risk (RR) was calculated by increases of 10 μg/m3 in PM10 and NO2 and by 1 °C in the case of Tmax and 1 g/m3 in the case of HA. Later, a linear regression was carried out that included the social determinants of health. Statistically significant associations were found between PM10, NO2, and the rate of COVID-19 incidence. NO2 was the variable that showed greater association, both for TIC as well as for TIHC in the majority of provinces. Temperature and HA do not seem to have played an important role. The geographic distribution of RR in the studied provinces was very much heterogeneous. Some of the health determinants considered, including income per capita, presence of airports, average number of diesel cars per inhabitant, average number of nursing personnel, and homes under 30 m2 could explain the differential geographic behavior. As findings indicates, environmental factors only could modulate the incidence and severity of COVID-19. Moreover, the social determinants and public health measures could explain some patterns of geographically distribution founded.
Similar content being viewed by others

Introduction
On March 11, 2020, the World Health Organization (WHO) declared a state of pandemic caused by COVID-19 (Cucinotta and Vanelli 2020). After the declaration of the state of emergency in Spain (March 14, 2020), the pandemic became the most important scientific issue around the world. Different lines of research have been established, including the origins of the virus (WHO-Convened Global Study of Origins of SARS-CoV-2, s. f.; Tang et al. 2020), its transmission mechanisms and treatments (Lotfi et al. 2020–COVID-19 Transmission, prevention, and potential .pdf, s. f.). Other lines of research have been focused on factors that could increase the transmission (Tello-Leal and Macías-Hernández 2021) and severity of infection due to COVID-19 (Jiang et al. 2020; Linares et al. 2021; Díaz et al. 2021).
Air pollution and its relationship to COVID-19 is an important area of research, and there has been study of the association between air pollutants such as PM10 and NO2. Some authors have shown that SAR-CoV-2 can attach itself to environmental pollutants such as particulate matter (PM) (Srivastava 2021). In prior studies, PM pollution has been related to infections such as severe acute respiratory syndrome (SARS) (Cui et al. 2003). Some papers reveal that the number of infected people was higher in Italian cities that exceeded the limit established for PM10 and for ozone (Coccia 2021a). It was suggested that pollution could operate as a determining factor for the spread of COVID-19 in society (Coccia 2020a). There has even been investigation of a possible relationship between Saharan dust and the severity of COVID-19 (Linares et al. 2021). Another study showed that 78% of studied regions in Spain, Italy, France, and Germany had both a greater number of cases of mortality due to COVID-19 and higher concentrations of NO2 (Ogen 2020); moreover, a study focus in Catalonia (Spain) showed a statically significant correlation between COVID-19 incidence and NO2 (Marquès et al. 2021). Furthermore, during days with Saharan dust intrusion, there was a greater association between NO2 and the incidence and severity of COVID-19 in eight provinces in Spain (Linares et al. 2021). In relation to the association between air pollution and the incidence and severity of COVID-19, there has also been evidence that noise pollution is a mobility indicator that has been a precursor to increased cases of COVID-19 (Díaz et al. 2021).
Despite the current evidence, there is still a lack of understanding of the association between the meteorological factors, air pollutants, and COVID-19. These differences are in many cases maintained because of methodological deficiencies in the published studies, the majority of which opt to study environmental factors and meteorological factors separately. There are also studies that do not include the incubation period of the disease, which is on average 4 days (2–7 days) (Guan et al. 2020).
There have been contrasting results with respect to meteorological factors such as temperature and COVID-19. While some studies in China mention both a positive and negative relationship, depending on the studied provinces (Shahzad et al. 2020), others show that a lower temperature increases the number of cases of COVID-19 (Şahin 2020; Xie and Zhu 2020) and could result in an increase in the number of deaths due to the disease (Wu et al. 2020). On the other hand, other authors are simply unable to identify any type of correlation between COVID-19 and temperature (Tosepu et al. 2020).
Absolute humidity has been shown to have a weak (not robust) association with COVID-19 in Bangladesh (Islam et al. 2020), Thailand (Sangkham et al. 2021), and Turkey (Şahin 2020). Some authors have shown that the stability of SARS-CoV in climates with low humidity could facilitate the community transmission in subtropical climates in the spring (Chan et al. 2011). Furthermore, laboratory studies have shown that SARS-CoV becomes inactive with greater temperature and humidity (Casanova et al. 2010). In this sense, one study showed that an increase in humidity was related to a decrease in the number of confirmed cases of COVID-19 (Lorenzo et al. 2021). Other authors suggest that SARS-Cov-2 presents a more efficient transmission at low temperature and low humidity, as does influenza (Qi et al. 2020).
Other types of studies, mostly restricted to middle latitudes, have focused on the effect of meteorological factors—such as average temperature and absolute average humidity during the maximum incubation period—on severity and intensity of the disease during its first wave (Burra et al. 2021). Some studies have found a negative correlation between both variables. For example, a study carried out in Spain (Hervella et al., 2021) suggested that meteorological factors could have been more relevant during the initial time of COVID-19, given the lack of significant measures like social distancing and masking.
Although there are papers that analyze both, meteorological factors and air pollutants on COVID-19 incidence (Shen et al. 2021; Rahimi et al. 2021; Diao et al. 2021), there are few focused in the short-term and for a whole country. In light of the absence of studies at the Spanish national level that analyze air pollutants and atmospheric variables in a combined model, the present study was proposed to identify the short-term association between the concentrations of air pollutants (PM10, NO2) and atmospheric variables (maximum daily temperature and absolute average humidity) and the incidence and severity of COVID-19. On the other hand, there are other factors that could influence the transmission of SARS-Cov-2 and affect the development of the disease as the government response policies (Coccia 2020b; Askitas et al. 2021) or health spending (Coccia 2021b). Even some authors propose the creation of an index to quantify environmental risks in relation to other demographic and social factors (Coccia 2020a). In this study, we try to evaluate the influence of some social determinants, and constructed a model that attempts to explain the heterogeneous geographic behavior observed for some of the impacts of the environmental variables.
Material and methods
Sample and data
This study was an ecological, longitudinal retrospective time series study of the period from February 1, 2020 through May 31, 2020. Forty-one of the Spain’s 52 provinces were considered.
Inclusion criteria: the study included those provinces for which there was homogeneous information on average daily concentrations of nitrogen dioxide (NO2), particulate matter with an aerodynamic diameter of less than 10 μm (PM10), and the atmospheric variables maximum daily temperature (Tmax) and absolute average daily humidity (HA). A maximum limit was established for information loss at 10% on the study days.
Measures of variables
Dependent variables
Daily incidence rate of COVID-19 per million inhabitants (TIC) and the rate of hospital admissions due to COVID-19 (TIHC). The dependent variables were calculated based on the number of cases of patients with positive PCR tests (COVID-19) in the provinces analyzed. This information was provided by the National Center for Epidemiology of the Carlos III Health Institute. At the provincial level, the population data were provided by the National Statistics Institute (INE). Based on these data, the following were calculated:
Rate of COVID-19 incidence per 1,000,000 inhabitants: (Number of positive COVID-19 cases/population) × 1,000,000 inhabitants.
Rate of COVID-19 hospital admissions per 1,000,000 inhabitants: (Number of emergency COVID-19 positive hospital admissions/ population) × 1,000,000 inhabitants.
Independent variables
Air pollutants
The average daily values of concentrations of PM10 and NO2 in μg/m3 were calculated, obtained from the representative stations located in the provinces analyzed. These data were provided by the Ministry for Ecological Transition and Demographic Challenge (MITECO).
Meteorological variables
The meteorological data used were the daily values of maximum temperature (Tmax) in °C and absolute average daily humidity (HA) in g/m3 obtained from the reference observatories of each province. As these variables presented the best behavior with the COVID-19 variables analyzed (Linares et al. 2021; Xie and Zhu 2020). The reference observatories belong to the State Meteorological Agency (AEMET).
Based on relative daily humidity (HR) and average daily temperature (T) (Gupta et al., 2020), absolute average humidity (AH) was calculated based on the Clausus Calpeyron equation, as follows (Iribarne and Cho 1980):
Other independent variables
In order to explain the heterogeneity of the geographic distribution of the results obtained from the study of air pollutants and meteorological variables associated with COVID-19, other independent variables were analyzed. These were grouped using the Lalonde Laframboise epidemiological model of health determinants, which classifies variables in terms of those related to human biology, lifestyles, and environment and health services.
Mobility was among the included variables related to lifestyles. Mobility information was extracted from Google (COVID-19 Community Mobility Report, s. f.).
Other variables included the long-term exposure to chemical pollutants, such as the average value of PM2,5, PM10, and NO2 from 2017 to 2019, (informe-calidad-aire-2017.pdf, s. f.) (informe-calidad-aire-2018.pdf, s. f.) (informe-calidad-aire-2019.pdf, s. f.). Other environmental variables were studied such as provinces with airports (Red de aeropuertos - Aena.es, s. f.), number of gasoline cars per inhabitant, number of gas-oil (diesel) cars per inhabitant, and total number of cars excluding zero and low-emissions vehicles (Tablas estadísticas 2019, s. f.).
Social environment variables included rurality (Ocana-Riola and Sanchez-Cantalejo 2005), homes under 30 m2 (to indirectly evaluate the level of overcrowding).
In terms of socioeconomic environment, variables included income level (INEbase / Economía /Cuentas económicas /Contabilidad regional de España / Resultados, s. f.), deprivation index (Duque et al. 2021), and environmental expenditure (SGFAL, s. f.).
The variables related to the response of health systems included number of clinics, number of health centers, average number of ambulances per inhabitant, average number of family physicians per inhabitant, average number of nurses per inhabitant, average number of physicians and nurses per inhabitant (Consulta Interactiva del SNS, s. f.), number of beds per 1000 inhabitants, number of intensive care beds per 1000 inhabitants (Ministerio de Sanidad, Consumo y Bienestar Social - Profesionales - Datos abiertos de capacidad asistencial, s. f.), and number of new social security personnel employed in the past year (05m-Afi. Med. R. General por Provincia-CCAA, y Sección-Actividad, s. f.).
Model and data analysis and procedure
Generalized linear models (GLM) with Poisson link were carried out in the 41 studied provinces, using the rate of positive COVID-19 cases and the rate of hospital admissions as the dependent variables and air pollutants and the meteorological variables as independent variables.
To control for the trend, a variable called n1 was used. This variable was defined as n1 = 1 for February 1, 2020; n2 = 2 for February 2, 2020 and so forth until the end of the period. To control for seasonalities of 4 months (120 days), 3 months (90 days), 2 months (60 days), and 1 month (30 days), the following variables were introduced: sen 120 = sen(2π*n1 (3/365.25), cos 120, sen 90, sen60, and sen30, in addition to the corresponding cosines of the same functions. We also introduced the autoregressive of order 1 of the corresponding dependent variable.
GLM were carried out between the dependent variables and the values of the independent variables, to establish days with statistically significant lags between both variables.
In the case of Tmax and HA, the lags were considered statistically significant starting with the 5th day, up to the 28th. The existing literature does not indicate that temperature or humidity can worsen the symptoms of the disease in an immediate way; rather, they can influence the possibility of infection by the virus, whose incubation period has been established at around 5 days. Along the same lines, some authors have found a greater correlation after the fifth day (Bolaño-Ortiz et al. 2020a).
On the contrary, air pollution can contribute to worsening the symptoms of respiratory and circulatory illnesses, and in consequence, it could cause patients to seek out health services to get a PCR test. A positive result is considered a case of COVID-19 for the same day (Domingo et al., 2020). Therefore, in order to study the impact of the concentrations of PM10 and NO2, lags from day 0 through day 28 were considered.
For the purposes of the analysis, a range of lag days was established of between 0 and 28 days, from the onset of symptoms until the worsening of the disease and admission to the hospital (Lauer et al. 2020). A weekly distribution model of lags was used (Linares et al. 2021) (Díaz et al. 2021). In a first step, the lags corresponding to the independent variables were introduced, with lags of 0 to 7 days. Second, lags of 8 to 14 days were introduced, maintaining the lags of the variables that were found to be statistically significant in step one, and so on, up to 28 days.
All of the independent and dependent variables were introduced into the same model. Relative risks (RR) were calculated using the estimators obtained, based on the absolute value of the estimators, as follows: RR = eβ where β is the absolute value of the estimator.
If the coefficient of the estimator was negative, it would indicate that an increase in the dependent variable is associated with a decrease in the independent variable. The RR was calculated using an increase of 10 μg/m3 in PM10 and NO2; of 1 °C in the case of Tmax and 1 g/m3 for AH.
Based on the risks obtained, the attributable risk (RA) was calculated for some of the provinces, based on the following formula: AR = 100*(RR-1)/RR, which permitted calculating the incidence of each of the significant independent variables at the population level. RA has been calculated as an example, only for some of the provinces.
In order to explain the heterogeneity of the geographic distribution of the results, we carried out a linear regression model that included the other intervening independent variables already described, using the following function:
where Y = risks associated with NO2, PM10, Tmax, and HA for each studied province; y x1j + x2j … xkj, represent the intervening independent variables.
Ethical considerations
Working with aggregated and anonymous data did not require the approval of the ethics committee; however, this study complied with the ethical considerations of the Declaration of Helsinki.
Software
SPSS 27.0 and Stata 16.0 were used for the analysis of the time series. Maps were developed using Qgis 3.16.3, and tables were constructed using Excel.
Results
Table 1 shows the Spanish provinces studied and the days for which there was an association or lag (Lag) with TIC and with TIHC, for the environmental pollutants (PM10, NO2) and for the atmospheric variables (Tmax y AH). The day of the lag shown to be statistically significant is shown in parenthesis.
In the case of TIC, only one province failed to show a lag associated with environmental pollutants or the atmospheric variables. In the case of the hospital admissions rate, 10 of the studied provinces did not produce any type of associated lag (see Fig. 1).

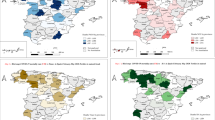
Maps of Relative Risks to air pollutants and meteorological variables associated with the rate of incidence of COVID-19 (TIC) in Spain* during First Wave (Feb-May 2020). *Study provinces: 41 of 52 provinces in Spain. Not all provinces were studied due to lack of information
Figures 1 and 2 and Supplementary Table 1 show the RR by province, associated with TIC and TIHC, by air pollutants and atmospheric variables. The maps show the different associations with RR stratified by terciles in natural breaks.

Maps of Relative Risks to air pollutants and meteorological variables associated with the hospital admission rate of COVID-19 (TIHC) in Spai* during First Wave (Feb-May 2020) *Studied provinces: 41 of 52 provinces in Spain. Not all provinces were studied due to lack of information
Figure 1 shows that the provinces that present a greater number of RR associated with PM10 are found in tercile 2, and the RR present a range of between 1015 and 1050. In order to understand the contribution of PM10 to TIC, by way of example, we can say that the province with the greatest value of RR associated with PM10 in Spain presented an RR of 1103 (1009–1198) (see Supplementary Table 1). That is to say that for each 10 °μg/m3 increase in PM10, the attributable risk (AR) of PM10 to TIC is 9.4%.
The province of Lugo, located in the Northwest of Spain, was the province with the greatest value of RR associated with TIC and NO2 (RR: 2,807 (1038–4575) (see Supplementary Table 1). The TIC of the provinces with the greatest values of RR associated with NO2 are found in the first tercile, with RR with a range of 1000 to 1109 (see Fig. 1).
Figure 1 highlights the greatest number of provinces with RR associated with TIC and temperature, which can be found in tercile 1, with RR that ranging between 1022 and 1055.
In Fig. 1, the provinces with RR associated with TIC and HA that present the highest values—that is to say, tercile 1 (RR that range between 1477 and 2043) and tercile 2 (RR from 1477 to 2043)—are concentrated in the Northwest zone of Spain.
In general, TIHC presented a lower number of associated provinces, both for the air pollutants as well as the atmospheric variables, as shown in Fig. 2.
In Fig. 2, it can be observed that 3 of the 5 provinces with the greatest RR values associated with TIHC and PM10 (tercile 1: RR of 1071 to 1127 and tercile 2: RR of 1031 to 1070) are found in the Northwest of Spain.
The greatest number of provinces that presented an association between TIHC and TIHC and NO2 can be found in tercile 1 (with values of RR that range between 1018 and 1079) (see Fig. 2).
There is a somewhat heterogeneous geographic distraction of the provinces that presented RR associated with TIHC and temperature in all of the country (see Fig. 2).
Figure 2 shows that the provinces that presented the highest values of RR associated with TIHC and HA (tercile 1 (RRs of 1576 to 1871) and tercile 2 (RRs of 1231 to 1575)) are found in the North and Northwest of Spain.
Table 2 shows that the majority of the provinces (81%) presented a significant association between TIC and NO2. In the same sense, 49% of the provinces presented an association between TIHC and NO2, with NO2 being the chemical pollutant with more association, both with TIC and TIHC.
In order to explain the geographic differences observed at the country level, shown in Figs. 1 and 2, other health determinants were analyzed (see Supplementary Table 2) using linear regression.
Table 3 shows the analysis of the correlation between the RR of association between air pollutants and meteorological variables associated with TIC or TIHC and the determinants of health. The positive correlations (positive coefficients) indicate that when the studied variables increase, so does the health determinant; if the correlation is negative (negative coefficient), a decrease in the studied variables would indicate an increase in the health determinant, and vice versa.
Discussion
The following sections are divided according the findings obtained for the incidence rate (TIC) and hospital admission rate (TIHC) of COVID-19 and the principal variables analyzed: air pollutants, meteorological variables and social factors.
Findings obtained for NO2
NO2 was the pollutant with the greatest number of provinces associated with TIC. About 81% of the provinces presented an association between the concentrations of NO2 and TIC. Forty-nine percent of the provinces presented an association between NO2 and TIHC. These findings agree with other research carried out in the United Kingdom (UK) (Travaglio et al. 2021), in China (Zhu et al. 2020) in Wuhan (Jiang et al. 2020), and even in Catalonia (Spain) (Marquès et al. 2021). A study of Saharan dust intrusions and COVID-19 carried out in eight Spanish cities also identified a greater number of cities with an association between NO2 and TIC (Linares et al. 2021). In our study, the province with the greatest RR associated with NO2 and TIC was the province of Lugo (see Map 1b), and the lags were significant between 0 and 14 days. The lags reflect the days prior to the start of symptoms that present an association with NO2, which is related to the incubation period of the disease, and these days coincide with the physiopathology of the virus. In a study carried out in Italy, a correlation was shown between TIC and the concentrations of NO2, with hotspots identified in the North of Italy and the urban areas of the Center and South of Italy, such as Rome and Naples (Fattorini and Regoli 2020). In this study, there was no identified pattern in terms of geographic zone (see maps 1 and 2).
With respect to the mechanism of action of NO2 and its relationship with the virus, it has been shown that environments with a greater concentration of NO2 can influence infiltration of airways by inflammatory cells (Ghio et al. 2000). Furthermore, it is believed that the exposure to NO2 inhibits the microbiome response and reduces the possibility of eliminating the virus in the lungs, which in consequence reduces its effectiveness (Lundborg et al. 2006). Also, it has been shown that the acute exposure to nitrogen oxides decreases pulmonary function through the mechanism of oxidative stress (Guarnieri and Balmes 2014). On the other hand, NO2 has been associated with an increase in medical visits and hospitalizations due to bronchitis and exacerbations of asthma (Bahrami Asl et al. 2018). It has been suggested that the angiotensin-converting enzyme (ACE2) may act as a receptor for SAR-CoV-2 (Lamas-Barreiro et al. 2020) (Yan et al. 2020). In other words, SAR-CoV-2 may interfere with the action of the ACE2 enzyme (Alifano et al. 2020). One study established a possible role of NO2 in interfering with ACE2 due to the fact that there is a high quantity of ACE2 in epithelial cells of the lung (Alifano et al. 2020). Thus, SAR-CoV-2 may interfere in the action of ACE2, as may NO2, but through different mechanisms. The interference results in difficulty in the degradation of ACE2 and accumulation of angiotensin II, substances that ACE2 acts upon. During COVID-19 infection, the alteration of ACE2 generates a disequilibrium in the inflammatory system involving an imbalance of vasoconstrictors, pro-inflammatory, proliferative, profibrotic, and oxidants, which could make the disease more severe. Although NO2 levels decreased dramatically during the lock down period (Querol et al. 2021), the analysis of long-term exposure has also shown that NO2 increases the risk of positive cases for COVID-19 (Saez et al. 2020).
Findings obtained for PM10
PM10 was associated with TIC in 63% of the studied provinces. It is known that the origin of the emission of PMs is 55% related to road traffic (Querol 2012) and is considered to be exclusively an oil product/fossil fuel (a product derived from gasoline and diesel fuel) (Lozhkina et al. 2016). Prior to COVID-19, it was shown that PM results in risks to health, especially respiratory infections, asthma, chronic obstructive disease, and lung cancer (Kim et al. 2018). It is known that PM10 and PM2.5 particles can be inhaled and penetrate the lungs and circulatory system, producing difficulty in breathing, cough, and circulatory system irritation (Kim et al. 2018). In the case of TIC, a study showed a positive relationship between the number of people infected and the provinces with daily concentrations of PM10 over 50 μg/m3 up to 14 days prior to the start of the infection (Setti et al. 2020). These results coincide with ours, because we have identified that many of the lags are found between 1 and 14 days. Another study mentioned that depending on the province, there are different thresholds at which PM2.5 and PM10 could be associated with the severity or mortality of COVID-19 (Magazzino et al. 2020), which agrees with our findings that identify different RR in the different study provinces (see Map 1 and Map 2, see Supplementary Table 1).
Some studies have identified that the number of infected people may increase in cities where the limit established for PM10 and Ozone levels exceed the WHO guidelines in a significant number of days (Coccia 2021a; Saez et al. 2020; Bashir et al. 2020). Our study also controlled for long-term exposure, including the average concentration of PM10 from 2017 to 2019 for PM10 and PM2.5; however, no association was identified when these variables were included in the final GLM model for each province.
Findings obtained for maximum daily temperature (Tmax)
Some authors consider that temperature could influence the transmission of SAR-CoV-2 (Chen et al. 2020). Other authors mention a different sort of correlation with the dissemination of the virus (Poole 2020). An Italian study identified a positive correlation between temperature and the number of cases of COVID-19 (Zoran et al. 2020), a similar relation was identified in 122 Chinese cities (Xie and Zhu 2020), other authors have identified with SARS-CoV transmission in Hong Kong and Beijin in 2003 (Bi et al. 2007). In the case of the first wave in Spain, 70.73% of the studied provinces presented a negative association between temperature and TIC (transmission), and 36.59% presented a negative association between temperature and TIHC (severity) (see Table 2). In Spain, a strong negative correlation has been found between the expansion and severity of the disease and temperature and humidity during the time just before the outbreak of the epidemic (Luna 2021). Similar results come from other studies that are restricted to middle latitudes during the initial period of the disease (Burra et al. 2021).
Studies of temperatures show varied results. One study that included tropical zones identified a negative correlation between the number of new cases and temperature (Bolaño-Ortiz et al. 2020a). Another study carried out in China did not identify a linear relationship between temperature and the number of COVID-19 cases (Xie and Zhu 2020). Despite the fact that studies have shown that high temperatures and humidity reduce transmission of diseases like the flu and the SARs coronavirus in the respiratory tract (Park et al. 2020) (Sarkodie and Owusu 2020), evidence of the true role of temperature on SAR-CoV-2 in still inadequate (Mecenas et al. 2020) (see Maps 1c and 2c).
Findings obtained for absolute humidity
Absolute humidity (AH) was the variable that presented the lowest percentage of provinces associated with TIHC (21.95%), and there was a negative association. A study in China found that HA produced negative effects on confirmed cases of COVID-19 (Liu et al. 2020). However, another study did not shown an association between HA and TIC (Araújo and Naimi 2020). Despite the fact that laboratory studies show that the transmission of SARS-CoV is more likely to be inactivated at higher temperatures and humidity (Qi et al. 2020), another study in Bangladesh identify a negative relation between humidity and temperature and the COVID-19 transmission; however, authors recognize that transmission during the summer period increased (Haque and Rahman 2020). Recent studies have not identified an association between humidity and the number of COVID-19 cases (Jiang et al. 2020). Even one study that analyzed levels of extreme humidity was unable to demonstrate inactivation of the virus (Luo et al. 2020), which confirms that there are differences between SARS-CoV-2 and other respiratory viruses. In addition, a study carried out during different seasons of the year suggested that it is possible that COVID-19 may not disappear on its own in warmer or more humid climates (Yuan et al. 2021) (see Maps 1d and 2d).
We can infer from the results of this study that both temperature and humidity play a secondary role, due to a lower number of provinces that presented an association in the GLM models (see Table 2, Maps 1c, 1d and 2c, 2d).
Despite the fact that some studies have proposed that the northern or coastal zones of some countries (Fattorini and Regoli 2020) were more affected by COVID-19. Other authors have proposed that some cities of the Italian coast are windy and showed a lower number of infected people; however, the risk of infection continued to be high due to the high percentage of the elderly population among other reasons (Coccia 2021d). In Barcelona, clusters with a greater number of infected patients were identified (Saez et al. 2020).
Our results point to a greater number of provinces with RR associations between TIC and AH in the Northwest (see Map 1d) and a greater number of provinces with RR associations between TIHC and PM10 in the Northwest (see Map 2a) and TIHC and HA in the North and Northwest in Spain (see Map 2d). However, we have not identified zones with a marked geographic concentration, from which we can infer that some geographic zones are much more affected than others. Thus, in general, there is a great deal of heterogeneity in the geographic distribution of the RR associated with TIC and TIHC in Spain. The geographic differences could probably be partly explained by the fact that the confinement altered the natural propagation of the virus, precluding a homogeneous distribution among all of the provinces and altering the pattern of comparison during the study period, which corresponded to the first wave of the virus in Spain.
On the other hand, during the first wave, there were insufficient tests to diagnose all of the positive cases of COVID-19. Symptomatic patients were prioritized; however, one in three patients with COVID-19 remained asymptomatic (Pollán et al. 2020). This difference could also have altered the geographic distribution of the results.
Because our results did not explain the heterogeneity in the geographic distribution of the RR association with TIC and TIHC, we carried out a complementary analysis with other health determinants, using the Lalonde Laframboise model (see Supplementary Table 2).
Findings obtained for social factors
TIC and social factors
TIC associated with PM10 presented a negative correlation with per capita income. It has already been suggested that the periodic appearance of other infectious disease viruses negatively correlate with socioeconomic, environmental and ecological factors (Jones et al. 2008; Coccia 2020a). One study showed that low poverty rates are related to high TIC (Bolaño-Ortiz et al. 2020b). Another study suggested that municipalities with a medium-low income level presented a greater number of mortal cases of COVID-19 (Olulana, s. f.). There has been a study of the fact that municipalities in rural areas tend to have poorer health outcomes (Anderson et al. 2015; You et al. 2020). A study in Italy concludes that a high gross domestic product per capita, high healthcare spending, and low levels of air pollution even could to reduce the mortality attributable to COVID-19 (Coccia 2021b). However, our study was not able to corroborate the association between the rural/urban variable and TIC or TIHC. Some studies have even proposed race as a risk factor in increases in TIC (Millett et al. 2020), though our study did not explore race.
The presence of airports presented a positive correlation with TIC associated with PM10. A short-term effect of PM10 has been identified, derived from air traffic, on pulmonary function in adults with asthma living near an airport in the USA (Habre et al. 2018). However, studies carried out at the airport in Barcelona have not been able to attribute the increase in PM10 only to the presence of the airport (Amato et al. 2010). Thus, these findings, though interesting, should be interpreted with prudence.
With respect to the positive correlation between TIC associated with NO2 and the number of diesel cars, it is well-known that an important source of NO in urban areas is transportation emissions, diesel combustion, and domestic heating (Grange et al. 2019), which would seem to confirm that our association is not random. Our study included NO2 pollution levels at least 14 days before the beginning of the first wave, thus we can say that average pollution levels included mobility that was prior to the first wave. However, the confinement could have altered these results. Despite the fact that the confinement could have been a modifying factor of the effect, NO2 was associated in the majority of the studied provinces. This association was confirmed with the correlation with the number of diesel cars, which is one of the primary sources of NO2 pollution.
TIHC and social factors
The decrease in nursing personnel per person could increase the risks of the association between TIHC and PM10. In the same way, a positive relationship has been identified with the number of new health personnel. In terms of health personnel, different studies have shown a negative association with cases of death due to COVID-19 (Perone 2021). It should be noted that, considering the severity of patients admitted with COVID-19, the results are highly coherent, as PM10 has already been associated in other studies with an increase in hospitalizations of children due to respiratory viruses, such as respiratory syncytial virus (Zhu et al. 2020). However, there is less evidence in adults.
We observed that the presence of a lower number of homes under 30 m2 could increase the risk of association between TIHC and temperature. In this sense, the majority of the literature does not identify a relationship between temperature and hospital admissions due to COVID-19. However, it is probable that the presence of low temperatures during the first wave in Spain gave way to greater probability of overcrowding in homes under 30 m2. Similar results have been published in the USA (Ahmad et al. 2020) and in China (indoor) (Qian et al. 2021). On the other hand, there is currently more evidence about the airborne transmission of respiratory virus (Wang et al. 2021); in this context, the presence of air conditioning or inadequate ventilation could contribute to the airborne transmission of viruses in indoor environments, which could also have contributed to the increase in the association between TIHC and temperature (Li et al. 2007).
Limitations
We are aware that some variables related to human biology, such as sex or age, could not be measured due to the lack of a database that grouped this information for each Spanish province.
In addition, the lack of a polymerase chain reaction-tests and its heterogeneous provincial distribution is an important bias that may condition the results of this study, especially in the incidence rate.
The period of confinement affected the exposure to pollutants (Xu et al. 2020; Querol et al. 2021; Rahimi et al. 2021) and to environmental variables in all of the provinces, above all in the provinces with a very low incidence. This decrease in air pollution levels as a consequence of confinement may affect the association that may exist between air pollution and COVID-19.
Meteorological variables not only include variables such as temperature and absolute humidity, there are other variables such as those considered here; there are also studies that analyze the possible incidence of wind speed and wind direction (Coccia 2021c) (Coccia 2020c) (Islam et al. 2021) as well as solar radiation or precipitation (Rosario et al., 2020). However, in our study, some of these variables were not available for all the provinces studied.
Our study is limited to the first wave, and it is in this context that the results should be interpreted.
Conclusion
This is the first Spanish study that identifies a joint model of exposure risk at the province level for both air pollutants and meteorological variables on TIC and TIHC including an analysis by health determinants. The role of NO2 is worth highlighting among the air pollutants, as it is the chemical pollutant that presented the greatest number of provinces associated with TIC and TIHC. The role of meteorological variables temperature and AH was not robust in relation to the air pollutants. The geographic distribution of the RR identified was highly heterogeneous, and this study was unable to explain this geographic distribution, despite including other social determinants.
The health impact of epidemics does not only depend on biological and environmental factors. This study shows that environmental factors considered can modulate the incidence and severity of the pandemic; they are not determining factors that can explain by themselves the development and evolution of COVID-19. There are also economic and social factors that can alter the course of the epidemic (Coccia 2021e).
In addition, non-pharmacological public health measures such as the use of a mask, ventilation of outdoor spaces, and social distancing are proving highly effective for the control of COVID-19. Especially in places where, for many hours, a large number of people live in confined spaces such as schools (Villanueva et al. 2021). Despite the limited effect of air pollution on the incidence and severity of COVID-19 in this analysis, it is evident that the scientific literature shows the existence of robust associations. These associations at the short- and long-term support that the decrease in air pollution levels results in an improvement in the health of the population. The use of technologies that reduce social inequalities and sustainable development (Coccia 2020c) are key to the fight against this pandemic, especially in large cities.
Data availability
It is an ecological analysis, so the study does not involve human subjects. The data in relation to COVID-19 used in this study are subject to statistical secrecy and, therefore, are not freely available
Change history
26 March 2022
A Correction to this paper has been published: https://doi.org/10.1007/s11356-022-19937-x
References
05m-Afi. Med. R. General por Provincia-CCAA, y Sección-Actividad. (s. f.) (2021) PxWeb. Recuperado 6 de julio de 2021, de http://w6.seg-social.es/PXWebPXWeb/pxweb/es/Afiliadosenaltalaboral/Afiliadosenaltalaboral__AfiliadosMedios/05m-Afi.Med.R.GeneralporProvincia-CCAAySección-Actividad.px/
Accinelli RA, Leon-Abarca JA (2020) En la altura la COVID-19 es menos frecuente: La experiencia del Perú. Archivos de Bronconeumología 56(11):760–761. https://doi.org/10.1016/j.arbres.2020.06.015
Ahmad K, Erqou S, Shah N, Nazir U, Morrison AR, Choudhary G, Wu W-C (2020) Association of poor housing conditions with COVID-19 incidence and mortality across US counties. PLOS ONE 15(11):e0241327. https://doi.org/10.1371/journal.pone.0241327
Alifano M, Alifano P, Forgez P, Iannelli A (2020) Renin-angiotensin system at the heart of COVID-19 pandemic. Biochimie 174:30–33. https://doi.org/10.1016/j.biochi.2020.04.008
Amato F, Moreno T, Pandolfi M, Querol X, Alastuey A, Delgado A, Pedrero M, Cots N (2010) Concentrations, sources and geochemistry of airborne particulate matter at a major European airport. J Environ Monit 12(4):854. https://doi.org/10.1039/b925439k
Anderson TJ, Saman DM, Lipsky MS, Lutfiyya MN (2015) A cross-sectional study on health differences between rural and non-rural U.S. counties using the County Health Rankings. BMC Health Serv Res 15(1):441. https://doi.org/10.1186/s12913-015-1053-3
Araújo MB, Naimi B (2020) Spread of SARS-CoV-2 Coronavirus likely constrained by climate. MedRxiv 2020(03):12.20034728. https://doi.org/10.1101/2020.03.12.20034728
Askitas N, Tatsiramos K, Verheyden B (2021). Estimating worldwide effects of non-pharmaceutical interventions on COVID-19 incidence and population mobility patterns using a multiple-event study. Sci Rep 11 (1), art. no. 1972.
Bahrami Asl F, Leili M, Vaziri Y, Salahshour Arian S, Cristaldi A, Oliveri Conti G, Ferrante M (2018) Health impacts quantification of ambient air pollutants using AirQ model approach in Hamadan. Iran. Environ Res 161:114–121. https://doi.org/10.1016/j.envres.2017.10.050
Bashir MF, Ma BJ, Bilal K, Bashir MA, Farooq TH, Iqbal N, Bashir M (2020) Correlation between environmental pollution indicators and COVID-19 pandemic: a brief study in Californian context. Environ Res 187:109652. https://doi.org/10.1016/j.envres.2020.109652
Bi P, Wang J, Hiller JE (2007) Weather: Driving force behind the transmission of severe acute respiratory syndrome in China? Intern Med J 37(8):550–554. https://doi.org/10.1111/j.1445-5994.2007.01358.x
Bolaño-Ortiz TR, Camargo-Caicedo Y, Puliafito SE, Ruggeri MF, Bolaño-Diaz S, Pascual-Flores R, Saturno J, Ibarra-Espinosa S, Mayol-Bracero OL, Torres-Delgado E, Cereceda-Balic F (2020a) Spread of SARS-CoV-2 through Latin America and the Caribbean region: a look from its economic conditions, climate and air pollution indicators. Environ Res 191:109938. https://doi.org/10.1016/j.envres.2020.109938
Bolaño-Ortiz TR, Camargo-Caicedo Y, Puliafito SE, Ruggeri MF, Bolaño-Diaz S, Pascual-Flores R, Saturno J, Ibarra-Espinosa S, Mayol-Bracero OL, Torres-Delgado E, Cereceda-Balic F (2020b) Spread of SARS-CoV-2 through Latin America and the Caribbean region: a look from its economic conditions, climate and air pollution indicators. Environ Res 191:109938. https://doi.org/10.1016/j.envres.2020.109938
Burra P, Soto-Díaz K, Chalen I, Gonzalez-Ricon RJ, Istanto D, Caetano-Anollés G (2021) Temperature and latitude correlate with SARS-CoV-2 epidemiological variables but not with genomic change worldwide. Evol Bioinformatics 17:1176934321989695. https://doi.org/10.1177/1176934321989695
Casanova LM, Jeon S, Rutala WA, Weber DJ, Sobsey MD (2010) Effects of air temperature and relative humidity on coronavirus survival on surfaces. Applied and Environmental Microbiology 76(9):2712–2717. https://doi.org/10.1128/AEM.02291-09
Coccia M (2020a) An index to quantify environmental risk of exposure to future epidemics of the COVID-19 and similar viral agents: theory and practice. Environ Res 191:110155. https://doi.org/10.1016/j.envres.2020.110155
Coccia M (2020b) Factors determining the diffusion of COVID-19 and suggested strategy to prevent future accelerated viral infectivity similar to COVID. Sci Total Environ 729:138474. https://doi.org/10.1016/j.scitotenv.2020.138474
Coccia M (2020c) How (Un)sustainable environments are related to the diffusion of COVID-19: the relation between coronavirus disease 2019, air pollution, wind resource and energy. Sustainability 12(22):9709. https://doi.org/10.3390/su12229709
Coccia M (2021a) Effects of the spread of COVID-19 on public health of polluted cities: Results of the first wave for explaining the dejà vu in the second wave of COVID-19 pandemic and epidemics of future vital agents. Environ Sci Pollut Res 28(15):19147–19154. https://doi.org/10.1007/s11356-020-11662-7
Coccia M (2021b) High health expenditures and low exposure of population to air pollution as critical factors that can reduce fatality rate in COVID-19 pandemic crisis: a global analysis. Environ Res 199:111339. https://doi.org/10.1016/j.envres.2021.111339
Coccia M (2021c) The effects of atmospheric stability with low wind speed and of air pollution on the accelerated transmission dynamics of COVID-19. Int J Environ Stud 78(1):1–27. https://doi.org/10.1080/00207233.2020.1802937
Coccia M (2021d) How do low wind speeds and high levels of air pollution support the spread of COVID-19? Atmos Pollut Res 12(1):437–445. https://doi.org/10.1016/j.apr.2020.10.002
Coccia M (2021e) The impact of first and second wave of the COVID-19 pandemic in society: comparative analysis to support control measures to cope with negative effects of future infectious diseases. Environ Res 197:111099. https://doi.org/10.1016/j.envres.2021.111099
Chan KH, Peiris JSM, Lam SY, Poon LLM, Yuen KY, Seto WH (2011) The effects of temperature and relative humidity on the viability of the SARS coronavirus. Adv Virol 2011:734690. https://doi.org/10.1155/2011/734690
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L (2020) Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet 395(10223):507–513. https://doi.org/10.1016/S0140-6736(20)30211-7
Consulta Interactiva del SNS. (s. f.). Recuperado 6 de julio de 2021, de https://pestadistico.inteligenciadegestion.mscbs.es/publicoSNS/C/sistema-de-informacion-de-atencion-primaria-siap/recursos/estructurales
COVID-19 Community Mobility Report. (s. f.). COVID-19 Community Mobility Report. Recuperado 6 de julio de 2021, de https://www.google.com/covid19/mobility?hl=en
Cucinotta D, Vanelli M (2020) WHO Declares COVID-19 a Pandemic. Acta Bio Medica Atenei Parmensis 91(1):157–160. https://doi.org/10.23750/abm.v91i1.9397
Cui Y, Zhang Z-F, Froines J, Zhao J, Wang H, Yu S-Z, Detels R (2003) Air pollution and case fatality of SARS in the People’s Republic of China: an ecologic study. Environ Health: A Glob Access Sci Source 2(1):15. https://doi.org/10.1186/1476-069X-2-15
Díaz J, Antonio-López-Bueno J, Culqui D, Asensio C, Sánchez-Martínez G, Linares C (2021) Does exposure to noise pollution influence the incidence and severity of COVID-19? Environ Res 195:110766. https://doi.org/10.1016/j.envres.2021.110766
Diao Y, Kodera S, Anzai D, Rashed EA, Hirata A (2021) Influence of population density, temperature, and absolute humidity on spread and decay durations of COVID-19: A comparative study of scenarios in China, England, Germany, and Japan. One Health 12:100203
Duque I, Domínguez-Berjón MF, Cebrecos A, Prieto-Salceda MD, Esnaola S, Calvo Sánchez M, Marí-Dell’Olmo M (2021) Índice de privación en España por sección censal en 2011. Gaceta Sanitaria 35(2):113–122. https://doi.org/10.1016/j.gaceta.2019.10.008
Fattorini D, Regoli F (2020) Role of the chronic air pollution levels in the Covid-19 outbreak risk in Italy. Environ Pollut 264:114732. https://doi.org/10.1016/j.envpol.2020.114732
Ghio AJ, Kim C, Devlin RB (2000) Concentrated ambient air particles induce mild pulmonary inflammation in healthy human volunteers. Am J Respir Crit Care Med 162(3):981–988. https://doi.org/10.1164/ajrccm.162.3.9911115
Grange SK, Farren NJ, Vaughan AR, Rose RA, Carslaw DC (2019) Strong Temperature Dependence for Light-Duty Diesel Vehicle NOx Emissions. Environ Sci Technol 53(11):6587–6596. https://doi.org/10.1021/acs.est.9b01024
Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, Liu L, Shan H, Lei C, Hui DSC, Du B, Li L, Zeng G, Yuen K-Y, Chen R, Tang C, Wang T, Chen P, Xiang J et al (2020) Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med 382(18):1708–1720. https://doi.org/10.1056/NEJMoa2002032
Guarnieri M, Balmes JR (2014) Outdoor air pollution and asthma. The Lancet 383(9928):1581–1592. https://doi.org/10.1016/S0140-6736(14)60617-6
Habre R, Zhou H, Eckel SP, Enebish T, Fruin S, Bastain T, Rappaport E, Gilliland F (2018) Short-term effects of airport-associated ultrafine particle exposure on lung function and inflammation in adults with asthma. Environ Intern 118:48–59. https://doi.org/10.1016/j.envint.2018.05.031
Haque SE, Rahman M (2020) Association between temperature, humidity, and COVID-19 outbreaks in Bangladesh. Environ Sci Policy 114:253–255. https://doi.org/10.1016/j.envsci.2020.08.012
INEbase / Economía /Cuentas económicas /Contabilidad regional de España / Resultados. (s. f.). INE. Recuperado 6 de julio de 2021, de https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736167628&menu=resultados&idp=1254735576581
Informe-calidad-aire-2017.pdf. (s. f.) (2017) Recuperado 15 de junio de 2021, de https://www.ecologistasenaccion.org/wp-content/uploads/2018/06/informe-calidad-aire-2017.pdf
Informe-calidad-aire-2018.pdf. (s. f.) (2018) Recuperado 15 de junio de 2021, de https://www.ecologistasenaccion.org/wp-content/uploads/2019/06/informe-calidad-aire-2018.pdf
Informe-calidad-aire-2019.pdf. (s. f.) (2019).
Iribarne, J. V., & Cho, H.-R. (1980). Atmospheric thermodynamics and vertical stability. En J. V. Iribarne & H.-R. Cho (Eds.), Atmospheric Physics (pp. 79-96). Springer Netherlands. https://doi.org/10.1007/978-94-009-8952-8_4.
Islam ARMT, Hasanuzzaman M, Azad MAK, Salam R, Toshi FZ, Khan MSI, Alam GMM, Ibrahim SM (2020) Effect of meteorological factors on COVID-19 cases in Bangladesh. Environ Dev Sustain 1-24. https://doi.org/10.1007/s10668-020-01016-1
Islam N, Bukhari Q, Jameel Y, Shabnam S, Erzurumluoglu AM, Siddique MA, Massaro JM, D’Agostino RB (2021) COVID-19 and climatic factors: A global analysis. Environ Res 193:110355. https://doi.org/10.1016/j.envres.2020.110355
Jiang Y, Wu X-J, Guan Y-J (2020) Effect of ambient air pollutants and meteorological variables on COVID-19 incidence. Infect Control Hosp Epidemiol 41(9):1011–1015. https://doi.org/10.1017/ice.2020.222
Jones KE, Patel NG, Levy MA, Storeygard A, Balk D, Gittleman JL, Daszak P (2008) Global trends in emerging infectious diseases. Nature 451(7181):990–993. https://doi.org/10.1038/nature06536
Kim D, Chen Z, Zhou L-F, Huang S-X (2018) Air pollutants and early origins of respiratory diseases. Chron Dis Transl Med 4(2):75–94. https://doi.org/10.1016/j.cdtm.2018.03.003
Lamas-Barreiro JM, Alonso-Suárez M, Fernández-Martín JJ, Saavedra-Alonso JA (2020) Supresión de angiotensina II en la infección por el virus SARS-CoV-2: Una propuesta terapéutica. Nefrología 40(3):213–216. https://doi.org/10.1016/j.nefro.2020.04.006
Lauer SA, Grantz KH, Bi Q, Jones FK, Zheng Q, Meredith HR, Azman AS, Reich NG, Lessler J (2020) The incubation period of coronavirus disease 2019 (COVID-19) from publicly reported confirmed cases: estimation and application. Ann Intern Med https://doi.org/10.7326/M20-0504
Li Y, Leung GM, Tang JW, Yang X, Chao CYH, Lin JZ, Lu JW, Nielsen PV, Niu J, Qian H, Sleigh AC, Su H-JJ, Sundell J, Wong TW, Yuen PL (2007) Role of ventilation in airborne transmission of infectious agents in the built environment—a multidisciplinary systematic review. Indoor Air 17(1):2–18. https://doi.org/10.1111/j.1600-0668.2006.00445.x
Linares, C., Culqui, D., Belda, F., López-Bueno, J. A., Luna, Y., Sánchez-Martínez, G., Hervella, B., & Díaz, J. (2021). Impact of environmental factors and Sahara dust intrusions on incidence and severity of COVID-19 disease in Spain. Effect in the first and second pandemic waves. Environ Sci Pollut Res International. https://doi.org/10.1007/s11356-021-14228-3.
Liu J, Zhou J, Yao J, Zhang X, Li L, Xu X, He X, Wang B, Fu S, Niu T, Yan J, Shi Y, Ren X, Niu J, Zhu W, Li S, Luo B, Zhang K (2020) Impact of meteorological factors on the COVID-19 transmission: a multi-city study in China. Sci Total Environ 726:138513. https://doi.org/10.1016/j.scitotenv.2020.138513
Lorenzo JSL, Tam WWS, Seow WJ (2021) Association between air quality, meteorological factors and COVID-19 infection case numbers. Environ Res 197:111024. https://doi.org/10.1016/j.envres.2021.111024
Lotfi et al. - 2020—COVID-19 Transmission, prevention, and potential .pdf. (s. f.).
Lozhkina O, Lozhkin V, Nevmerzhitsky N, Tarkhov D, Vasilyev A (2016) Motor transport related harmful PM2.5 and PM10: From onroad measurements to the modelling of air pollution by neural network approach on street and urban level. J Phys Conf Ser 772:012031. https://doi.org/10.1088/1742-6596/772/1/012031
Luna MY (2021) Spatial Variability of COVID-19 First wave severity and transmission intensity in Spain: the influence of meteorological factors. Biomed J Sci Tech Res 35(2). https://doi.org/10.26717/BJSTR.2021.35.005667
Lundborg M, Dahlén S-E, Johard U, Gerde P, Jarstrand C, Camner P, Låstbom L (2006) Aggregates of ultrafine particles impair phagocytosis of microorganisms by human alveolar macrophages. Environ Res 100(2):197–204. https://doi.org/10.1016/j.envres.2005.08.007
Luo C, Yao L, Zhang L, Yao M, Chen X, Wang Q, Shen H (2020) Possible transmission of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in a public bath center in Huai’an, Jiangsu Province. China. JAMA Network Open 3(3):e204583. https://doi.org/10.1001/jamanetworkopen.2020.4583
Magazzino C, Mele M, Schneider N (2020) The relationship between air pollution and COVID-19-related deaths: an application to three French cities. Appl Energy 279:115835. https://doi.org/10.1016/j.apenergy.2020.115835
Marquès M, Rovira J, Nadal M, Domingo JL (2021) Effects of air pollution on the potential transmission and mortality of COVID-19: a preliminary case-study in Tarragona Province (Catalonia, Spain). Environ Res 192:110315. https://doi.org/10.1016/j.envres.2020.110315
Mecenas P, Bastos RTDRM, Vallinoto ACR, Normando D (2020) Effects of temperature and humidity on the spread of COVID-19: A systematic review. PLOS ONE 15(9):e0238339. https://doi.org/10.1371/journal.pone.0238339
Millett GA, Jones AT, Benkeser D, Baral S, Mercer L, Beyrer C, Honermann B, Lankiewicz E, Mena L, Crowley JS, Sherwood J, Sullivan PS (2020) Assessing differential impacts of COVID-19 on black communities. Ann Epidemiol 47:37–44. https://doi.org/10.1016/j.annepidem.2020.05.003
Ministerio de Sanidad, Consumo y Bienestar Social—Profesionales—Datos abiertos de capacidad asistencial. (s. f.). Recuperado 6 de julio de 2021, de https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/nCov/capacidadAsistencial.htm.
Ocana-Riola R, Sanchez-Cantalejo C (2005) Rurality Index for Small Areas in Spain. Soc Indic Res 73(2):247
Ogen Y (2020) Assessing nitrogen dioxide (NO2) levels as a contributing factor to coronavirus (COVID-19) fatality. Sci Total Environ 726:138605. https://doi.org/10.1016/j.scitotenv.2020.138605
Olulana, O. (n.d.) (s. f.). Racial, Economic and Health Inequality and COVID-19 Infection in the United States. 21
Park J, Son W, Ryu Y, Choi SB, Kwon O, Ahn I (2020) Effects of temperature, humidity, and diurnal temperature range on influenza incidence in a temperate region. Influenza Other Respir Viruses 14(1):11–18. https://doi.org/10.1111/irv.12682
Perone G (2021) The determinants of COVID-19 case fatality rate (CFR) in the Italian regions and provinces: an analysis of environmental, demographic, and healthcare factors. Sci Total Environ 755:142523. https://doi.org/10.1016/j.scitotenv.2020.142523
Pollán M, Pérez-Gómez B, Pastor-Barriuso R, Oteo J, Hernán MA, Pérez-Olmeda M, Sanmartín JL, Fernández-García A, Cruz I, Larrea NF, Molina M, Rodríguez-Cabrera F, Martín M, Merino-Amador P, Paniagua JL, Muñoz-Montalvo JF, Blanco F, Yotti R, Blanco F et al (2020) Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study. The Lancet 396(10250):535–544. https://doi.org/10.1016/S0140-6736(20)31483-5
Poole L (2020) Seasonal influences on the spread of SARS-CoV-2 (COVID19), causality, and forecastabililty (3-15-2020). SSRN Electr J https://doi.org/10.2139/ssrn.3554746
Qi H, Xiao S, Shi R, Ward MP, Chen Y, Tu W, Su Q, Wang W, Wang X, Zhang Z (2020) COVID-19 transmission in Mainland China is associated with temperature and humidity: a time-series analysis. Sci Total Environ 728:138778. https://doi.org/10.1016/j.scitotenv.2020.138778
Qian H, Miao T, Liu L, Zheng X, Luo D, Li Y (2021) Indoor transmission of SARS-CoV-2. Indoor Air 31(3):639–645. https://doi.org/10.1111/ina.12766
Querol X (2012). Bases científico-técnicas para un Plan Nacional de Mejora de la Calidad del Aire. Consejo Superior de Investigaciones Científicas.
Querol X, Massagué J, Alastuey A, Moreno T, Gangoiti G, Mantilla E, Duéguez JJ, Escudero M, Monfort E, Pérez García-Pando C, Petetin H, Jorba O, Vázquez V, de la Rosa J, Campos A, Muñóz M, Monge S, Hervás M, Javato R, Cornide MJ (2021) Lessons from the COVID-19 air pollution decrease in Spain: Now what? Sci Total Environ 779:146380. https://doi.org/10.1016/j.scitotenv.2021.146380
Rahimi NR, Fouladi-Fard R, Aali R, Conti Gea O, Fiore M (2021) Bidirectional association between COVID-19 and the environment: A systematic review. Environ Res, 194,110692.
Red de aeropuertos—Aena.es. (s. f.). (2021) Recuperado 15 de junio de 2021, de https://portal.aena.es/es/aerolineas/red-aeropuertos.html.
Rosario Denes KA, Mutz Yhan S, Bernardes Patricia C, Conte-Junior Carlos A (2020) Relationship between COVID-19 and weather: case study in a tropical country. Int J Hyg Environ Health 229:113587
Saez M, Tobias A, Barceló MA (2020) Effects of long-term exposure to air pollutants on the spatial spread of COVID-19 in Catalonia. Spain. Environ Res 191:110177. https://doi.org/10.1016/j.envres.2020.110177
Şahin M (2020) Impact of weather on COVID-19 pandemic in Turkey. Sci Total Environ 728:138810. https://doi.org/10.1016/j.scitotenv.2020.138810
Sangkham S, Thongtip S, Vongruang P (2021) Influence of air pollution and meteorological factors on the spread of COVID-19 in the Bangkok Metropolitan Region and air quality during the outbreak. Environ Res 197:111104. https://doi.org/10.1016/j.envres.2021.111104
Sarkodie SA, Owusu PA (2020) Impact of meteorological factors on COVID-19 pandemic: evidence from top 20 countries with confirmed cases. Environ Res 191:110101. https://doi.org/10.1016/j.envres.2020.110101
Setti L, Passarini F, De Gennaro G, Barbieri P, Licen S, Perrone MG, Piazzalunga A, Borelli M, Palmisani J, Di Gilio A, Rizzo E, Colao A, Piscitelli P, Miani A (2020) Potential role of particulate matter in the spreading of COVID-19 in Northern Italy: first observational study based on initial epidemic diffusion. BMJ Open 10(9):e039338. https://doi.org/10.1136/bmjopen-2020-039338
SGFAL. (s. f.). CONPREL: Consulta Presupuestos y Liquidaciones de EELL. Recuperado 6 de julio de 2021, de https://serviciostelematicosext.hacienda.gob.es/SGFAL/CONPREL.
Shahzad F, Shahzad U, Fareed Z, Iqbal N, Hashmi SH, Ahmad F (2020) Asymmetric nexus between temperature and COVID-19 in the top ten affected provinces of China: A current application of quantile-on-quantile approach. Sci Total Environ 736:139115. https://doi.org/10.1016/j.scitotenv.2020.139115
Shen L, Zhao T, Wang H, Zhu Y, Shu Z (2021) Importance of meteorology in air pollution events during the city lockdown for COVID-19 in Hubei Province, Central China. Sci Total Environ 754:142227
Srivastava A (2021) COVID-19 and air pollution and meteorology-an intricate relationship: A review. Chemosphere 263:128297. https://doi.org/10.1016/j.chemosphere.2020.128297
Tablas estadísticas 2019. (s. f.). Recuperado 15 de junio de 2021, de https://www.dgt.es/es/seguridad-vial/estadisticas-e-indicadores/parque-vehiculos/tablas-estadisticas/2019/.
Tang, X., Wu, C., Li, X., Song, Y., Yao, X., Wu, X., Duan, Y., Lu, J. (2020). On the origin and continuing evolution of SARS-CoV-2 .Nat Sci 2020
Tello-Leal E, Macías-Hernández BA (2021) Association of environmental and meteorological factors on the spread of COVID-19 in Victoria, Mexico, and air quality during the lockdown. Environ Res 196:110442. https://doi.org/10.1016/j.envres.2020.110442
Tosepu R, Gunawan J, Effendy DS, Ahmad LOAI, Lestari H, Bahar H, Asfian P (2020) Correlation between weather and Covid-19 pandemic in Jakarta. Indonesia. Sci Total Environ 725:138436. https://doi.org/10.1016/j.scitotenv.2020.138436
Travaglio M, Yu Y, Popovic R, Selley L, Leal NS, Martins LM (2021) Links between air pollution and COVID-19 in England. Environ Pollut 268:115859. https://doi.org/10.1016/j.envpol.2020.115859
Villanueva F, Notario A, Cabañas B, Salgado S, Gabriel MF (2021) Assessment of CO2 and aerosol (PM2.5, PM10, UFP) concentrations during the reopening of schools in the COVID-19 pandemic: The case of a metropolitan area in Central-Southern Spain. Environ Res 197(111092)
Wang CC, Prather KA, Sznitman J, Jimenez JL, Lakdawala SS, Tufekci Z, Marr LC (2021) Airborne transmission of respiratory viruses. Science 373(6558). https://doi.org/10.1126/science.abd9149
WHO-convened global study of origins of SARS-CoV-2: China Part. (s. f.). Recuperado 17 de junio de 2021, de https://www.who.int/publications-detail-redirect/who-convened-global-study-of-origins-of-sars-cov-2-china-part.
Wu Y, Jing W, Liu J, Ma Q, Yuan J, Wang Y, Du M, Liu M (2020) Effects of temperature and humidity on the daily new cases and new deaths of COVID-19 in 166 countries. Sci Total Environ 729:139051. https://doi.org/10.1016/j.scitotenv.2020.139051
Xie J, Zhu Y (2020) Association between ambient temperature and COVID-19 infection in 122 cities from China. Sci Total Environ 724:138201. https://doi.org/10.1016/j.scitotenv.2020.138201
Xu K, Cui K, Young L-H, Hsieh Y-K, Wang Y-F, Zhang J et al (2020) Impact of the COVID-19 event on air quality in central China. Aerosol Air Qual Res 20:915–929
Yan R, Zhang Y, Li Y, Xia L, Guo Y, Zhou Q (2020) Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science 367(6485):1444–1448. https://doi.org/10.1126/science.abb2762
You H, Wu X, Guo X (2020) Distribution of COVID-19 Morbidity rate in association with social and economic factors in Wuhan, China: implications for urban development. Int J Environ Res Publ Health 17(10):3417. https://doi.org/10.3390/ijerph17103417
Yuan J, Wu Y, Jing W, Liu J, Du M, Wang Y, Liu M (2021) Non-linear correlation between daily new cases of COVID-19 and meteorological factors in 127 countries. Environ Res 193:110521. https://doi.org/10.1016/j.envres.2020.110521
Zhu Y, Xie J, Huang F, Cao L (2020) Association between short-term exposure to air pollution and COVID-19 infection: Evidence from China. Sci Total Environ 727:138704. https://doi.org/10.1016/j.scitotenv.2020.138704
Zoran MA, Savastru RS, Savastru DM, Tautan MN (2020) Assessing the relationship between surface levels of PM2.5 and PM10 particulate matter impact on COVID-19 in Milan, Italy. Sci Total Environ 738:139825. https://doi.org/10.1016/j.scitotenv.2020.139825
Acknowledgements
To Maria Ascaso Sánchez for collaboration in writing this article.
Funding
This work was carried out with funds of the ENPY 221/20 project.
Author information
Authors and Affiliations
Contributions
Conceptualization: Julio Diaz; Cristina Linares. Methodology: Julio Diaz; Cristina Linares; Software: José A. Lopez. Supervision: Julio Diaz, Cristina Linares. Data curation: Dante R. Culqui; Alex Blanco. Writing—original draft preparation: Dante R. Culqui; Alex Blanco. Writing—reviewing and Editing: Dante R. Culqui; Alex Blanco. Visualization: José A. Lopez; Miguel A. Navas; Gerado Sanchez-Martinez; Yolanda Luna; Beatriz Hervella; Fernando Belda. Investigation: José A. Lopez; Miguel A. Navas; Gerado Sanchez-Martinez; Yolanda Luna; Beatriz Hervella; Fernando Belda. Software: José A. Lopez; Miguel A. Navas. Validation: José A. Lopez; Miguel A. Navas.
Corresponding author
Ethics declarations
Ethics approval
This study do not need to approbation by ethical committee because in this study we worked with aggregate data and we aren't including personal information.
The manuscript was not submitted to more than one journal for simultaneous consideration. The submitted work is original and have been not published elsewhere in any form or language (partially or in full).
Consent to participate
This study works with aggregate data; therefore, there are no individual data, and the consent to participate is not applicable.
Consent for publication
This study works with aggregate data, and there are no individual data; therefore, the consent to publish is not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The original online version of this article was revised: The correct given name of the 3rd Author is Alejandro.
Rights and permissions
About this article

Cite this article
Culqui, D.R., Díaz, J., Blanco, A. et al. Short-term influence of environmental factors and social variables COVID-19 disease in Spain during first wave (Feb–May 2020). Environ Sci Pollut Res 29, 50392–50406 (2022). https://doi.org/10.1007/s11356-022-19232-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-022-19232-9