
Abstract
Background
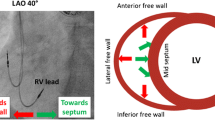
The fluoroscopic individualized LAO (i-LAO) projection has demonstrated high accuracy for identifying right ventricular (RV) lead positioning, likely by approximating a view along the septal or RV long axes. However, RV and septal anatomical axes have not been studied, and their relation with i-LAO is unknown. We sought to determine RV, septal, and left ventricular (LV) long-axis orientations by CT scan and to compare them to the i-LAO angle, to confirm the anatomical relevance of i-LAO.
Methods
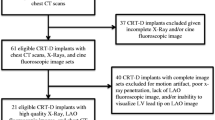
We prospectively included patients (pts) for whom i-LAO angle was determined during pacemaker or defibrillator implant. Then, RV, septal, and LV long-axis orientations were determined by CT scan by a physician blinded to i-LAO data. The horizontal components of the cardiac axes were compared with those of the i-LAO angle.
Results
We included 26 pts. Median values were 57.5° for i-LAO angle (range 47.5–70), 64.5° for RV axis (range 48–90), 51.5° for septal axis (range 39–74), and 37° for LV axis (range 25–67). i-LAO angle best correlated with septal axis (r = 0.91 and ρc = 0.71). Up to an angle of 70° (maximal measurable i-LAO value; 23/26 pts), the i-LAO angle was comprised between the septal and the RV axes (21/23 pts, 91.3%), or within 2° of this interval (2/23 pts, 8.7%).
Conclusions
RV and septal anatomical axes present major interindividual variations, prompting the use of individualized fluoroscopy criteria for lead implantation. i-LAO angle demonstrated to be almost constantly between the septal and RV long axes, thus confirming its anatomical relevance for RV lead implantation.






Similar content being viewed by others

References
Shimony A, Eisenberg MJ, Filion KB, Amit G. Beneficial effects of right ventricular non-apical vs. apical pacing: a systematic review and meta-analysis of randomized-controlled trials. Europace. 2012;14:81–91.
Margulescu AD, Suran BM, Rimbas RC, Dulgheru RE, Siliste C, Vinereanu D. Accuracy of fluoroscopic and electrocardiographic criteria for pacemaker lead implantation by comparison with three-dimensional echocardiography. J Am Soc Echocardiogr. 2012;25:796–803.
Pang BJ, Joshi SB, Lui EH, Tacey MA, Ling LH, Alison J, et al. Validation of conventional fluoroscopic and ECG criteria for right ventricular pacemaker lead position using cardiac computed tomography. Pacing Clin Electrophysiol. 2014;37:495–504.
Sharma G, Salahuddin S, Sanders P, Gupta H, Gulati G, Jagia P, et al. Inadequacy of fluoroscopy and electrocardiogram in predicting septal position in RVOT pacing - validation with cardiac computed tomography. Indian Heart J. 2016;68:174–80.
Squara F, Scarlatti D, Riccini P, Garret G, Moceri P, Ferrari E. Classical fluoroscopy criteria poorly predict right ventricular lead septal positioning by comparison with echocardiography. J Interv Card Electrophysiol. 2018;52:209–15.
Engblom H, Hedstrom E, Palmer J, Wagner GS, Arheden H. Determination of the left ventricular long-axis orientation from a single short-axis MR image: relation to BMI and age. Clin Physiol Funct Imaging. 2004;24:310–5.
Engblom H, Foster JE, Martin TN, Groenning B, Pahlm O, Dargie HJ, et al. The relationship between electrical axis by 12-lead electrocardiogram and anatomical axis of the heart by cardiac magnetic resonance in healthy subjects. Am Heart J. 2005;150:507–12.
Foster JE, Engblom H, Martin TN, Wagner GS, Steedman T, Ferrua S, et al. Determination of left ventricular long-axis orientation using MRI: changes during the respiratory and cardiac cycles in normal and diseased subjects. Clin Physiol Funct Imaging. 2005;25:286–92.
Sathananthan G, Aggarwal G, Zahid S, Byth K, Chik W, Friedman D, et al. Computed tomography-guided in vivo cardiac orientation and correlation with ecg in individuals without structural heart disease and in age-matched obese and older individuals. Clin Anat (New York, NY). 2015;28:487–93.
Squara F, Scarlatti D, Riccini P, Garret G, Moceri P, Ferrari E. Individualized left anterior oblique projection: a highly reliable patient-tailored fluoroscopy criterion for right ventricular lead positioning. Circ Arrhythm Electrophysiol. 2018;11:e006107.
Squara F, Tomi J, Scarlatti D, Theodore G, Moceri P, Ferrari E. Self-taught axillary vein access without venography for pacemaker implantation: prospective randomized comparison with the cephalic vein access. Europace. 2017.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures followed our institutional guidelines, and all patients provided their written informed consent.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Squara, F., Fourrier, E., Diascorn, Y. et al. Cardiac anatomical axes by CT scan and confirmation of the accuracy of fluoroscopic individualized left anterior oblique projection for right ventricular lead implantation. J Interv Card Electrophysiol 60, 213–219 (2021). https://doi.org/10.1007/s10840-020-00729-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10840-020-00729-7