
Abstract
Background
Studies assessing the effects of parenting programs have focused on interventions delivered through face-to-face modalities. There is a need for research to evaluate the effects of online parenting programs on child development, such as the BEM Program (‘Play Teaches Change’ in English), an online play-based parenting program that teaches caregivers on how to introduce playful interactions into their daily household chores.
Objective
To assess the effects of the BEM Program on child development and the quality of caregiver-child interaction.
Method
A two-arm randomized controlled trial was conducted in a socioeconomically disadvantaged district of São Paulo city in Brazil. 129 children aged 12–23 months and their caregiver were randomly assigned to receive either the BEM Program for 8 weeks (intervention, n = 66) or standard child care (control, n = 63). Data were collected at baseline and endline of the intervention through home visits and online interviews. An intention-to-treat analysis was conducted.
Results
The intervention showed positive effects on child development, by improving language development (Cohen’s d = 0.20, 95%CI 0.08–0.47) and reduced intrusiveness (Cohen’s d = 0.35, 95%CI 0.06–0.65) of caregiver-child interaction. No significant differences were observed in caregiver’s repertoire and engagement in age-appropriate play activities with the child while doing the household chores, parenting sense of competence and perceived stress.
Conclusions
Despite the small size and low adherence to the program, such promising results advance evidences for fully remote parenting programs and their effects on child development.
Similar content being viewed by others


Introduction
Globally, a significant number of children under the age of 5 years in low-middle income countries (LMICs) live in conditions that hinder their fundamental right to healthy development (Lu et al., 2016). This reality represents a major public health concern and improving these children’s lives is currently a global priority. Poverty is a critical factor which determines the quality of the environment and the presence of other negative conditions that put children at risk of not achieving their developmental potential (Grantham-McGregor et al., 2007). Early experiences in life shape the quality of brain architecture which is crucial for child’s development and lifelong physical and mental health, school performance and income (Fox et al., 2010; Heckman, 2006).
Research demonstrates that a stimulating and nurturing home environment in early childhood might protect children from the negative effects of poverty and toxic stress on early child development (Bick & Nelson, 2017; Shonkoff, 2012; Shonkoff & Phillips, 2000). Caregivers living under poor conditions may experience greater financial and emotional difficulties in fulfilling their parenting role (Britto et al., 2017; Harris et al., 2020). Thus, these caregivers often require support to create stimulating and nurturing environments to promote child development (Britto & Ulkuer, 2012; Rayce et al., 2017).
Parenting programs are interventions or services that aim to improve parenting interactions, behaviors, practices, knowledge, attitudes and beliefs regarding child care to promote better child health and development (Britto et al., 2017). These programs are the most suitable strategy to reach both caregivers and children in order to enhance child development and health through early learning and responsive interactions (Jeong et al., 2021). Consequently, researchers and policy makers have increased their interest in investing in parenting interventions to promote early child development. Meta-analyses and systematic reviews have confirmed the effectiveness of parenting programs on improving caregiver-child interaction and child development (Britto et al., 2017; Jeong et al., 2018; Rayce et al., 2017). Specifically, previous studies revealed a positive effect of short duration (approximately 8–12 weeks) parenting programs on child development outcomes (Kochanska et al., 2013; McGillion et al., 2017; Murray et al., 2016; Pontoppidan et al., 2016; Vally et al., 2015).
Nonetheless, studies on the effectiveness of parenting programs focusing on caregiver-child interaction and child development have mainly been delivered through face-to-face modalities such as home visits, parent group meetings or interventions during well-child visits. Hence, most of the available evidence on parenting programs is based on these delivery modalities, and evidence-based online parenting programs are scarce in LMIC (Jeong et al., 2021), where the majority of children are at risk of not meeting their cognitive and socioemotional potential (McCoy et al., 2016).
Online Parenting Programs
Parenting programs are a promising strategy to guide and motivate caregivers and promote the acquisition of parenting skills that enhance the healthy development of the children and prevent future problems (Pontoppidan et al., 2016, WHO, 1997). While various types of interventions, including nutrition and health, can support healthy development, evidence has revealed that those parenting programs that include components to directly improve caregiver-child interaction are more effective in improving early child development outcomes (Engle et al., 2007).
Traditional delivery modalities of parenting programs that require a face-to-face meeting either at home or at the health center present challenges in reaching a large number of families due to the logistical, economical and human requirements (Breitenstein et al., 2014; Shah et al., 2016). Reaching socioeconomically disadvantaged populations in Brazil could represent another challenge. Parents, and specially mothers, face important time constraints for participating in face-to-face interventions due to their work, household chores, child care and the territorial extension of the country.
Therefore, remote interventions such as online interventions represent an innovative option that reduces the challenges of face-to-face activities and reaches a greater number of children and their families. Previous systematic reviews and meta-analyses revealed that online parenting interventions targeting children in the age range of 0–5 years were effective to improve caregivers and child outcomes (Breitenstein et al., 2014; Harris et al., 2020; Nieuwboer et al., 2013). Nonetheless, a recent systematic review showed a limited number of studies that assess the effect of remotely delivery parenting programs on caregiver-child interaction and child development (Solís-Cordero et al., 2022). Thus, it is imperative to develop and test remotely delivered interventions that focus on children living under adverse conditions to ensure positive child outcomes.
The BEM Program (an acronym for Brincar Ensina a Mudar in Portuguese, which in English is Play Teaches Change) is an online play-based parenting program that teaches female caregivers, living in socioeconomically disadvantaged areas of São Paulo city and responsible for the care of children from 12 to 23 months of age, how to introduce playful interactions into their daily household chores to enhance the quality of caregiver-child interaction and child development.
Play as a Strategy to Improve the Quality of Caregiver-Child Interaction and Child Development
Previous studies have shown that encouraging play between caregiver and child provided an ideal opportunity to strengthen caregiver-child interactions and improve child development (Abimpaye et al., 2019; Attanasio et al., 2014; Shah et al., 2019; Yousafzai et al., 2016). However, caregivers are often not aware of the need for play materials, playmates, and responsive interaction (Aboud et al., 2013). Children living under poverty and disadvantaged socioeconomic backgrounds are more likely to experience less playful and stimulating interactions with their caregivers (Grantham-McGregor et al., 2007).
In Brazil, specifically, a study titled: “Playing in Brazilian Slums” revealed that: 50% of caregivers had difficulty finding time to play with children, 68% had difficulty taking care of the house and children at the same time, 88% of mothers turn to screens to distract their children and take care of household chores. For 63% of children, the main place to play is indoors, only 29% of mothers have a playground in the community (Unidos pelo brincar, 2021). Moreover, a study entitled: “Perceptions and Practices of Society in Relation to Early Childhood” showed that only 19% of the participants recognized play as one of the important aspects for the development of children under 3 years of age (Fundação Maria Cecilia Souto Vidigal, 2013).
Caregivers can take advantage of different times of the day to incorporate playful activities that promote caregiver-child interactions and child development. Playful moments are everywhere, and even daily chores alongside parents can be turned into playful opportunities (Galinsky, 2010; Yogman et al, 2018). The novelty of the BEM Program comes from this idea of taking advantage of everyday simple moments and household items to play with children to improve the quality of caregiver-child interaction and child development.
Therefore, in addition to being online, another core element that makes the BEM Program stand out as an innovative intervention is the incorporation of playful activities between the caregiver and their children in the daily routine. Many other parenting programs might require caregivers to allocate exclusive time to play with their children. The BEM Program represents a valuable option for female caregivers, who find it difficult to separate time to play with their children or who do not know how to take advantage of the little time they have available with their children. Since this program teaches caregivers about the importance of engaging in playful activities with their children, what kind of activities they can incorporate into their daily routine and how to incorporate these activities with their children into their daily household chores.
Current Study
The aim of this study was to assess the effect of the BEM Program on child development (primary outcome), quality of caregiver-child interaction, caregiver’s repertoire and engagement in age-appropriate play activities with the child while doing household chores, parenting sense of competence and perceived stress (secondary outcomes). We further examined whether adherence to the program, caregiver’s education level and number of children at home moderated the effect of the intervention on primary and secondary outcomes. We hypothesized that, compared to the control group, children from families who received the BEM Program would have fewer developmental delays and caregivers would engage more in age-appropriate play activities with the child during the daily routine. We also hypothesized that caregiver-child dyads who received the BEM Program would have higher quality caregiver-child interactions and sense of parental competence and would experience less stress than dyads from the control group. Finally, we hypothesized that the effect of the intervention would be larger among caregivers who participated more in the program, had a higher educational level, and had fewer number of children at home.
Methods
Study Design and Setting
We performed a two-arm randomized controlled trial to assess the effects of the BEM Program on child development and the quality of caregiver-child interaction, and other secondary outcomes. The intervention group received the BEM Program and the control group received the standard care. Dyads participating in the study who received standard care did not receive any type of intervention other than the care received in the daycare.
We adhered to the Consolidated Standards of Reporting Trials (CONSORT) guidelines for reporting our study.
This randomized controlled trial was conducted between July 2019 and August 2020 in Campo Limpo, a socioeconomically disadvantaged district of São Paulo city in Brazil. This district is located 20 km from the city center, and has one of the highest prevalence of households in slums (highly populated urban residential area where living conditions are poor) (26.6%) (Rede Nossa São Paulo, 2019).
Participants and Sample Size
The study recruited 129 children aged 11–21 months and their female caregivers. Female caregiver was defined as the female adult who lived with the child, who had the responsibility of caring, stimulating, loving and educating the child, and with whom the child has formed the strongest emotional bonds in the first year of life (Fundação Maria Cecilia Souto Vidagal, 2017). Therefore, the female caregiver was not necessarily the child’s mother; rather, sometimes it was the grandmother.
The sample size was calculated based on the global development indicator (Denver II) (Frankenburg, 1992). Considering a power of 80%, alpha of 5%, R2 of covariates (Denver at baseline, sex, age, race) of 56% (based on Phase I results), the sample size was 160 families per group.
Inclusion criteria were children aged between 11 and 21 months at enrollment, who lived in Campo Limpo, who attended daycare centers where the BEM Program was implemented, and had a female caregiver who had a smartphone with Internet access.
Children with clinical conditions that interfered with the typical course of development, twins and caregivers who did not understand Portuguese were excluded.
In order to achieve the required sample size, the study was conducted in two cohorts. Recruitment took place at two timepoints, in July 2019 and January 2020. Caregiver-child dyads were recruited at 14 daycare centers located in the district where the study was conducted, and that accepted to participate in the research. All female caregivers of children aged between 11 and 21 months at the time of recruitment were invited to participate during a face-to-face meeting at each daycare center. Recruitment materials were also sent home with the children and delivered to parents via mobile messaging. Once the caregiver showed interest in participating in the research, data was collected to confirm the inclusion criteria, and her consent was obtained for participation in the study.
Intervention
The BEM Program is an eight-week online play-based parenting program which aims to improve caregiver-child interaction for enhancing the development of children aged 12 to 23 months from socially disadvantaged families. The BEM Program is an innovative parenting program which consists of 8 video classes and 40 text and audio messages sent through WhatsApp, which teaches female caregivers how to play with their children during the daily routine, using resources available at home.
The theoretical framework in which we based our intervention is the Nurturing Care for Early Childhood Development Framework of the World Health Organization. This framework presents five core components of nurturing care for children reaching their developmental potential: good health, adequate nutrition, opportunities for early learning, security and safety and responsive caregiving (WHO, 2018). The Nurturing Care encourages the creation and implementation of interventions that provide opportunities for early learning and support responsive caregiving, two components of nurturing care that can be supported by caregiver-child playful interactions. In terms of opportunities for early learning, evidence shows that young children under 3 years old learn and explore the world through playing (Ginsburg et al., 2007; Kochanska et al, 2013; Yogman et al., 2018) Playful interactions between caregiver and children during everyday activities, such as cooking, cleaning, feeding, bathing and sleeping, with the use of materials and household objects that are commonly available at home represent great opportunities for early learning (Popp & Thomsen, 2017; Yogman et al., 2018). Regarding the component of responsive caregiving, caregivers are children’s first playmates and the home environment is where the children’s first experiences with play occur (Brazelton & Greenspan, 2002) The framework recognizes the importance of responsive interactions to stimulate brain connections and enhance caregiver-child interactions. Through playing, caregivers observe and learn to respond to children’s movements, sounds, gestures and verbal requests which contributes to build an emotional bond and secure attachment (WHO, 2018). Thus, the creation and implementation of the BEM Program encourages opportunities for early learning and supporting responsive caregiving through playful interactions during daily activities with the use of materials and household objects commonly available at home.
The content of the BEM Program is adapted to the children's age group (12–23 months), focused on four prominent and frequent household chores of the caregiver’s daily routine: (1) while she cooks or washes the dishes, (2) while she washes clothes, (3) while she cleans the house, and (4) while she takes care of the child. Each of the videos presented a playful activity that could be included into a specific moment of the caregiver’s routine. In addition to explaining how to do the activity, the video included information such as safety tips and benefits for caregiver-child interaction and child development. Text and audio messages complement the content of the video lessons by providing additional information on child development, responsive parenting, strengthening the bond with children and taking advantage of moments of interaction to promote early learning experiences. Video, text and audio messages were selected from previous studies of proof of concept and feasibility.
The BEM Program was delivered on two separate occasions. The first cohort received the program between October and November 2019; and the second between April and May 2020, during COVID-19 pandemic.
Outcomes
Primary outcome: Child development was assessed using the Ages and Stages-3, Brazilian version, a caregiver completed scale that assesses child development through five domains: communication, gross motor coordination, fine motor coordination, problem-solving and personal-social skills (Filgueiras et al., 2013). For each domain, the child can get a score between 0 and 60. The higher the score, the better the child development.
Secondary outcomes: Quality of caregiver-child interaction was assessed through the Coding Interactive Behavior (CIB), a tool for coding parent-infant interactions using a set of observable behaviors (Feldman, 1998). The CIB consists of 43 scales; 22 are adult scales, 16 are child scales, and 5 are dyadic scales. A 5-min video of an interaction between the caregiver and the child while playing was coded on a 5-point scale, where 1 implies a minimal level of the specific behavior or attitude and 5 implies a maximal level (Feldman, 1998). Coding was conducted by trained coders, blind to any other information. To analyze the quality of interaction, eight composites were created by grouping different scales, according to the indications of the CIB instrument.
Repertoire and engagement in age-appropriate play activities with the child while doing the household chores was assessed. Due to the non-existence of an instrument that would allow to asses play with the child while doing household chores, a questionnaire was created and pre-tested by the researchers. Through yes/no questions we verified whether the caregiver played with the child while doing household chores (at the four specific moments addressed in the intervention: while she cooks or washes the dishes, while she washes clothes, while she cleans the house, and while she takes care of the child) and if it was considered possible to incorporate playing while doing the household chores. In addition, from a list of options of household chores and playful activities, the participants could choose which playful activities they engaged in while doing each of the household chores in their routine. Then, we calculated a score of the total number of activities according to each of the household chores. Finally, engagement in age-appropriate play activities with the child while doing the household chores was evaluated by analyzing one 5-min video, using another instrument created by the research team for this purpose. The instrument consisted of a checklist that identifies whether the caregiver engaged with the child in playful activities while doing household chores (at the four specific moments addressed in the intervention). Two trained examiners assessed the videos. Prior to coding, examiners were trained and reliability was established at r > 0.8 for both examiners. More details of both instruments are reported elsewhere.
Parenting sense of competence was evaluated through the Parenting Sense of Competence Scale (PSOC), which consists of 17-item scale answered on a 6-points scale ranging from “strongly disagree” to “strongly agree”. The PSOC measures parents’ satisfaction with parenting and their self-efficacy in the parenting role. A higher score indicates a greater sense of parenting competence. Studies have reported an internal consistency of the PSOC Scales Scores of 0.80. (Ohan et al., 2000). We used the Portuguese translation authorized by the authors (Linhares & Gaspardo, 2017).
Perceived stress was measured using the Perceived Stress Scale, a 14-item instrument designed to determine the degree to which life situations are considered as stressful during the last month. A higher level of stress is indicated by higher scores on this scale (Cohen et al., 1983). The internal consistency of the Brazilian version was 0.82. (Luft et al., 2007).
Measurements
Child’s sex, age, prematurity and skin color, caregiver’s age, education, work, marital status and skin color; and family’s income, number of children and beneficiary of Bolsa Familia (Brazilian cash-transfer Program) were collected using a sociodemographic questionnaire.
Caregiver’s adherence to the program was calculated by the number of videos watched and class time watched per caregiver (%per caregiver), data that were obtained through the Wistia Platform database (online video platform that registered the access to the videos and watched time). Using this data, we classified adherence into (1) adhered caregivers who watched 4 or more video classes, and (2) non-adhered caregivers who watched fewer than 4 classes.
Data Collection
Data were collected at baseline and endline of the intervention by 10 trained data collectors. Both baseline and endline data collection for cohort 1, and baseline data collection for cohort 2 was performed during home visits. Due to the COVID-19 pandemic and the stay-at-home measures it was no longer feasible to do the home visits for endline data collection of cohort 2. Data collection procedure modifications due to the COVID-pandemic have been published elsewhere (Solís-Cordero et al., 2021). Briefly, visits were adapted to an online video-conference to collect the endline data for cohort 2 only. The participants were interviewed by the data collectors through a video-conference using WhatsApp or Zoom.
Data collectors used the REDCap platform (Research Electronic Data Capture) directly on tablets. This software allows the collection of data offline and the direct transmission of responses to a database, which avoids wasting time and minimizes typing errors (RedCap, 2018). Tablets were also used for recording the two 5-min videos used to assess two of our outcomes (caregiver-child interaction and repertoire and engagement in age-appropriate play activities with the child).
Randomization and Blinding
Eligible caregiver-child dyads were randomized to the intervention or control group after the collection of baseline data. Randomization was at the family level; families were stratified based on child daycare center and Denver scores at baseline (global, language, adaptative and gross motor); within each stratum, half of the families were randomly selected to the intervention and half to the control group. Random assignment was done by a researcher who had no role in the direct implementation of the intervention.
Due to the characteristics of the intervention, blinding of participants was not possible. However, the examiners who assessed the trial outcomes were blinded to group allocation.
Statistical Analyses
Descriptive statistics were computed for the entire study sample by randomized group. Numerical data were described with location (mean) and dispersion (standard deviation) measures, whereas categorical variables were described as absolute and relative frequencies. Group comparisons of transversal variables were carried out with Student or Welch t-test and Wilcoxon-Mann–Whitney test for continuous variables and chi-squared test for categorical ones. A longitudinal comparison of intervention groups was done using linear mixed models (LMM) or its generalized version (GLMM) on all available data; the distribution used for the latter is noted in the table. The model incorporated time (baseline and endline), randomized group (control vs intervention) and group by time interaction. Intervention effects were estimated for this model as the difference between the intervention and control arms in mean change from baseline to endline. Model 1 was the intent-to treat. Model 2 adjusted for characteristics which were not comparable across intervention and control groups at baseline. All models were adjusted for stratification variables used in randomization. The residual normality assumption was assessed by inspecting the corresponding QQ plot and homoscedasticity with Levene test. All analyses were conducted in R 4.2.1. Subgroup analyses were conducted to examine whether intervention effects differed by (1) adherence to the program (categorized as caregiver having watched ≥ or < 4 intervention videos), (2) caregiver educational level and (3) number of children at home. Cohen’s d effect sizes were calculated.
Ethics
The study received approval from the Fundação José Luiz Egydio Setubal Institutional Review Board (IRB File # 09,941,319.1.0000.5567). All caregivers provided written informed consent (or thumbprint) at the time of the baseline data collection. The corresponding author takes responsibility for the integrity of the data and the accuracy of the data analysis.
Results
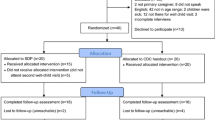
Sociodemographic variables and adherence to the intervention were similar for the two cohorts and therefore, participants for both cohorts were combined in a pooled analysis. Of the 496 caregiver–child dyads assessed for eligibility, 129 were enrolled in the study for the baseline data collection, and 66 were allocated to the intervention group and 63 to the control group (Fig. 1).

CONSORT diagram for the randomized controlled trial
Loss to follow-up was 31%. Families lost to follow up were more likely to receive Bolsa Familia (32.5%, p = 0.013) and had more children (2.1 children on average, p = 0.047).
Table 1 shows the characteristics of the study population at baseline. Only caregiver’s race was significantly different between intervention and control group at baseline (p = 0.019).
The BEM Program significantly improved the communication domain of child development compared to the control group (p < 0.001) (Table 2), Cohen’s d effect size was 0.20 (95%CI 0.08–0.47). No significant differences were observed in the other developmental domains (Fig. 2), although descriptively they have tended to be better in the endline of the intervention group compared to the control group.

BEM Program Effect on Child Development (Primary Outcome)
Quality of caregiver-child interaction outcomes are reported in Table 3. We found positive effects of the BEM Program on the component intrusiveness of the quality of caregiver-child interaction (p = 0.015), Cohen’s d effect size was 0.35 (95%CI 0.06–0.65).
Finally, there was no effect of the BEM Program on the repertoire and engagement in age-appropriate play activities with the child while doing the household chores (Table 4). Parenting sense of competence and perceived stress, both outcomes assessed at the caregiver level, were not affected by the intervention.
We found no differences in any of the outcomes when adjusting for caregiver’s race (Model 2). Moreover, we found no moderating effect of the caregiver’s education level, number of children at home and adherence of caregivers to the program on any primary and secondary outcomes.
Discussion
We conducted this study to examine the effects of an online play-based parenting program on child development (primary outcome), quality of caregiver-child interaction, caregiver’s repertoire and engagement in age-appropriate play activities with the child while doing the household chores, parenting sense of competence and perceived stress (secondary outcomes). Our findings show that the BEM Program had significant positive effects on the communication domain of child development, but not on other developmental domains, including cognitive, motor, socio-emotional development, and problem solving. Moreover, the program improved the quality of caregiver-child interaction, in terms of intrusiveness.
Previous parenting programs that promoted caregiver-child interactions and child development through responsive play found similar effects on early language development. A systematic review including 21 studies which assessed stimulation interventions based on responsive play with children aged 24 months and younger, demonstrated a medium effect size (0.47) on language (Aboud & Yousafzai, 2015). Additionally, a study carried out in Brazil with low-income families which provided an intervention promoting interaction through reading to 566 parent–child dyads with children aged 2–4 years, showed significant impact of the intervention on child language (Weisleder et al., 2018). The positive effect of the BEM Program on the communication domain of child development might be explained by the fact that the content of the messages and videos constantly reinforced the importance of activities that stimulate the child's speech. Further, evidence has shown that adult–child play benefits widely children’s language development (Moreno, 2016).
Benefits on the components of the quality of caregiver-child interaction were also seen in previous responsive parenting interventions. In relation to intrusiveness, a randomized controlled trial conducted in South Africa with 449 pregnant women with adverse socioeconomic circumstances showed that the mothers, who received an intervention which encourages sensitive and responsive interactions with her child, were significantly less intrusive while interacting with their child at 6 months of age (Cooper et al., 2009). Furthermore, at-risk mothers in the United States who participated in a high-intensity comprehensive parenting intervention were less intrusive with their child at 16 months of age (Guttentag et al., 2014).
The prior studies have used face-to-face interventions; the most common modalities of delivery being home visits, group sessions, and clinic appointments. The BEM Program undertook a novel online delivery method, sending caregivers weekly videos and daily messages to promote responsive interactions which could be built into their regular household chores and activities. This study was the first step towards creating a scalable and effective remotely delivered program.
Remotely delivered programs have important advantages for the service provider and participants. In regard to the service provider, staff implementing the intervention do not need to travel to participants’ home, reducing costs of ineffective visits, and allowing the intervention to be delivered to a large number of families in a short amount of time (Sawyer et al., 2017). Remote program delivery also enables the continuity of the intervention even in situations for which face-to-face contact is challenging such as in large geographical areas and when movement is restricted such as during the COVID-19 pandemic. Considering these last two advantages remotely delivered programs such as the BEM Program might be easier to scale. For participants, remotely delivered interventions ensures access to information when it is convenient for the participant, without being restricted by scheduled home visits or appointments (Sawyer et al., 2017).
Despite these advantages of the remotely delivered parenting programs, our results revealed low adherence to the program. It is well-known that adherence is a frequent challenge faced by intervention programs with consequences on its effectiveness (Souza et al., 2006). In the case of our intervention, the low adherence rates might be due to the lack of relationship-building that often occurs with home visits or group sessions, which likely increases adherence (Burrell et al., 2018; Girvin et al., 2007). Furthermore, a systematic review revealed no evidence of improvements from interventions that did not include direct contact between participants and providers. In contrast, those interventions incorporating direct contact were significantly effective (Harris et al., 2020).
To overcome the challenge represented by the low adherence rates the BEM Program could, in the future, be integrated within an existing face-to-face intervention. This type of mixed-modality intervention is supported by a systematic review that demonstrated that programs using more than one modality had a greater impact on child development than those using only one modality (Britto et al., 2015).
The short duration and the low intensity of the BEM Program could have contributed to the lack of effects on cognitive, motor, socio-emotional development, and problem solving, as well as on the caregiver outcomes. Evidence shows that the shorter and less intense the intervention, the more likely it is to have a smaller effect (Engle et al., 2007). Studies suggested that the minimum duration of a parenting program should be 12 months if the goal is to observe positive results in cognitive and socioemotional development, as well as parental outcomes (Britto et al., 2015).
Sociodemographic characteristics were associated with the caregiver’s adherence to the program and retainment in the study. Higher level of caregiver education was associated with better adherence to the program, a finding that is consistent with previous research (Eisner & Meidert, 2011; Souza et al., 2006). Further, families who remained in the study were less likely to benefit from Bolsa Família, i.e., they had better social conditions. Similar findings were reported in a systematic review where families with the greatest needs and who would benefit most from the intervention dropped out (Barrett, 2010). Caregivers with fewer financial needs and higher level of education might be more likely to recognize the impact of early interventions on child development such as the BEM Program which motivates them to participate more in the program.
Moreover, families who remained in the study were more likely to have only one child. Pontoppidan et al. (2016) demonstrated that families with greater number of children dropped out. This situation can be understood considering that the caregivers with more children at home might be busier with less time available to participate in the program or they might believe that they have more experience to take better care of the child than women who take care of fewer children.
Strengths of our study design and implementation included the use of self-report and observational assessments to measure child development and caregiver’s engagement in age-appropriate play activities with the child while doing the household chores, and the successful adaptation of data collection to a 100% online interview. The study also had several limitations including small sample size and a high loss to follow-up. Finally, we cannot ignore the limitations due to the barriers imposed by technology to keep the participants engaged in the intervention, such as lack of devices and access to Internet, and that participants must have some level of digital literacy.
Future research to assess the effect of BEM Program should incorporate strategies to improve participants’ adherence to the program, such as a tutor to support the implementation of the program, or while integrating the BEM Program into an existing face-to-face early childhood service, such as the Family Health Strategy, which is largely disseminated in Brazil. In addition, further research should consider not only the videos as adherence, but the impact of the messages as well.
Conclusion
An online play-based parenting program promoting caregiver-child interaction and child development showed positive results on language development and the quality of caregiver-child interaction among socioeconomically disadvantaged families. Despite the small size and low adherence to the program, such promising results advance evidences for fully remote parenting programs and their effects on improving child development. Further evaluation is needed to test strategies to improve participants’ adherence to the program and demonstrate the effectiveness of program on a larger scale.
References
Abimpaye, M., Dusabe, C., Nzabonimpa, J., Ashford, R., & Pisani, L. (2019). Improving parenting practices and development for young children in Rwanda: Results from a randomized control trial. International Journal of Behavioral Development. https://doi.org/10.1177/0165025419861173
Aboud, F. E., Singla, D. R., Nahil, M. I., & Borisova, I. (2013). Effectiveness of a parenting program in Bangladesh to address early childhood health, growth and development. Social Science and Medicine, 97, 250–258. https://doi.org/10.1016/j.socscimed.2013.06.020
Aboud, F. E., & Yousafzai, A. K. (2015). Global health and development in early childhood. Annual Review of Psychology, 66, 433–457. https://doi.org/10.1146/annurev-psych-010814-015128
Attanasio, O. P., Bentham, J., Fernández, C., Grantham-McGregor, S., Douglas, C. M., & Rubio-Codina, M. (2014). Using the infrastructure of a conditional cash transfer program to deliver a scalable integrated early child development program in Colombia: Cluster randomized controlled trial. BMJ (Online). https://doi.org/10.1136/bmj.g5785
Barrett, H. (2010). The delivery of parent skills training programmes Meta-analytic studies and systematic reviews of what works best.Family and Parenting Institute.
Bick, J., & Nelson, C. (2017). Early experience and brain development Wiley interdisciplinary reviews. Cognitive Science, 8(1–2), e1387. https://doi.org/10.1002/wcs.1387
Brazelton, T. B., & Greenspan, S. I. (2002). As necessidades essenciais das crianças: O que toda criança precisa para crescer, aprender e se desenvolver. Trad. Cristina Monteiro. Porto Alegre: Artmed.
Breitenstein, S. M., Gross, D., & Christophersen, R. (2014). Digital delivery methods of parenting training interventions: A systematic review. Worldviews on Evidence-Based Nursing, 11(3), 168–176. https://doi.org/10.1111/wvn.12040
Britto, P. R., Lye, S. J., Proulx, K., Yousafzai, A. K., Matthews, S. G., Vaivada, T., Perez-Escamilla, R., Rao, N.,… Early Childhood Development Interventions Review Group, for the Lancet Early Childhood Development Series Steering Committee. (2017). Nurturing care: promoting early childhood development. Lancet, 389(10064), 91-102. doi: https://doi.org/10.1016/S0140-6736(16)31390-3
Britto, P. R., Ponguta, L. A., Reyes, C., & Karnati, R. (2015). A Systematic Review of Parenting Programmes for Young Children. Retrieved from https://www.unicef.org/earlychildhood/files/P_Shanker_final__Systematic_Review_of_Parenting_ECD_Dec_15_copy.pdf
Britto, P. R., & Ulkuer, N. (2012). Child development in developing countries: Child rights and policy implications. Child Development, 83(1), 92–103. https://doi.org/10.1111/j.1467-8624.2011.01672.x
Burrell, L., Crowne, S., Ojo, K., Snead, R., O’Neill, K., Cluxton-Keller, F., & Duggan, A. (2018). Mother and home visitor emotional well-being and alignment on goals for home visiting as factors for program engagement. Maternal and Child Health Journal, 22(1), 43–51. https://doi.org/10.1007/s10995-018-2535-9
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. Retrieved from https://pdfs.semanticscholar.org/bed9/2e978f5bca851a79b16d8499b8ca21eeb3d6.pdf
Cooper, P. J., Tomlinson, M., Swartz, L., Landman, M., Molteno, C., Stein, A., Mc Pherson, K., & Murray, L. (2009). Improving quality of mother-infant relationship and infant attachment in socioeconomically deprived community in South Africa: Randomised controlled trial. BMJ (clinical Research Ed.), 338, b974. https://doi.org/10.1136/bmj.b974
de Souza, N., Sardessai, V., Joshi, K., Joshi, V., & Hughes, M. (2006). The determinants of compliance with an early intervention programme for high-risk babies in India. Child Care and Health Development, 32(1), 63–72. https://doi.org/10.1111/j.1365-2214.2006.00576.x
Eisner, M., & Meidert, U. (2011). Stages of parental engagement in a universal parent training program. Jornal Primary Prevention, 32, 83–93. https://doi.org/10.1007/s10935-011-0238-8
Engle, P. L., Black, M. M., Behrman, J. R., de Mello, M., Gertler, P. J., Kapiriri, L., Martorell, R., & Young, M. E. (2007). Strategies to avoid the loss of developmental potential in more than 200 million children in the developing world. Lancet, 369(9557), 229–242. https://doi.org/10.1016/S0140-6736(07)60112-3
Feldman, R. (1998). Coding interactive behavior (CIB). Bar-Ilan University.
Filgueiras, A., Pires, P., Maissonette, S., & Landeira-Fernandez, J. (2013). Psychometric properties of the Brazilian-adapted version of the ages and stages questionnaire in public child daycare centers. Early Human Development, 89, 561–576. https://doi.org/10.1016/j.earlhumdev.2013.02.005
Fox, S. E., Levitt, P., & Nelson, C. A. (2010). How the timing and quality of early experiences influence the development of brain architecture. Child Development, 81(1), 28–40. https://doi.org/10.1111/j.1467-8624.2009.01380.x
Frankenburg, W. K., Dodds, J., Archer, P., Shapiro, H., & Bresmck, B. (1992). The Denver II: A major revision and restandardization of the denver developmental screening test. Pediatrics, 89(1), 91–97.
Fundação Maria Cecilia Souto Vidagal. (2017). Primeiríssima infância creche: necessidades e interesses de famílias e crianças. Fundação Maria Cecilia Souto Vidigal.
Fundação Maria Cecilia Souto Vidagal. (2013). Primeiríssima Infância da gestação aos três anos Percepções e práticas da sociedade brasileira sobre a fase inicial da vida. Fundação Maria Cecilia Souto Vidigal.
Galinsky, E. (2010). Mind in the making. The seven essential life skills every child needs. Harperstudio.
Ginsburg, K. R. (2007). The importance of play in promoting healthy child development and maintaining strong parent-child bond. Pediatrics, 119(1), 182–191. https://doi.org/10.1542/peds.2011-2953
Girvin, H., DePanfilis, D., & Daining, C. (2007). Predicting program completion among families enrolled in a child neglect preventive intervention. Research on Social Work Practice, 17(6), 674–685. https://doi.org/10.1177/1049731507300285
Grantham-McGregor, S., Cheung, Y. B., Cueto, S., Glewwe, P., Richter, L., & Strupp, B. (2007). Developmental potential in the first 5 years for children in developing countries. The Lancet, 369, 60–70. https://doi.org/10.1016/S0140-6736(07)60032-4
Guttentag, C. L., Landry, S. H., Williams, J. M., Baggett, K. M., Noria, C. W., Borkowski, J. G., Swank, P. R., Farris, J. R., Crawford, A., Lanzi, R. G., Carta, J. J., Warren, S. F., & Ramey, S. L. (2014). “My Baby & Me”: Effects of an early, comprehensive parenting intervention on at-risk mothers and their children. Developmental Psychology, 50(5), 1482–1496. https://doi.org/10.1037/a0035682
Harris, M., Andrews, K., Gonzalez, A., Prime, H., & Atkinson, L. (2020). Technology-assisted parenting interventions for families experiencing social disadvantage: A meta-analysis. Prevention Science: The Official Journal of the Society for Prevention Research, 21(5), 714–727. https://doi.org/10.1007/s11121-020-01128-0
Heckman, J. J. (2006). Skill formation and the economics of investing in disadvantaged children. Science, 312, 1900–1902. https://doi.org/10.1126/science.1130121
Jeong, J., Franchett, E. E., Ramos de Oliveira, C. V., Rehmani, K., & Yousafzai, A. K. (2021). Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS Medicine, 18(5), e1003602. https://doi.org/10.1371/journal.pmed.1003602
Jeong, J., Pitchik, H. O., & Yousafzai, A. K. (2018). Stimulation interventions and parenting in low- and Middleincome countries: A meta-analysis. Pediatrics, 141(4), e20173510. https://doi.org/10.1542/peds.2017-3510
Kochanska, G., Kim, S., Boldt, L. J., & Nordling, J. K. (2013). Promoting toddlers’ positive social-emotional outcomes in low-income families: A play-based experimental study. Journal of Clinical Child and Adolescent Psychology, 42(5), 700–712. https://doi.org/10.1080/15374416.2013.782815
Linhares, M.B.M., & Gaspardo, C.M. (2017). Tradução da versão do instrumento adaptada pelo FOI, autorizada pelo autor. Versão original: Gibaud-Wallston, J., & Wandersman, L. P. (1978). Development and utility of the Parenting Sense of Competence Scale. Paper presented at the anual meeting of the American Psychological Association, Toronto.
Lu, C., Black, M. M., & Richter, L. M. (2016). Risk of poor development in young children in low-income and middle-income countries: An estimation and analysis at the global, regional, and country level. The Lancet Global Health, 4(12), e916–e922. https://doi.org/10.1016/S2214-109X(16)30266-2
Luft, C. D. B., Sanches, S. O., Mazo, G. Z., & Andrade, A. (2007). Versão brasileira da Escala de Estresse Percebido: Tradução e validação para idosos. Revista De Saúde Pública, 41(4), 606–615.
McCoy, D. C., Peet, E. D., Ezzati, M., Danaei, G., Black, M. M., Sudfeld, C. R., Fawzi, W., & Fink, G. (2016). Early childhood developmental status in low- and middle-income countries: National, regional, and global prevalence estimates using predictive modeling. PLoS Medicine, 13(6), e1002034. https://doi.org/10.1371/journal.pmed.1002034
McGillion, M., Pine, J. M., Herbert, J. S., & Matthews, D. (2017). A randomised controlled trial to test the effect of promoting caregiver contingent talk on language development in infants from diverse socioeconomic status backgrounds. Journal of Child Psychology and Psychiatry, 58(10), 1122–1131. https://doi.org/10.1111/jcpp.12725
Moreno, M. A. (2016). Supporting child play. JAMA Pediatrics, 170(2), 184. https://doi.org/10.1001/jamapediatrics.2015.2505
Murray, L., De Pascalis, L., Tomlinson, M., Vally, Z., Dadomo, H., MacLachlan, B., Woodward, C., & Cooper, P. J. (2016). Randomized controlled trial of a book-sharing intervention in a deprived South African community: Effects on carer-infant interactions, and their relation to infant cognitive and socioemotional outcome. Journal of Child Psychology and Psychiatry, 57(12), 1370–1379. https://doi.org/10.1111/jcpp.12605
Nieuwboer, C. C., Fukkink, R. G., & Hermanns, J. M. A. (2013). Online programs as tools to improve parenting: A meta-analytic review. Child and Youth Services Review, 35, 1823–1829. https://doi.org/10.1016/j.childyouth.2013.08.008
Ohan, J. L., Leung, D. W., & Johnston, C. (2000). The parenting sense of competence scale: Evidence of a stable factor structure and validy. Canadian Journal of Behavioural Science, 32(4), 251–261. https://doi.org/10.1037/h0087122
Pontoppidan, M., Klest, S. K., & Sandoy, T. M. (2016). The incredible years parents and babies program: a pilot randomized controlled trial. PLoS One, 11(12), e0167592. https://doi.org/10.1371/journal.pone.0167592
Popp, J. M., & Thomsen, B. S. (2017). A commentary on the importance of father–child play and children’s development. Infant Mental Health Journal, 38(6), 785–788. Retrieved from https://onlinelibrary.wiley.com/doi/abs/https://doi.org/10.1002/imhj.21681
Rayce, S. B., Rasmussen, I. S., Klest, S. K., Patras, J., & Pontoppidan, M. (2017). Effects of parenting interventions for at-risk parents with infants: a systematic review and meta-analyses. BMJ OPEN, 7, 12. https://doi.org/10.1136/bmjopen-2016-015707
REDCap. (2018). REDCap. https://redcap.hc.fm.usp.br/
Rede Nossa São Paulo. (2019). Mapa da desigualdade 2019. Retrieved from https://www.nossasaopaulo.org.br/wp-content/uploads/2019/11/Mapa_Desigualdade_2019_tabelas.pdf
Sawyer, M. G., Reece, C. E., Bowering, K., Jeffs, D., Sawyer, A. C. P., Mittinty, M., & Lynch, J. W. (2017). Nurse-moderated internet-based support for new mothers: Non-inferiority, randomized controlled trial. Journal of Medicine Internet Research, 19(7), 1–14. https://doi.org/10.2196/jmir.6839
Shah, R., Isaia, A., Schwartz, A., & Atkins, M. (2019). Encouraging parenting behaviors that promote early childhood development among caregivers from low-income urban communities: A randomized static group comparison trial of a primary care-based parenting program. Maternal and Child Health Journal, 23(1), 39–46. https://doi.org/10.1007/s10995-018-2589-8
Shah, R., Kennedy, S., Clark, M. D., Bauer, S. C., & Schwartz, A. (2016). Primary care-based interventions to promote positive parenting behaviors: A meta-analysis. Pediatrics, 137(5), e20153393. https://doi.org/10.1542/peds.2015-3393
Shonkoff, J. P. (2012). Leveraging the biology of adversity to address the roots of disparities in health and development. Proceedings of the National Academy of Sciences of the United States of America, 109(Suppl. 2), 17302–17307. https://doi.org/10.1073/pnas.1121259109
Shonkoff, Jack P, & Phillips, D. A. (2000). From Neurons to Neighborhoods: The Science of Early Childhood Development. Retrieved from http://www.nap.edu.
Solís-Cordero, K., Duarte, L. S., & Fujimori, E. (2022). Effectiveness of remotely delivered parenting programs on caregiver-child interaction and child development: A systematic review. Journal of Child and Family Studies. https://doi.org/10.1007/s10826-022-02328-8
Solís-Cordero, K., Lerner, R., Marinho, P., Camargo, P., Takey, S., & Fujimori, E. (2021). Overcoming methodological challenges due to COVID-19 pandemic in a non-pharmacological caregiver-child randomly controlled trial. International Journal of Social Research Methodology. https://doi.org/10.1080/13645579.2021.1933067
Unidos pelo brincar. (2021). O brincar nas favelas brasileiras. Retrieved from: http://aliancapelainfancia.org.br/wp-content/uploads/2021/05/Pesquisa-Brincar-nas-Favelas-Brasileiras-deck-Webinar-Direito-do-Brincar.pptx-2.pdf
Vally, Z., Murray, L., Tomlinson, M., & Cooper, P. J. (2015). The impact of dialogic book-sharing training on infant language and attention: A randomized controlled trial in a deprived South African community. Journal of Child Psychology and Psychiatry, 56(8), 865–873. https://doi.org/10.1111/jcpp.12352
Weisleder, A., Mazzuchelli, D. S. R., Lopez, A. S., Neto, W. D., Cates, C. B., Goncalves, H. A., Fonseca, R. P., Oliveira, J., & Mendelsohn, A. L. (2018). Reading aloud and child development: A cluster-randomized trial in Brazil. Pediatrics, 141, 1. https://doi.org/10.1542/peds.2017-0723
World Health Organization. (2018). Nurturing care for early childhood development: a framework for helping children survive and thrive to transform health and human potential. Switzerland; 2018. Retrieved from: https://apps.who.int/iris/bitstream/handle/10665/272603/9789241514064-eng.pdf?ua=1
World Health Organization. (1997). Improving Mother/child Interaction To Promote Better Psychosocial Development in Children. 1997. Retrieved from https://www.who.int/mental_health/media/en/29.pdf
Yogman, M., Garner, A., Hutchinson, J., Hirsh-Pasek, K., & Golinkoff, R. M. (2018). The power of play: A pediatric role in enhancing development in young children. Pediatrics, 142(3), e20182058. https://doi.org/10.1542/peds.2018-2058
Yousafzai, A. K., Obradovic, J., Rasheed, M. A., Rizvi, A., Portilla, X. A., Tirado-Strayer, N., Siyal, S., & Memon, U. (2016). Effects of responsive stimulation and nutrition interventions on children’s development and growth at age 4 years in a disadvantaged population in Pakistan: A longitudinal follow-up of a cluster-randomised factorial effectiveness trial. The Lancet. Global Health, 4(8), e548–e558. https://doi.org/10.1016/S2214-109X(16)30100-0
Acknowledgements
The authors would like to thank the children and caregivers who generously participated in this study. Taís Coppini Pereira e Lucas Ferreria for all the administrative and logistical work to carry out the study. The examiners who participated in the data collection and analysis of the videos. Dr. Leila Larson for her valuable contributions to the manuscript.
Funding
This study was financed by Núcleo Ciência pela Primeira Infãncia.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflicts of interest to disclose.
Ethical Approval
The study received approval from the Fundação José Luiz Egydio Setubal de São Paulo Human Ethics Committee (CAAE: 09941319.1.0000.5567). The trial was registered with The Brazilian Clinical Trials Registry, number RBR-10c27qjq, “retrospectively registered”.
Consent to Participate
All caregivers provided written informed consent (or thumbprint) at the time of the baseline data collection.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The trial was registered with The Brazilian Clinical Trials Registry, number RBR-10c27qjq, “retrospectively registered”.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Solís-Cordero, K., Marinho, P., Camargo, P. et al. Effects of an Online Play-Based Parenting Program on Child Development and the Quality of Caregiver-Child Interaction: A Randomized Controlled Trial. Child Youth Care Forum 52, 935–953 (2023). https://doi.org/10.1007/s10566-022-09717-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10566-022-09717-6