
Abstract
Aim
An evidence gap exists on sex and gender differences in drowning with previous research neglecting females. Drowning studies have largely focused on accidental drowning and submersion, excluding other classifications such as intentional, water transport-related, and undetermined drowning. This study examined all external causes of drowning deaths over a 13-year period in Australia disaggregated by sex. Drowning deaths were compared by sex with drowning classification, year, month, age, place of death, Indigenous status, socioeconomic, and visitor status.
Subject and methods
This retrospective total population study included all females and males who died from drowning in Australia from 2006 to 2019. Data was extracted from the Australian Bureau of Statistics Cause of Death Unit Record Files. Australian population data were extracted to calculate the crude death rate and relative risk for drowning.
Results
There were 4007 drowning deaths recorded, and females represented 25.2% of drowning fatalities. Females were less likely than males to drown, including by drowning classification, year, month, state, remoteness and visitor status, age, socioeconomic, and Indigenous status. The highest proportion of female drowning deaths were from intentional drowning, fall into swimming pools, and in natural water. Drowning deaths among females increased as age increased.
Conclusion
There is a clear need for improved disaggregation of sex and gender in drowning research. Without the detailed exploration of females in drowning statistics there will be limited knowledge translation specific to females. The development of drowning prevention strategies targeted to females is required to reduce the incidence and risk of drowning.
Similar content being viewed by others


Introduction
Drowning is a preventable cause of injury within the international community (World Health Organization 2014). In 2019 there were approximately 236,000 deaths globally from drowning, with 90% of drowning deaths occurring in low- and middle-income countries (LMIC) (World Health Organization 2021). Within high-income countries (HIC), drowning remains a substantial cause of injury and death (Centers for Disease Control and Prevention 2012; Royal Life Saving Society-Australia 2021; Water Safety New Zealand 2018). Drowning is of significant financial cost to the Australian community, with an estimated cost of $85.5 million (USD) annually (World Health Organization 2021). Despite a considerable increase (70%) in the number of drowning publications in the 6-year period to 2020 (Scarr and Jagnoor 2021), a large gap exists in evidence and knowledge on sex and gender differences in the occurrence of drowning, with previous research focusing primarily on males and children, neglecting females (Roberts et al. 2021).
Sex is the biological characteristics of female, male, and intersex people defined by physiological attributes including chromosomes, genes, hormones, and sex anatomy (Wainer et al. 2020). Gender is defined by the social and cultural norms and constructs associated with behaviour and roles that are attributed as female, male, and gender-diverse, in societies (Tannenbaum et al. 2016; Wainer et al. 2020). The lack of representation of sex and gender differences occurs widely in health research, with only 69% of public health studies including sex and/or gender in data (Sugimoto et al. 2019). This is an issue of high importance within drowning research, as sex and gender are rarely disaggregated data in epidemiological and clinical studies (Roberts et al. 2021), and gender plays an influential role in behaviour and risk-taking activities that can lead to a drowning event (Quinton et al. 2022). The three recent National Drowning Reports in Australia (2022, 2021, and 2020) (Royal Life Saving Society-Australia 2020; Royal Life Saving Society-Australia 2021; Royal Life Saving Society-Australia 2022) exemplify this issue, as detailed data are presented only on males, with no inclusion of the description of the impact of drowning on females, despite previous drowning reports (2018 and 2019) including results for females (Royal Life Saving Society-Australia 2018; Royal Life Saving Society-Australia 2019). The total number of drowning deaths in Australia increased by 15% from 2021 to 2022, with females accounting for 18% of drowning deaths in 2022 (Royal Life Saving Society-Australia 2022).
The priority to include sex and gender in research studies has been widely supported, and urgent action is called for to improve the representation of sex and gender in all areas of health research (Gahagan 2016; Gahagan et al. 2015; Gogovor et al. 2021; Heidari et al. 2016; McGregor et al. 2017; Peters and Norton 2018; Sugimoto et al. 2019; Tannenbaum et al. 2016; Wainer et al. 2020). International research committees and academic journals have introduced editorial policies and guidelines calling for the mandatory inclusion of sex and gender comparisons in studies, including complete disaggregation of data by sex and gender (Gahagan 2016; Gogovor et al. 2021; Heidari et al. 2016; McGregor et al. 2017; Tannenbaum et al. 2016; Wainer et al. 2020). Females are widely under-represented in health research, and this needs to be urgently addressed (Mazure and Jones 2015). Unequal representation of females in studies is to the detriment of evidence-based knowledge and research translation (Gahagan et al. 2015; Peters and Norton 2018).
The process for recording data on drowning is identified as problematic by researchers internationally (Bierens and Hoogenboezem 2022; Claesson et al. 2021; Franklin et al. 2020; Scarr et al. 2022). Drowning fatalities are classified utilizing the International Classification of Diseases version 10 codes (ICD-10) (World Health Organization 2016) including accidental drowning and submersion (W65-74), but often other drowning classification codes are excluded from national and international drowning fatality estimates. This includes water transport-related incidents (V90 and V92), intentional self-harm (X71), assault by drowning (X92), and undetermined intent (Y21) (Claesson et al. 2021; Franklin et al. 2020; World Health Organization 2016). This leads to inaccurate estimates of total drowning incidents and the reduced recognition of the impact of morbidity and mortality related to drowning, especially in the clinical setting (Franklin et al. 2020). While some studies have included all ICD-10 drowning classification codes (V90-92, W65-74, X71, X92, Y21) and other relevant codes such as victim of flood (X38) (Bierens and Hoogenboezem 2022; Claesson et al. 2021; World Health Organization 2016), they are limited (Bierens and Hoogenboezem 2022; Claesson et al. 2021). In HICs, it is estimated that up to 50–60% of drowning-related data are not captured, due to the poor reporting on unintentional drowning (W65-74) only (Bierens and Hoogenboezem 2022; Claesson et al. 2021; Peden et al. 2017).
This study aimed to (1) describe external causes of drowning deaths, as the primary or secondary cause of death, over a 13-year period (2006–2019) in Australia, and (2) compare drowning deaths by the sex of victims with drowning classification, year, state, month, age, remoteness, Indigenous status, socioeconomic status, and visitor status.
Subject and methods
Study design
This study was a retrospective, total-population observational study, conducted and reported utilizing the Strengthening of the Reporting of Observational Studies in Epidemiology (STROBE) statement (von Elm et al. 2014).
Setting and participants
All people who died from drowning in Australia from 1 July 2006 to 30 June 2019 were included in the study.
Data collection
Data was extracted from the Australian Bureau of Statistics (ABS) Cause of Death Unit Record File (COD URF) database utilizing the Underlying Cause of Death (UCOD) data (Australian Bureau of Statistics 2019). The COD URF is data that is compiled and coded (ICD-10) by the Australian Bureau of Statistics (ABS), based on data from the National Coronial Information System (NCIS) and the registries of births, deaths and marriages of all states and territories in Australia. All external causes for drowning-related deaths in Australia from 2006 to 2019 were recorded. Data extracted from the COD URF included sex, death year (financial year), month, state/territory, age at death, age group, Index of Relative Socio-economic Advantage and Disadvantage (IRSAD), statistical local area (used to define IRSAD), remoteness, Indigenous status, and visitor status. The ABS Cause of Death database includes data by sex only and did not include data on gender; therefore, only results by sex characteristics have been analysed and presented in this study.
Drowning deaths were classified by the International Classification of Diseases 10th edition (ICD-10-CM) codes as follows (World Health Organization 2016):
-
Accidental drowning and submersion: W65 Drowning and submersion while in bathtub, W66 Drowning and submersion following fall into bathtub, W67 Drowning and submersion while in swimming pool, W68 Drowning and submersion following fall into swimming pool, W69 Drowning and submersion while in natural water, W70 Drowning and submersion following fall into natural water, W73 Other specified drowning and submersion, and W74 Unspecified drowning and submersion.
-
Intentional drowning: X71 Intentional self-harm by drowning and submersion, and X92 Assault by drowning and submersion.
-
Water transport accidents: V90 Accident to watercraft causing drowning and submersion, and V92 Water-transport-related drowning and submersion without accident to watercraft.
-
Undetermined intent: Y21 Drowning and submersion, undetermined intent.
The drowning classification for deaths was examined by ICD-10 code for primary and secondary cause of death. A total of 186 deaths were recorded with drowning as secondary cause of death under 42 other primary ICD-10 codes, see Appendix 1 (World Health Organization 2016).
Australian population data were extracted to calculate the crude death rate per 100,000 persons and relative risk for drowning. To calculate crude death rates, Australian population data from 2006 to 2019 from ABS and Tourism Research Australia were extracted (Australian Bureau of Statistics 2016a; Australian Bureau of Statistics 2021; Tourism Research Australia 2020). Remoteness and regional areas are defined using the Remoteness Area Structure from the Australian Statistical Geographic Standard based on statistical local area level 2 (SA2) (Australian Bureau of Statistics 2016a). Socio-Economic Indexes for Areas (SEIFA) were based on SA2, with information utilized to interpret IRSAD decile ranking, including low IRSAD (most disadvantaged and least advantaged) to high IRSAD (least disadvantaged and highest advantage) (Australian Bureau of Statistics 2016b). Drowning deaths registered by each state or territory were examined by the number of deaths recorded in the state of residence of the victim, deaths recorded as interstate visitor, or deaths recorded as an international visitor and new arrival.
There were 336 cases with missing data (78 females and 258 males) on IRSAD status, including SA2, 9-digit codes, and deciles on IRSAD status, and were excluded. As population estimates for IRSAD status and remoteness and regional status are based on usual area of residence, a code was not able to be obtained for those from overseas or where usual area of residence is unknown; therefore; the proportion of deaths by sex is presented only. There were missing data for age groups and age at death (one female).
Data with a value less than 5 are not presented due to the risk of identification of the victim and as part of ethics requirements; these data are presented as ‘np’ in tables.
Data analysis
Descriptive statistics were calculated for all variables in this study. Descriptive results are presented as proportion (number) and percentage, mean and standard deviation (SD), and relative risk (RR). The crude death rate was calculated per 100,000 persons using Australian population data. Relative risk was calculated using females as the control group, female crude death rate/male crude death rate. The confidence interval (CI) for RR was calculated with a 95% CI of p<0.05 considered statistically significant. Data analysis was performed using IBM SPSS Statistics version 26.0 software (IBM Corp. 2019).
Ethics
Ethical approval for this study was granted by the Human Research Ethics Committee, James Cook University (H6136).
Results
There were 4007 drowning fatalities recorded in Australia from 2006 to 2019 (Table 1). Females accounted for 25.2% of drowning fatalities. Females were less likely to experience fatality from drowning in Australia in all variables analysed (RR:0.333, 95% CI 0.31-0.358), including drowning classification, year, month, state/territory and visitor status, age, remoteness, socioeconomic status, and Indigenous status. The crude death rate was 0.63 deaths per 100,000 persons for females and 1.88 deaths per 100,000 persons for males.
Drowning classification
The risk of death among females from drowning in a bathtub (W65) (RR:1.346, 95% CI 0.959–1.888), fall into bathtub (W66) (RR:1.070, 95% CI 0.489–2.345), or fall into a swimming pool (W68) (RR:0.706, 95% CI 0.538–0.925) was higher than the overall risk for female deaths for unintentional drowning (RR:0.291, 95% CI 0.265–0.32) (Table 1). The risk for females to die from drowning from water-transport-related incidents was significantly lower (RR:0.149, 95% CI 0.114–0.195) than males, and within the water transport-related classification, females experienced the lowest risk of death from drowning compared to all other drowning classification codes.
The largest proportion of drowning deaths among females was caused by intentional self-harm (X71, n = 247, 24%), drowning and submersion while in natural water (W69, n = 162, 16%), and drowning and submersion from fall into swimming pool (W68, n = 90, 9%). The largest proportion of drowning deaths among males was caused by drowning and submersion while in natural water (W69, n = 924, 31%), intentional self-harm (X71, n = 406, 13%), and following fall into natural water (W70, n = 361, 12%).
Year and month of drowning death
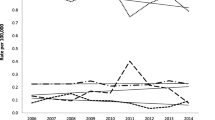
The crude death rate from drowning was highest for females in 2010–2011, and lowest in 2018–2019 (Table 2). Among males, the crude death rate was highest in the years 2009–2010, and lowest in 2017–2018. The crude drowning death rate (per 100,000 persons) for females and males increased in December (females = 0.09, males = 0.23), January (females = 0.08, males = 0.27), and February (females = 0.06, males = 0.19). May to September had the lowest crude death rate from drowning for females (0.03–0.04) and males (0.11).
drowning death rate (per 100,000 persons) for females and males increased in December (females = 0.09, males = 0.23), January (females = 0.08, males = 0.27), and February (females = 0.06, males = 0.19). May to September had the lowest crude death rate for females (0.03–0.04) and males (0.11) from drowning.
Drowning deaths by state and territories
The crude death rate was highest among females who died from drowning in Tasmania and lowest in Victoria (Table 3). The largest proportion of death from a drowning incident among females occurred in New South Wales (NSW) (33%), Queensland (QLD) (23%), and Victoria (17%). Among males, the highest crude death rate from drowning occurred in the Northern Territory and the lowest was in the Australian Capital Territory. The largest proportion of drowning deaths for males by state and territory, was similar to females, occurring in NSW (34%), QLD (24%), and Victoria (16%).
Deaths in state and interstate or international visitor status
Most females (88%, n = 892/1010) and males (85%, n = 2534/2997) died from drowning within their state of residence (Table 3), compared to drowning deaths that occurred as an interstate or international visitor (including new arrivals). The crude death rate from drowning was lowest for deaths that occurred as an interstate visitor among females (0.02 per 100,000 persons) and males (0.07 per 100,000 persons).
Drowning deaths by age group
The crude death rate for females was highest in the 0–4-year age group with the highest death rate occurring among females and males aged 1 and 2 years (Table 4). The crude death rate reduced after 3 years of age for females and males until adulthood. The number of drowning deaths increased as age increased among females from 20 years of age.
Age at death
Females were 1.27 years older at age of death compared to males (Table 5). Age at death was highest for intentional drowning (females = 55.52 years, males = 56.21 years). The largest difference in sex and age at death from drowning occurred in the water transport-related classification, where females were 11.7 years younger than males.
Remoteness and regional status
The largest proportion of drowning deaths among females and males occurred in major cities (%) and inner regional areas (%) of Australia (Table 6). The crude death rate for drowning was highest for females (1.08 per 100,000 persons) and males (3.558 per 100,000 persons) in the very remote areas of Australia.
Socioeconomic status
The highest proportion of drowning deaths, when compared by sex, occurred in the high-IRSAD group for females (27.5%) and low-IRSAD group for males (77.5%) (Table 6). When females and males were analysed separately by sex, the largest number of drowning deaths in the female and male groups occurred in the mid-IRSAD group (females 42%, males 41%).
Aboriginal and/or Torres Strait Islander and non-Indigenous deaths
Aboriginal and/or Torres Strait Islander females were 17% more at risk to die from drowning than non-Indigenous females (RR:1.17, 95% CI 0.847–1.618) (Table 6). Aboriginal and/or Torres Strait Islander males were 21% more at risk to die from drowning than non-Indigenous males (RR: 1.219, 95% CI 1.014–1.465).
Discussion
The examination of drowning deaths in Australia from 2006 to 2019 revealed that females were less likely to die from a drowning incident than males; this is consistent with worldwide data on drowning fatalities (Bessereau et al. 2016; Claesson et al. 2021; Franklin et al. 2020; Tyler et al. 2017). The comparison of drowning deaths in Australia by sex and drowning classification, year and month of death, age, Indigenous status, state/territory, and remoteness, found that females were 67% less likely than males to experience fatality from a drowning incident representing 25% of all drowning fatalities in Australia. The largest number of deaths among females from drowning occurred by intentional drowning, falls into swimming pools, and in natural water. Age was also found to be a risk factor for females as the number of drowning deaths increased as age advanced. This study is important as it is the first time the burden of fatal drownings experienced by females and males in Australia has been examined by all external causes of death, and complete disaggregation of data by sex has been presented and explored. Previously there was limited description regarding females who experience drowning, and females are widely unrepresented in drowning data, creating inequality (Roberts et al. 2021).
Drowning classification
The examination of drowning by primary cause of death and by accidental drowning and submersion (W65-W74) codes only has been recognized for over 20 years as problematic by drowning researchers (Franklin et al. 2020; Lunetta et al. 2002; Smith and Langley 1998). However, recently some publications on drowning have included the ICD-10 codes V90, V92, X71, X92, and Y21, including flood X38, in addition to accidental drowning and submersion W65-W74 (Bierens and Hoogenboezem 2022; Centers for Disease Control and Prevention 2020; Claesson et al. 2021; World Health Organization 2016). In this study, 1530 (38%) drowning deaths were recorded under ICD-10 codes that did not include W65-W74.
A comparison of the Australian drowning deaths by sex and drowning classification found in the current study was made with studies from the United States, Sweden, and the Netherlands (Bierens and Hoogenboezem 2022; Centers for Disease Control and Prevention 2020; Claesson et al. 2021). The crude death rate from drowning when compared by all codes for drowning classification and sex in Australia, from 2006 to 2019, was lower than the United States during the same period by 0.115 (per 100,000 persons) for females and 0.411 for males (Centers for Disease Control and Prevention 2020). The proportion of deaths among females was similar in Australia (25.2%) and the United States (23.9%) (Centers for Disease Control and Prevention 2020). In Sweden and the Netherlands, the proportion of drowning deaths for all drowning classification codes was comparably higher for females at 30.3% in Sweden (Claesson et al. 2021), and 29.7% in the Netherlands (Bierens and Hoogenboezem 2022; Centers for Disease Control and Prevention 2020), compared to Australia.
Intentional drowning (X71) in this study accounted for 16.3% of all drowning deaths for females and males combined. The largest proportion of drowning deaths in females was from intentional drowning, and this result was consistent with two studies from the Netherlands and Ireland where females were found to commit suicide by drowning at higher rates than males (Bierens and Hoogenboezem 2022; Haw and Hawton 2016). Intentional drowning was the second leading cause of death for males in this study. In Ireland, male deaths from intentional drowning were the second leading cause of suicide, highlighting the need to further investigate intentional drownings for both females and males to reduce mortality from this preventable cause of death (Haw and Hawton 2016).
Year and month of death
Death from drowning in this study was highest among females in 2010 to 2011. In these years it is important to note the impact of cataclysmic events in Queensland, New South Wales, and Victoria where widespread flooding occurred, with 48 people dying flood-related deaths (females 42%, males 58%), including 41 deaths in Queensland (Coates 2022). The summer months experienced the highest number of drowning deaths among females and males in Australia (December to February). This is consistent with international studies that have reported a higher number of drowning deaths during their summer months, including studies from Canada (Clemens et al. 2016), France (Bessereau et al. 2016), and New Zealand (Webber et al. 2020).
Place of death
The highest number of drowning deaths in Australia occurred within the state or territory of residence of the victim (females 88%, males 85%). Female and male travelers including domestic interstate visitors (females 0.02, males 0.07) and international visitors (females 0.12, males 0.40) experienced the lowest crude death rate per 100,000 persons from drowning during this period.
Regional and remote status is an important epidemiological factor in drowning in Australia, as the crude death rate increases with remoteness (Taylor et al. 2020). This was also found in this study, with females and males experiencing the highest crude death rate in the very remote areas of Australia. For females, the crude death rate increased by 71% to 1.08 per 1,000,000 persons and increased by 88% among males to 3.55 deaths per 100,000 persons in the very remote areas. This is important to acknowledge as people living in rural and remote in Australia have limited access to emergency medical services and healthcare, and distance for medical retrieval has placed people living in these areas at risk for injury (Dobson et al. 2022; McGrail and Humphreys 2015; Taylor et al. 2020).
Age
The comparison of drowning deaths and age was made with Sweden (Claesson et al. 2021), the Netherlands (Bierens and Hoogenboezem 2022), and Canada (Clemens et al. 2016), although there are some limitations with the study from Canada which only included unintentional drowning and submersion. The incidence of fatality from drowning in the 0–4-year age group was higher among females in Australia compared to Canada (Clemens et al. 2016). There was no difference by sex in the risk of death from drowning among the 0–4-year age group in this study, and males that were 0–4 years of age experienced a higher number of deaths compared to females. Infants are a vulnerable group in drowning, with males known to account for most fatalities (Gaida and Gaida 2016; Wallis et al. 2015b; World Health Organization 2014). The infant mortality rate from drowning remains high in HIC and LMICs despite this age group having been studied extensively in drowning (Gaida and Gaida 2016; Miller et al. 2019).
The incidence of death from drowning among females and males in the 5–19-year age group in Australia was similar to Canada (Clemens et al. 2016). Within the 20–34-year, 35–49-year, 50–64-year, and 65+-year age groups, the number of drowning deaths followed similar patterns among females and males from Australia with Sweden and Canada (Claesson et al. 2021; Clemens et al. 2016). The number of drowning deaths across all age groups was higher among females in Australia compared to females in Canada and was lower in Australia compared to Sweden (Claesson et al. 2021; Clemens et al. 2016). In this study, the largest number of drowning deaths among females occurred within the 65+-year age group, and the number of drowning deaths increased among females as age increased from 35 years, which was similar to the findings in Sweden (Claesson et al. 2021).
The average age of death from drowning in Australia was lower among Australian females and males compared to the Netherlands, females were 11.9 years younger and males were 5.3 years younger at age of death in Australia (Bierens and Hoogenboezem 2022). The largest difference in age of death in this study occurred in the water transport-related classification with females found to be younger than males by 11 years. It is unclear why there exists such a difference in age among females. Males are known to engage in water-transport-related activities more than females and experience a higher rate of death from water-transport-related drowning compared to females (Wilcox-Pidgeon et al. 2019). However, in a recent Australian study, females were found to be more likely to experience fatality from incidents involving jet skis than males, and also engaged in similar alcohol consumption as males while on board water-transport vessels (Wilcox-Pidgeon et al. 2019).
Indigenous status
Drowning deaths were more likely to occur among female (17%) and male (21%) Aboriginal and/or Torres Strait Islanders compared to non-Indigenous females and males in Australia (including Indigenous status not stated). This study also found that the crude death rate was higher among female and male Aboriginal and/or Torres Strait Islander peoples than among non-Indigenous females and males. A previous Australian study reported the drowning risk for Aboriginal and/or Torres Strait Islander children to be 1.44 times higher than for non-Indigenous children, and they were found to be more vulnerable to drowning in remote and rural areas (Wallis et al. 2015a). However, further research is required to understand drowning in Aboriginal and/or Torres Strait Islander peoples (Royal Life Saving Society-Australia 2021; Wallis et al. 2015a).
Socioeconomic status
Socioeconomic status has been previously found in drowning to be related to health outcomes, with a study from the United States reporting an association between lower socioeconomic status and poor health outcomes in drowning (El Sibai et al. 2018). In Australia, the IRSAD measures income, education, employment, housing, and other variables, including family household indexes in a geographical area, but does not relate to individual status (Australian Bureau of Statistics 2016b). In this study, when compared by sex, the largest proportion of females (42%) and males (41%) who died from drowning were from geographical areas indexed as ‘mid-IRSAD’ status. Within these geographical areas, people more commonly experienced a moderate level of socioeconomic advantage and disadvantage, meaning there may be small differences (above or below the national average), such as in income status, employment status, occupational status, housing (owning versus renting), and level of education (Australian Bureau of Statistics 2018). This is another area of drowning research that requires further exploration.
Impact of drowning by sex
This study has presented a review of drowning deaths over a 13-year period in Australia and has included a detailed description of drowning deaths among females. Although males clearly represent the highest number of drowning deaths in Australia, this study has found that females who had died from a drowning incident during this period experienced similar patterns to males in the month of death, place of death (state/territory and regional and remote status), socioeconomic status, and age at death for the drowning classification of accidental drowning and submersion, and intentional drowning. This is the first study on drowning to present detailed results on females.
Drowning is a significant public health issue, and public health research that examines the causal factors by sex and gender can be used to inform gender-specific prevention and health promotion strategies. The impact of socialization and its association with gender and gender-based activities is believed to be influential in the behaviour and risk-taking attitudes and activities among females and males in drowning (Howland et al. 1996); however, it is an area of research that is yet to be fully explored. It is well documented that overall males are more likely to engage in riskier activities compared to females which lead to drowning incidents (Howland et al. 1996; Quinton et al. 2022), such as swimming in open waters (i.e., oceans and rivers), swimming alone, and at night (Howland et al. 1996; Morgan et al. 2009). Males have been found to be more likely to swim outside lifeguard-patrolled areas (Castelle et al. 2018) and to spend a longer amount of time in the water (Morgan et al. 2009), less likely to wear life protective jackets when on board water vessels (Peden et al. 2018a), and likely to ingest alcohol at higher rates than females when engaging in aquatic activities (Peden et al. 2018b); however, this may be changing, with gender differences in alcohol consumption decreasing (Keyes et al. 2019). Although aquatic activities and risk-taking behaviours among females are less documented, the limited evidence on females suggests they may engage in less risk-taking behaviours; for example, females have been found to be more likely to wade and swim in shallower areas rather than in deeper water at beaches compared to males (Morgan et al. 2009). Females have also been found to have had a higher uptake of and engagement in formal swimming programs over a longer time period than males (Howland et al. 1996; Morgan et al. 2009). These are examples of the protective factors among females in aquatic activities that may reduce the risk of drowning. As more studies explore the role of gender and the links with the socialization of gender and drowning risk, this will uncover much-needed gender-specific health promotion strategies that will act to reduce the risk of and burden of drowning experienced by females and males.
When sex and/or gender analysis is not included in public health studies, the opportunities to uncover health risks and health knowledge specific to females are missed, reinforcing the sex and gender bias existing in health research that has largely focused on males (Gahagan 2016; van Hagen et al. 2021). Internationally, researchers have emphasized the important need for both a sex and gender focus to be mainstreamed within the research community (Mazure and Jones 2015; van Hagen et al. 2021). This has particularly affected the public health knowledge and evidence on females who have experienced unequal representation in research studies over many decades (Peters and Norton 2018; van Hagen et al. 2021). This directly affects knowledge translation, as the generalizability of research findings to inform prevention and health promotion strategies is limited when sex and/or gender are not disaggregated (Gahagan et al. 2015; Peters and Norton 2018; van Hagen et al. 2021). The impact of this reduces equity in health decision-making, healthcare and health program planning, and health policy at the local, national, and international levels (van Hagen et al. 2021).
Currently in Australia there are a limited number of health promotion campaigns and programs that specifically target females. Wilcox-Pidgeon and colleagues report on a qualitative evaluation of a drowning prevention campaign involving a swimming skill intervention program which was introduced for older female migrants in Australia, a group which has been identified as high risk for drowning (Wilcox-Pidgeon et al. 2021). Participants in this study reported a range of benefits as a result of engaging in the program (Wilcox-Pidgeon et al. 2021). This included improvements to their physical and mental health, greater confidence in the water and increased health literacy related to drowning risk and water safety for themselves and their families (Wilcox-Pidgeon et al. 2021). Another Australian study assessed the perceived ability of young adults to perform a rescue; determined the level of aquatic rescue knowledge; and measured the effect of an aquatic rescue intervention, and found that a higher proportion of females in the 15–24-year age group had completed water rescue and/or lifeguard training and formal swimming lessons, compared to males (Petrass and Blitvich 2018). The aquatic rescue intervention focused on water rescue and swimming survival skills, and found that the knowledge and practical skills learned were significantly higher among females than among males (Petrass and Blitvich 2018). These studies (Petrass and Blitvich 2018; Wilcox-Pidgeon et al. 2021) highlight the importance of engaging females in swimming and water rescue skill training as a protective factor to reduce the risk of drowning; however, more interventions targeting females are required with ongoing research to evaluate their success and impact.
Limitations
While this study has provided some female-specific knowledge on drowning there are a number of limitations to be acknowledged. The data provided by the ABS was only available for sex and not gender; therefore, the inclusion of gender in the data analysis was not possible. There was also missing data on sex for the variables of socioeconomic status (IRSAD) and age. Population data stratified by sex was not able to be accessed on usual residence overseas or unknown usual residence and IRSAD status; therefore, the results have been presented by proportion only. The risk of bias has to be acknowledged, two authors (KR and RF) completed data analysis and then independently rechecked data analysis and results. A further limitation is that only minimal comparisons of females who had died from drowning could be made with international studies due to the limited research and evidence that exists.
Conclusion
The importance of including sex and/or gender in research to improve health equity for females is gaining attention. In drowning research in particular, there continues to be a clear need for improved disaggregation of sex and gender. This study found that Australian females are vulnerable to the risk of death from drowning particularly in regard to intentional drowning, falls into swimming pools, and in natural water. As their age increased, the number of fatalities from drowning also increased. The development of dedicated drowning prevention and health promotion strategies targeted to females are urgently required to reduce the risk of fatality from drowning. However, without the equal representation and exploration of females in drowning research, knowledge gaps will remain and will continue to hinder program development in this area.
References
Australian Bureau of Statistics (2016a) Australian Statistical Geography Standard (ASGS): Volume 5 - Remoteness structure 17 October 2021. Available from: https://www.abs.gov.au/AUSSTATS/abs@.nsf/Lookup/1270.0.55.005Main+Features1July%202016?OpenDocument. Accessed 18 Aug 2021
Australian Bureau of Statistics (2016b) Census of population and housing: Socio-Economic Indexes for Areas (SEIFA) Australia 2016 17 October 2021. Available from: https://www.abs.gov.au/ausstats/abs@.nsf/mf/2033.0.55.001. Accessed 18 Aug 2021
Australian Bureau of Statistics (2018) Socio-Economic Indexes for Areas (SEIFA) Technical paper. Report No. 2033.0.55.001. Available from: https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/756EE3DBEFA869EFCA258259000BA746/$File/SEIFA%202016%20Technical%20Paper.pdf. Accessed 18 Aug 2021
Australian Bureau of Statistics (2019) Cause of death. Available from: https://www.abs.gov.au/statistics/health/causes-death/causes-death-australia/2019. Accessed 29 Aug 2021
Australian Bureau of Statistics (2021) National, state and territory population: Estimated resident population. Available from: https://www.abs.gov.au/statistics/people/population/national-state-and-territory-population/dec-2021#data-downloads-data-cubes. Accessed 18 Aug 2021
Bessereau J, Fournier N, Mokhtari T, Brun PM, Desplantes A, Grassineau D et al (2016) Epidemiology of unintentional drowning in a metropolis of the French Mediterranean coast: a retrospective analysis (2000-2011). Int J Inj Control Saf Promot 23:317–322. https://doi.org/10.1080/17457300.2015.1047862
Bierens J, Hoogenboezem J (2022) Fatal drowning statistics from the Netherlands – an example of an aggregated demographic profle. BMC Public Health 22:339. https://doi.org/10.1186/s12889-022-12620-3
Castelle B, Brander R, Tellier E, Simonnet B, Scott T, McCarroll J et al (2018) Surf zone hazards and injuries on beaches in SW France. Nat Hazards 93:1317–1335. https://doi.org/10.1007/s11069-018-3354-4
Centers for Disease Control and Prevention (2012) Drowning-United States, 2005-2009 Contract No.: 19. Available from: https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6119a4.htm#:~:text=In%20the%20United%20States%2C%20an,department%20care%20for%20nonfatal%20drowning. Accessed 13 June 2020
Centers for Disease Control and Prevention (2020) Wisqars injury mortality report. Available from: https://www.wisqars.cdc.gov/fatal-reports. Accessed 18 June 2020
Claesson A, Krig A, Jonsson M, Ringh M, Svensson L, Forsberg S et al (2021) Incidence and characteristics of drowning in Sweden during a 15-year period. Resuscitation 162:11–19. https://doi.org/10.1016/j.resuscitation.2021.01.028
Clemens T, Tamim H, Rotondi M, Macpherson AK (2016) A population based study of drowning in Canada. BMC Public Health 16:1–8. https://doi.org/10.1186/s12889-016-3221-8
Coates L (2022) A flood of rain events: how does it stack up with the previous decade?: Risk frontiers [updated 05 July 2022] Available from: https://riskfrontiers.com/insights/flood-rain-events-decade-2011-2022/#:~:text=A%20total%20of%2048%20flood,to%20a%20flash%20flooding%20event. Accessed 15 Sept 2022
Dobson GP, Gibbs C, Poole C, Butson B, Lawton LD, Morris JL et al (2022) Trauma care in the tropics: addressing gaps in treating injury in rural and remote Australia. Rural Remote Health 22. https://doi.org/10.22605/RRH6928
El Sibai R, Bachir R, El Sayed M (2018) Submersion injuries in the United States: Patients characteristics and predictors of mortality and morbidity. Injury 49:543–548. https://doi.org/10.1016/j.injury.2018.02.012
Franklin RC, Peden AE, Hamilton EB, Bisignano C, Castle CD, Dingels ZV et al (2020) The burden of unintentional drowning: global, regional and national estimates of mortality from the Global Burden of Disease 2017 Study. Inj Prev 26:i83–i95. https://doi.org/10.1136/injuryprev-2019-043484
Gahagan J (2016) Commentary on the new sex and gender editorial policy of the Canadian Journal of Public Health. Can J Public Health 107:e140–e141. https://doi.org/10.17269/CJPH.107.5584
Gahagan J, Gray K, Whynacht A (2015) Sex and gender matter in health research: addressing health inequities in health research reporting. Int J Equity Health 14:1–4. https://doi.org/10.1186/s12939-015-0144-4
Gaida FJ, Gaida JE (2016) Infant and toddler drowning in Australia: Patterns, risk factors and prevention recommendations. J Paediatr Child Health 52:923–927. https://doi.org/10.1111/jpc.13325
Gogovor A, Zomahoun HTV, Ekanmian G, Adisso EL, Tardif AD, Khadhraoui L et al (2021) Sex and gender considerations in reporting guidelines for health research: a systematic review. Biol Sex Differ 12:1–11. https://doi.org/10.1186/s13293-021-00404-0
Haw C, Hawton K (2016) Suicide and Self-Harm by Drowning: A Review of the Literature. Arch Suicide Res 20:95–112. https://doi.org/10.1080/13811118.2015.1025120
Heidari S, Babor TF, De Castro p, Tort S, Curno M (2016) Sex and Gender Equity in Research: rationale for the SAGER guidelines and recommended use. Res Integrity Peer Rev 1:1-9. https://doi.org/10.1186/s41073-016-0007-6.
Howland J, Hingson R, Mangione TW, Bell N, Bak S (1996) Why are most drowning victims men? Sex differences in aquatic skills and behaviors. Am J Public Health 86:93–96. https://doi.org/10.2105/AJPH.86.1.93
IBM Corp. (2019) IBM SPSS Statistics for Windows, Version 26.0. IBM Corp, Armonk, NY
Keyes KM, Jager J, Mal-Sarkar T, Patrick ME, Rutherford C, Hasin D (2019) Is There a Recent Epidemic of Women's Drinking? A Critical Review of National Studies. Alcohol Clin Exp Res 43:1344–1359. https://doi.org/10.1111/acer.14082
Lunetta P, Penttila A, Sajantila A (2002) Drowning in Finland: ‘‘external cause’’ and ‘‘injury’’ codes. Inj Prev 8:342–344. http://injuryprevention.bmj.com/. Accessed 08 Sept 2022
Mazure CM, Jones DP (2015) Twenty years and still counting: including women as participants and studying sex and gender in biomedical research. BMC Womens Health 15. https://doi.org/10.1186/s12905-015-0251-9
McGrail MR, Humphreys JS (2015) Spatial access disparities to primary health care in rural and remote Australia. Geospat Health 10:138–143. https://doi.org/10.4081/gh.2015.358
McGregor AJ, Beauchamp GA, Wira CR, Perman SM, Safdar B (2017) Sex as a bilogical variable in emergency medicine research and clinical practice: A brief narrative review. West J Emerg Med 18:1079–1090. https://doi.org/10.5811/westjem.2017.8.34997
Miller L, Alele FO, Emeto TI, Franklin RC (2019) Epidemiology, risk factors and measures for preventing drowning in Africa: A systematic review. Medicina 55:1–25. https://doi.org/10.3390/medicina55100637
Morgan D, Ozanne-Smith J, Triggs T (2009) Self-reported water and drowning risk exposure at surf beaches. Australian & New Zealand J Public Health 33:180–188. https://doi.org/10.1111/j.1753-6405.2009.00367.x
Peden AE, Franklin RC, Mahony AJ, Scarr J, Barnsley PD (2017) Using a retrospective cross-sectional study to analyse unintentional fatal drowning in Australia: ICD-10 coding-based methodologies verses actual deaths. BMJ Open 7:e019407. https://doi.org/10.1136/bmjopen-2017-019407
Peden AE, Demant D, Hagger MS, Hamilton K (2018a) Personal, social, and environmental factors associated with lifejacket wear in adults and children: A systematic literature review. PLoS ONE [Electronic Resource] 13:e0196421. https://doi.org/10.1371/journal.pone.0196421
Peden AE, Franklin RC, Leggat PA (2018b) Breathalysing and surveying river users in Australia to understand alcohol consumption and attitudes toward drowning risk. BMC Public Health 18. https://doi.org/10.1186/s12889-018-6256-1
Peters SAE, Norton R (2018) Sex and gender reporting in global health: new editorial policies. BMJ Glob Health 3:e001038. https://doi.org/10.1136/bmjgh-2018-001038
Petrass LA, Blitvich JD (2018) A lack of aquatic rescue competency: a drowning risk factor for young adults involved in aquatic emergencies. J Community Health 43:688–693. https://doi.org/10.1007/s10900-018-0472-6
Quinton J, Giles AR, Rich K (2022) Missing masculinities: The need for gender transformative approaches in water safety promotion for men. Health Promot J Austr 33:148–150. https://doi.org/10.1002/hpja.490
Roberts K, Thom O, Devine S, Leggat PA, Peden AE, Franklin RC (2021) A scoping review of female drowning: an underexplored issue in five high-income countries. BMC Public Health 21:1072. https://doi.org/10.1186/s12889-021-10920-8
Royal Life Saving Society-Australia (2018) Royal life saving national drowning report 2018. Sydney, Australia. Available from: https://www.royallifesaving.com.au/__data/assets/pdf_file/0006/32685/RLS_NDR2018_ReportLR.pdf. Accessed 13 Oct 2022
Royal Life Saving Society-Australia (2019) Royal life saving national drowning report 2019. Report. Sydney, Australia. Available from: https://www.royallifesaving.com.au/__data/assets/pdf_file/0005/32684/rlssa-ndr-2019-digital.pdf. Accessed 13 Oct 2022
Royal Life Saving Society-Australia (2020) Royal life saving national drowning report 2020. Sydney, Australia. Available from: https://www.royallifesaving.com.au/__data/assets/pdf_file/0003/33861/RLS_NationalDrowningReport2020LR-FINAL.pdf. Accessed 13 Oct 2022
Royal Life Saving Society-Australia (2021) Royal life saving national drowning report 2021. Sydney, Australia. Available from: https://www.royallifesaving.com.au/__data/assets/pdf_file/0007/50110/RLS_NationalDrowningReport2021_LR.pdf. Accessed 13 Oct 2022
Royal Life Saving Society-Australia (2022) Royal life saving national drowning report 2022. Sydney, Australia. Available from: https://www.royallifesaving.com.au/__data/assets/pdf_file/0007/67687/RLS_NationalDrowningReport2022_SPG_LR.pdf. Accessed 13 Oct 2022
Scarr JP, Jagnoor J (2021) Mapping trends in drowning research: A bibliometric analysis 1995–2020. Int J Environ Res Public Health 18:1–14. https://doi.org/10.3390/ijerph18084234
Scarr JP, Buse K, Norton R, Meddings DR, Jagnoor J (2022) Tracing the emergence of drowning prevention on the global health and development agenda: a policy analysis. Lancet Glob Health 10:E1058–E1066. https://doi.org/10.1016/S2214-109X(22)00074-2
Smith GS, Langley JD (1998) Drowning surveillance: how well do E codes identify submersion fatalities. Inj Prev 4:135–139. https://doi.org/10.1136/ip.4.2.135
Sugimoto CR, Ahn JY, Smith E, Macaluso B, Lariviere V (2019) Factors affecting sex-realted reporting in medical research: a cross-disciplinary bibliometric analysis. Lancet 393:550–559. https://doi.org/10.1016/S0140-6736(18)32995-7
Tannenbaum C, Greaves L, Graham ID (2016) Why sex and gender matter in implementation research. BMC Med Res Methodol 16:145. https://doi.org/10.1186/s12874-016-0247-7
Taylor DH, Peden AE, Franklin RC (2020) Next steps for drowning prevention in rural and remote Australia: A systematic review of the literature. Australian J Rural Health 28:530–542. https://doi.org/10.1111/ajr.12674
Tourism Research Australia (2020) Summation options by type of traveller, stopover interstate/intrastate and age group by stopover state/region, years ending and gender 05 February 2022. Available from: https://www.tra.gov.au/. Accessed 18 Aug 2022
Tyler MD, Richards DB, Reske-Nielsen C, Saghafi O, Morse EA, Carey R et al (2017) The epidemiology of drowning in low- and middle-income countries: a systematic review. BMC Public Health 17:413. https://doi.org/10.1186/s12889-017-4239-2
van Hagen LJ, Muntinga M, Appleman Y, Verdonk P (2021) Sex and gender-sensitive public health research: an analysis of research proposals in a research institute in the Netherlands. Women Health 61:109–119. https://doi.org/10.1080/03630242.2020.1834056
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzche P, Vandenbroucke JP (2014) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int J Surg 12:1495–1499. https://doi.org/10.1016/j.ijsu.2014.07.013
Wainer Z, Carcel C, Hickey M, Schiebinger L, Schmiede A, McKenzie B et al (2020) Sex and gender in health research: updating policy to reflect evidence. Med J Aust 212:57–62. https://doi.org/10.5694/mja2.50426
Wallis BA, Watt K, Franklin RC, Kimble RM (2015a) Drowning in Aboriginal and Torres Strait Islander children and adolescents in Queensland (Australia). BMC Public Health 15:1–11. https://doi.org/10.1186/s12889-015-2137-z
Wallis BA, Watt K, Franklin RC, Nixon JW, Kimble RM (2015b) Drowning mortality and morbidity rates in children and adolescents 0-19 yrs: a population-based study in Queensland, Australia. PLoS One 10:e0117948. https://doi.org/10.1371/journal.pone.0117948
Water Safety New Zealand (2018) Drowning report. Report. Available from: http://drowningreport.watersafety.org.nz/. Accessed 20 Oct 2021
Webber J, Moran K, French C, Fozard F, Pearless O (2020) Fatal costal drowning incidents: A 10-year review of body recovery times in New Zealand. Forensic Sci Int 317. https://doi.org/10.1016/j.forsciint.2020.110573
Wilcox-Pidgeon S, Peden AE, Franklin RC, Scarr J (2019) Boating-related drowning in Australia: Epidemiology, risk factors and the environment. J Saf Res 70:117–125. https://doi.org/10.1016/j.jsr.2019.06.005
Wilcox-Pidgeon S, Franklin RC, Devine S, Leggat PA, Scarr J (2021) Reducing inequities among adult female migrants at higher risk for drowning in Australia: The value of swimming and water safety programs. Health Promot J Austr 32:49–60. https://doi.org/10.1002/hpja.407
World Health Organization (2014) Global report on drowning: preventing a leading killer. Geneva, Switzerland. Available from: https://www.who.int/publications/i/item/global-report-on-drowning-preventing-a-leading-killer. Accessed 08 Aug 2022
World Health Organization (2016) International statistical classification of diseases and related health problems 10th revision 18 June 2021. Available from: https://www.who.int/classifications/icd/en/. Accessed 04 Apr 2022
World Health Organization (2021) Drowning. [Fact Sheet]: World Health Organization [29 March 2022]. Available from: https://www.who.int/news-room/fact-sheets/detail/drowning. Accessed 08 Aug 2022
Acknowledgements
The authors wish to thank the Australian Bureau of Statistics, the State and Territory Registries of Births, Deaths and Marriages, the State and Territory Coroners, and the National Coronial Information System for enabling CODURF data to be used for this publication. The authors would like to acknowledge the Australian Government Research Training Program Scholarship, and the College of Public Health, Medical and Veterinary Sciences, James Cook University.
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
This study was performed in line with the principles of the Declaration of Helsinki. Ethical approval for this study was granted by the Human Research and Ethics Committee, James Cook University (H6136) on 22 April 2015.
Conflict of interest/Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendices
Appendix 1
ICD-10 codes (World Health Organization 2016) - Secondary cause of drowning death
C50 - Malignant neoplasm, breast
D68 - Coagulation defect
F10 - Mental and behavioural disorders due to use of alcohol, acute intoxication/psychotic disorder, dependent syndrome
F32 - Depressive episode
G20 - Parkinson disease
G40 - Epilepsy
G80 - Cerebral palsy
G93 - Encephalopathy
I08 - Multiple valve diseases
I11 - Hypertensive heart disease
I21 - Acute myocardial infarction
I25 - Chronic ischaemic heart disease
I46 - Cardiac arrest
I51 - Complications and ill-defined descriptions of heart disease
I69 - Sequelae of cerebrovascular disease
J43 - Emphysema
Q07 - Other congenital malformations of nervous system
Q85 - Phakomatoses, not elsewhere classified
V43 - Car occupant injured in collision with car
V47 - Car occupant injured in collision with fixed or stationary object
V48 - Car occupant injured in non-collision transport accident
W12 - Fall on and from scaffolding, industrial and construction area
W13 - Fall from, out of or through building or structure
W15 - Fall from cliff
W58 - Bitten or struck by crocodile or alligator
W78 - Inhalation of gastric contents
X31 - Exposure to excessive natural cold
X37 - Victim of cataclysmic storm
X38 - Victim of flood
X41 - Accidental poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified
X44 - Accidental poisoning by and exposure to other and unspecified drugs, medicaments, and biological substances
X61 - Intentional self-poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified
X64 - Intentional self-poisoning by and exposure to other and unspecified drugs, medicaments, and biological substances
X65 - Intentional self-poisoning by and exposure to alcohol
X78 - Intentional self-harm by sharp object
X80 - Intentional self-harm by jumping from a high place
Y00 - Assault blunt object
Y11 - Poisoning by and exposure to antiepileptic, sedative-hypnotic, antiparkinsonism and psychotropic drugs, not elsewhere classified, undetermined intent, home
Y14 - Poisoning by and exposure to other and unspecified drugs, medicaments and biological substances, undetermined intent
Y20 - Hanging, strangulation and suffocation, undetermined intent
Y87 - Sequelae of intentional self-harm
Appendix 2
Table 7
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Roberts, K., Thom, O., Devine, S. et al. A focus on sex differences in drowning deaths in Australia: the need for reporting on sex and gender in drowning research. J Public Health (Berl.) (2023). https://doi.org/10.1007/s10389-023-01931-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s10389-023-01931-3